
Introduction
Hepatocelluar carcinoma(HCC) is a primary malignant disease derived from liver cells. HCC is one of the most common digestive cancers worldwide and the third most common cause of cancer related death in the Asia-Pacific region [1]. In China, HCC is the second most common cancer after lung cancer. The treatments options for HCC includes hepatectomy, liver transplantation, local ablative therapy, chemotherapy and molecular targeted therapies [2]. The hepatectomy and liver transplantation are considered to be the curative therapies, however, HCC is usually diagnosed at advanced stage when the application of curative treatments seems to be of little value [3, 4]. For intermediate HCC identified by the Barcelona Clinic Liver Cancer (BCLC) staging system, the local-regional therapies including trans-catheter arterial chemoembolization (TACE), radiofrequency ablation (RFA), and percutaneous ethanol injection (PEI) are suggested as the optimal treatments [5, 6]. These methods have been shown to prolong survival and treatment response for patients, particularly TACE [7-9].
TACE delivers chemotherapeutic agents to the cancer location while blocking the blood supply supporting the growth of tumor [10]. However, the 3-year survival rate is only about 20% due to the complex recurrence mechanisms of HCC. One of them is believed to be angiogenesis caused by vascular endothelial growth factor(VEGF) [11]. It is reported that the elevated levels of VEGF and other angiogenic factors secreted by the hypoxic tumor cells after TACE has the role of promoting abnormal angiogenesis [11]. Indeed, by targeting VEGF, platelet derived growth factor receptor, and other signaling, anti-angiogenesis agents proved to block tumor development and neo-angiogenesis [12, 13].
In recent years, several molecular targeted agents inhibiting the process of angiogenesis have been introduced into clinical practice and show effective results [14]. Thalidomide is not only capable of inhibiting angiogenesis, but also modulating immunity [15, 16]. Thalidomide alone or in combination with other regimen has been widely used in treating cancers such as multiple myeloma [17, 18], HCC [4, 19], lung cancer [20], and bladder cancer [21]. With regards to HCC, many clinical retrospective studies or RCTs [3, 19, 22-29] evaluated the effect of adding thalidomide to TACE on patients with primary HCC, and the results of most of these studies are positive. Patients treated with thalidomide and TACE have a better clinical response and survival than TACE alone. However, these evidences are lack of powerful convincing as the samples of these studies are relatively small. Besides, whether the use of thalidomide in combination with TACE has a better clinical efficacy in patients with intermediate or advanced HCC, there is no final conclusion.
With the concern mentioned above, we systematically identified clinical studies on the topic of thalidomide with TACE for treating HCC, extracted data and conducted this meta-analysis to evaluate the efficacy and safety of thalidomide when combined with TACE, aimed to provide evidence for supporting administration of thalidomide in HCC patients treated with TACE.
Results
Results of literature research and baseline characteristics of included studies
After systematically retrieving in selected databases, a total of 401 articles were identified. 203 records were left after duplicates removed. 165 of them were discarded after reviewing the title and abstract. The full-text of the left 38 studies were further reviewed and 15 of them were excluded. Finally, 23 clinical studies [30-52] including 1836 patients with primary HCC were included. There were 904 cases in the thalidomide combined with TACE group and 932 cases in the TACE group. The overall process of study selection is presented in Figure 1.
The baseline characteristics of included studies are listed in Table 1. Most of the eligible studies did not report the method of blinding. All of the studies were on the topic of efficacy and safety of thalidomide combined with TACE versus TACE alone in intermediate or advanced primary HCC patients. The age and sex distribution were similar in both groups. All of the included trials were performed in China. The dose of thalidomide and cycle of TACE were in accordance within these studies. The regimen of TACE were similar between different studies. The studies of Yun-xiao Lin, et al. [36, 40] and Chang-nan Chen, et al. [36] reported more cases than other studies. All of the included studies reported the therapeutic effects of thalidomide according to the mRECIST criteria. The ORR and DCR were defined as (cases of CR plus PR)/total cases and (cases of CR, PR, and SD)/total cases, respectively. All of the studies reported ethics and written consent during treatments. The concentrations of VEGF and AFP were reported to be tested by Enzyme-linked immuno sorbent assay(ELISA) test in included studies. The parameters of cellular immunity were tested by flow cytometry and analyzed by CellQuest in included studies.
Table 1: Baseline characteristics of included studies
Studies |
N |
Sex |
Age |
Interventions |
Outcomes |
||||
T |
C |
Male |
Female |
T |
C |
T |
C |
||
Wei-sheng Zheng-1, 2007 |
15 |
15 |
27 |
3 |
21-70 |
21-69 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
QOL, IF, TNF-a, |
Wei-sheng Zheng-2, 2007 |
15 |
15 |
27 |
3 |
21-70 |
21-69 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
QOL, IF, TNF-a, |
Hai-lan Lin, 2007 |
32 |
31 |
53 |
10 |
22-75 |
22-75 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
VEGF |
Ming-zhi Hao, 2007 |
45 |
51 |
86 |
10 |
22-75 |
22-75 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
SR |
Xiao-jun Qi, 2007 |
34 |
34 |
48 |
20 |
30-83 |
30-83 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
VEGF |
Xiu-fang Liu, 2007 |
40 |
58 |
62 |
36 |
36-70 |
36-70 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, SR, AE |
Chang-nan Chen, 2008 |
62 |
60 |
106 |
16 |
18-82 |
18-82 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, SR, AE |
Long Feng, 2008 |
15 |
20 |
28 |
7 |
31-73 |
31-73 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, SR, |
Gao-hua Han, 2008 |
18 |
18 |
29 |
7 |
29-76 |
34-68 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, AFP, VEGF, IF |
Wei-min Wang, 2009 |
21 |
26 |
30 |
17 |
25-75 |
25-75 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, AE |
Xiao-bing Yuan, 2009 |
18 |
21 |
31 |
8 |
35-75 |
35-75 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
SR |
Hai-ying Jiang, 2010 |
50 |
50 |
77 |
23 |
30-60 |
30-60 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, SR, VEGF, AE |
Yun-xiao Lin, 2010 |
70 |
60 |
94 |
26 |
31-77 |
30-76 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
SR |
Fei Wang, 2010 |
38 |
34 |
48 |
24 |
15-70 |
15-70 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
SR, VEGF |
Zeng-hu Zhao, 2010 |
45 |
42 |
66 |
21 |
39-68 |
39-68 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, VEGF, AFP |
Yan Shang, 2011 |
60 |
60 |
69 |
51 |
31-74 |
31-74 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, SR, AE |
Hai-ying Jiang, 2011 |
50 |
50 |
77 |
23 |
37-72 |
37-72 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, SR, AE |
Zhen-kai Ye, 2013 |
38 |
39 |
72 |
5 |
23-69 |
23-69 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, SR |
Ji-qun Pan, 2013 |
27 |
27 |
38 |
16 |
36-76 |
36-76 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, DCR, VEGF, AFP |
Xiang-dong Lu, 2014 |
30 |
30 |
41 |
19 |
26-77 |
26-77 |
TACE+TLD: TLD, 200mg, po, qd |
TACE |
ORR, VEGF |
Xia Zhang, 2015 |
50 |
50 |
68 |
32 |
35-73 |
35-73 |
TACE+TLD: TLD, 100-200mg, po, qd |
TACE |
IF |
Di-yang Xie, 2015 |
42 |
48 |
NA |
NA |
NA |
NA |
TACE+TLD: TLD, 150-400mg, po, qd |
TACE |
SR, AE |
Cheng Zhang, 2015 |
40 |
40 |
47 |
33 |
31-77 |
30-76 |
TACE+TLD: TLD, 200-300mg, po, qd |
TACE |
ORR, DCR, SR, AE |
Kang Zheng, 2016 |
49 |
53 |
74 |
28 |
49-62 |
47-62 |
TACE+TLD: TLD, 200mg, po, qd |
TACE+sorafenib: Sorafenib, 400mg, po, bid |
ORR, DCR, SR, AFP, AE |
Abbreviation: NA: not available; po, oral administration; tid, three times a week; QOL, quality of life; PRS, Patient-Reported Symptoms; IF, immunity function; T, treatment; C, control; TLD, thalidomide; TACE, transcatheter arterial chemoembolization; SR, survival rate; ORR, overall response; DCR, disease control rate; AE, adverse events;
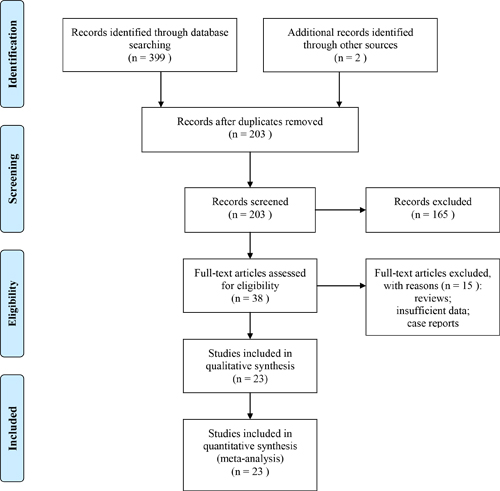
Figure 1: The flow chart of systematically research for eligible studies.
Results of quality evaluation
The overall quality of included studies was evaluated according to criteria for bias risk assessment in the Cochrane collaboration handbook 5.1.4. All of the eligible trials reported the application of randomization. Among these studies, four [32, 33, 44, 46] of them mentioned about the method of randomized number table, one [47] mentioned the use of envelop method, and the rest of them did not report detailed method of randomization. All of the studies did not report whether the treatment regimen was allocated or not. Only two studies [38, 39] used blinding method in the process of treatments. All of the studies presented the data about baseline characteristics and endpoints of participants and they were regarded as reporting complete data. Other sources of bias were not evaluable as all of the studies did not provide enough bias related data. The detailed information about quality assessment in each study is presented in Table 2.
Table 2: methodological quality evaluation of included studies
Studies |
Randomization |
Allocation |
Blinding |
Incomplete data |
Selective reporting |
Other bias |
Wei-sheng Zheng-1, 2007 |
Y |
N |
N |
N |
N |
NR |
Wei-sheng Zheng-2, 2007 |
Y |
N |
N |
N |
N |
NR |
Hai-lan Lin, 2007 |
Y |
N |
N |
N |
N |
NR |
Ming-zhi Hao, 2007 |
Y |
N |
N |
N |
N |
NR |
Xiao-jun Qi, 2007 |
Y |
N |
N |
Y |
N |
NR |
Xiu-fang Liu, 2007 |
Y |
N |
N |
N |
N |
NR |
Chang-nan Chen, 2008 |
Y |
N |
N |
Y |
N |
NR |
Long Feng, 2008 |
Y |
N |
N |
N |
N |
NR |
Wei-min Wang, 2009 |
Y |
N |
Y |
N |
N |
NR |
Xiao-bing Yuan, 2009 |
Y |
N |
Y |
N |
N |
NR |
Fei Wang, 2010 |
Y |
N |
N |
N |
N |
NR |
Zeng-hu Zhao, 2010 |
Y |
N |
N |
N |
N |
NR |
Hai-ying Jiang, 2010 |
Y |
N |
N |
N |
N |
NR |
Yun-xiao Lin, 2010 |
Y |
N |
N |
Y |
N |
NR |
Yan Shang, 2011 |
Y |
N |
N |
N |
N |
NR |
Hai-ying Jiang, 2011 |
Y |
N |
N |
N |
N |
NR |
Zhen-kai Ye, 2013 |
Y |
N |
N |
N |
N |
NR |
Ji-qun Pan, 2013 |
Y |
N |
N |
N |
N |
NR |
Xiang-dong Lu, 2014 |
Y |
N |
N |
N |
N |
NR |
Xia Zhang, 2015 |
Y |
N |
N |
N |
N |
NR |
Di-yang Xie, 2015 |
Y |
N |
N |
Y |
N |
NR |
Cheng Zhang, 2015 |
Y |
N |
N |
N |
N |
NR |
Kang Zheng, 2016 |
Y |
N |
N |
N |
N |
NR |
Abbreviation: Y, yes; N, no; NA, not available; NR, not reported
Results of Meta-analysis
Survival rates
There were 5 [32, 35, 36, 40, 53], 14 [32, 34-38, 40, 42-45, 47, 50, 51], 2 [36, 40], 12 [32, 34, 36, 37, 40, 42-45, 47, 50, 51], and 3 [34, 45, 51] studies reported data of survival rates at 6, 12, 18, 24, 36 months, respectively. As shown in Figure 2 and 3, there were no significant heterogeneity in most of the combined analyses in terms of survival rates, and the fixed effect model was used, except the 36 months survival. The results of meta-analyses revealed that compared to TACE alone, primary HCC patients treated with thalidomide and TACE could gain significantly superior in increasing 6-month survival rate(OR=1.79, 95% CI:1.02-3.15, P=0.04), 1-year survival rate(OR=1.76, 95% CI:1.38-2.24, P<0.0001), 1.5-year survival rate(OR=4.72, 95% CI:2.64-8.43, P<0.001), and 2-year survival rate(OR=1.78, 95% CI:1.37-2.30, P<0.001), respectively. However, there was no significant difference between combination group and TACE alone group in 3-year survival rate(OR=1.54, 95% CI:0.70-3.41, P=0.09 ).
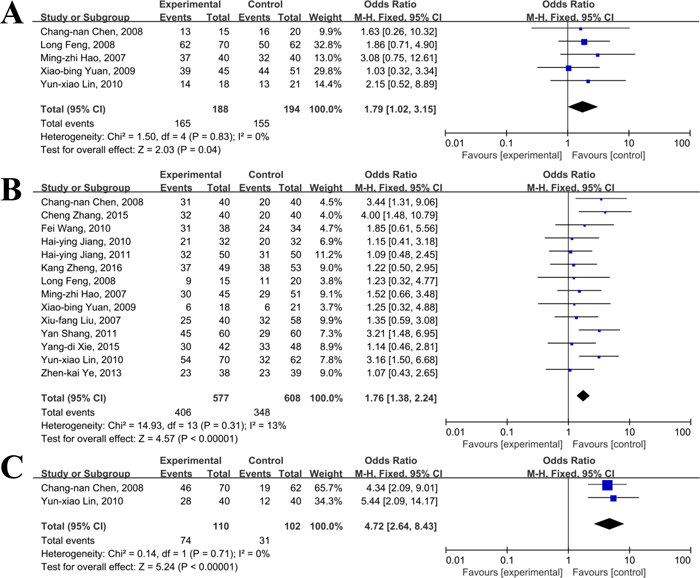
Figure 2: Meta-analyses of 6 (A), 12 (B), and 18 (C) months survival rates between thalidomide combined with TACE versus TACE alone in patients with primary HCC.
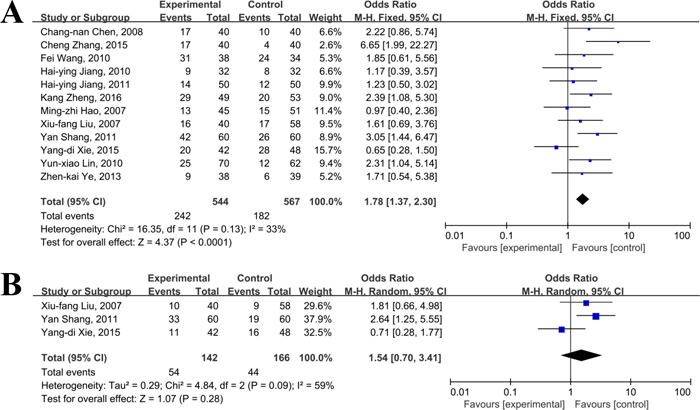
Figure 3: Meta-analyses of 24 (A) and 36 (B) months survival rates between thalidomide combined with TACE versus TACE alone in patients with primary HCC.
Overall response rate
Of the 23 included studies, 15 [34-37, 39, 41, 42, 44-47, 49-51] of them reported the ORR in primary HCC patients receiving thalidomide and TACE versus TACE alone. After inputting effective numbers and total cases in RevMan 5.3 software, the combined results showed that there was a low risk of heterogeneity as indicated by the I2 value=0%, and the fixed model was used to calculate the Odds Ratio(OR). As illustrated by Figure 4, there were 350(63.9%) cases gained significantly improvements in ORR in patients treated with thalidomide and TACE, when compared to 281 cases(49.0%) in TACE group(OR=1.89, 95%CI: 1.48-2.42; P<0.01). This finding indicated that thalidomide combined with TACE had a better efficacy than TACE alone in primary HCC patients. The sensitivity analyses showed that the final effect of combination regimen was reliable.
We introduced sub-group analysis to evaluate the clinical efficacy of thalidomide combined with different regimen of TACE. Included studies were divided into 3 groups(oxaliplatin based regimen, 5-Fu+DDP based regimen, and 5-Fu+ADM\EPI based regimen), according to the agents used in the TACE process. By using fixed effect model, the combined results showed that thalidomide plus oxaliplatin based regimen had a higher OR(OR=2.88, 95%CI: 1.34-6.19; P=0.007 ), followed by 5-Fu+DDP based regimen(OR=1.90, 95%CI: 1.31-2.76; P<0.001) and 5-Fu+ADM\EPI based regimen (OR=1.87, 95%CI: 1.21-2.88; P=0.005).
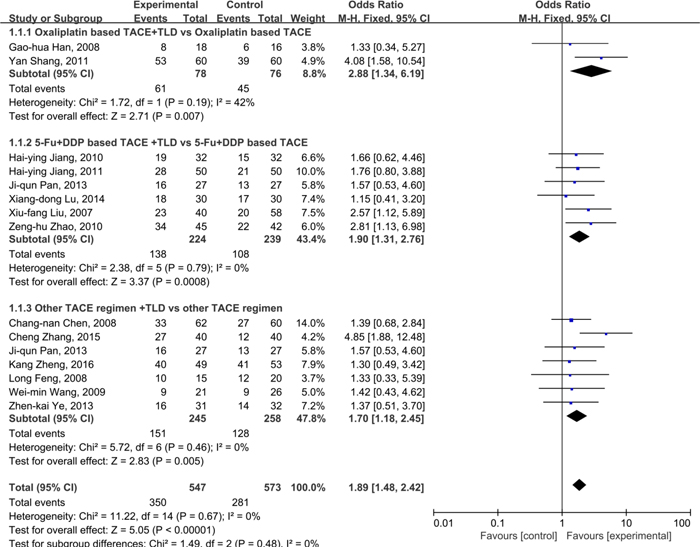
Figure 4: Comparison of ORR between thalidomide combined with TACE versus TACE alone in patients with primary HCC.
Disease control rate
There were 13 studies [34-37, 39, 41, 42, 44-47, 49, 50] reported data of disease control rate(DCR) with regards to regimen of thalidomide combined with TACE versus TACE alone in patients with primary HCC. As indicated by the I2%=0%, it was considered that there was no significant heterogeneity across included studies, and the fixed model was applied. As illustrated in Figure 5, the combined data showed that the DCR in thalidomide plus TACE group was significantly better than that in the TACE group(83.5% vs. 67.2%; OR=2.62, 95%CI: 1.90-3.63; P<0.01), suggesting that patients treated with thalidomide plus TACE may have a better DCR than TACE alone.
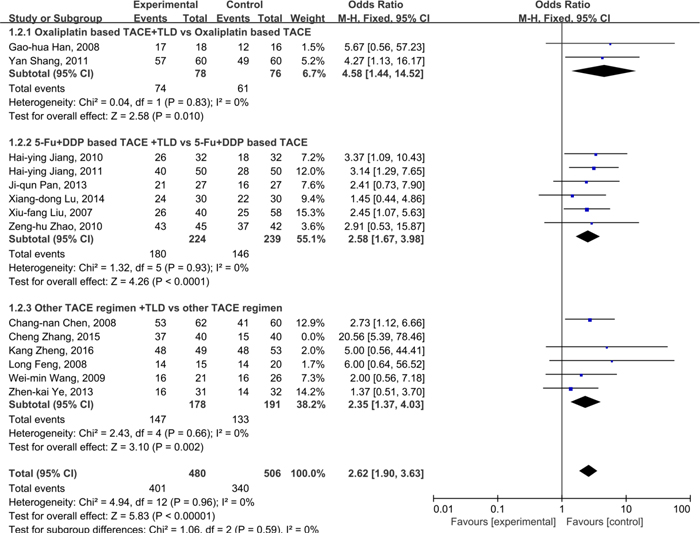
Figure 5: Comparison of DCR between thalidomide combined with TACE versus TACE alone in patients with primary HCC.
Quality of life
Only 1 of the included studies reported data about quality of life in terms of KPS scores. However, the meta-analysis was not performed as there was insufficient data and significant heterogeneity in the selected study. As shown by the study of Wei-sheng Zheng, et al., [30] compared to TACE treatment, a significant improvement in KPS scores was achieved in patients receiving thalidomide plus TACE treatment(KPS score: 51.71±8.75 vs. 43.13% ±7.39; P<0.05), showing that thalidomide plus TACE may have a better effect in improving the quality of life in patients with primary HCC when compared with TACE treatment.
Parameters of cellular immunity
Only 3 [37, 48, 52] of the included studies reported data about parameters of cellular immunity including CD3+, CD4+, CD8+, CD4+/CD8+, and NK. The results of meta-analysis revealed that significant heterogeneity was observed within these two trials(I2%>50%) on CD3+ and CD8+, and the random effect model was used to synthesize the data. As shown in Figure 6, compared to TACE treatment, significant improvements in CD4+(MD=9.54, 95%CI: 7.43-11.65; P<0.01), CD4+/CD8+(MD=0.63, 95%CI: 0.45-0.80; P<0.01), and NK(MD=9.74, 95%CI: 5.60-13.89; P<0.001) were achieved in patients receiving thalidomide plus TACE treatment, showing that thalidomide plus TACE may have a better effect in improving the quality of life in patients with primary HCC when compared with TACE treatment. However, the percentages of CD3+(MD=6.83, 95%CI: -18.19-31.85; P=0.59), and CD8+(MD=-1.46, 95%CI: -16.94-14.03; P=0.85) were not significantly different in combination group and TACE group.
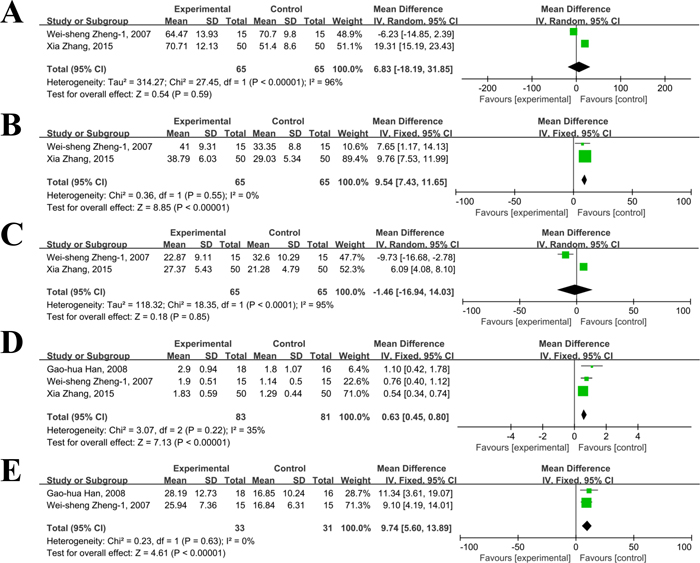
Figure 6: Comparison of cellular immunity between thalidomide combined with TACE versus TACE alone in patients with primary HCC (A, CD3+; B, CD4+ ; C, CD8+ ; D, CD4/CD8+; E, NK.).
Changes of VEGF and AFP
With regards to VEGF, 7 [33, 37, 42, 43, 46, 49, 54] of 23 RCTs provided data of changes of VEGF in patients treated with thalidomide and TACE. There was moderate heterogeneity(I2=43%) between these selected studies, so the fixed effect model was introduced. As shown in Figure 7, the levels of VEGF were significantly lower in patients treated with thalidomide and TACE when compared to TACE alone(MD=-119.71, 95% CI:-135.75--103.68; p<0.01), suggesting that thalidomide may have role of decreasing the level of VEGF when combined with TACE.
Six studies [34, 37, 41, 42, 46, 49] provided data about changes of AFP level or numbers of AFP reduction in patients receiving thalidomide combined with TACE versus TACE. For AFP levels, the analysis of heterogeneity showed that there was low risk of heterogeneity across selected studies(I2%=41%), and the fixed effect model was used. As presented in Figure 7, the combined mean difference was -74.76(95%CI:-90.25, -59.28; p<0.001). This suggested that thalidomide in combination with TACE had a better effect on reducing concentration of AFP in serum than TACE alone. For numbers of AFP reduction, three studies reported data of decrease rates of AFP level in patients with primary HCC receiving TACE plus thalidomide. As the I2%=0%, it was considered that there was no significant heterogeneity across included studies, and the fixed effect model was applied during the process of analysis. As shown in Figure 7, the cases with decreased AFP was 56 in combination group, and it was 42 cases in TACE alone group(55.4% vs. 35.9%; OR=2.21, 95%CI: 1.22-4.00; P=0.009), suggesting that the combination regimen had a better effect on decreasing AFP.
Table 3: Detailed information of TACE regimen in each included studies
Studies |
TACE regimens |
Wei-sheng Zheng-1, 2007 |
5-Fu 1.0g, OXA 200mg |
Wei-sheng Zheng-2, 2007 |
5-Fu 1.0g, OXA 200mg |
Hai-lan Lin, 2007 |
5-Fu 0.5-1.0g, OXA 100-200mg, Gem 0.4-1.6g |
Ming-zhi Hao, 2007 |
5-Fu 0.5-1.0g, OXA 100-200mg, Gem 0.4-1.6g |
Xiao-jun Qi, 2007 |
5-Fu 1.0g, HCPT 20mg, DDP 100mg |
Xiu-fang Liu, 2007 |
5-Fu 0.75-1.0mg, DDP 80-100mg, ADM 40-50mg |
Chang-nan Chen, 2008 |
NR |
Long Feng, 2008 |
5-Fu 1.0g, MMC 8-12mg, ADM 40-60mg \ EPI 70-90mg |
Gao-hua Han, 2008 |
5-Fu 750mg/m2, ADM 30-40mg/m2, OXA 125mg/m2 |
Wei-min Wang, 2009 |
5-Fu 600mg/m2, HCPT 20mg/m2, EPI 60 mg/m2 |
Xiao-bing Yuan, 2009 |
5-Fu 600mg/m2, HCPT 20mg/m2, EPI 60 mg/m2 |
Hai-ying Jiang, 2010 |
5-Fu 0.8-1.2g, DDP 80-100mg, EPI 80-120mg |
Yun-xiao Lin, 2010 |
NR |
Fei Wang, 2010 |
OXA 100mg, DOX 20mg |
Zeng-hu Zhao, 2010 |
5-Fu 1.0g, DDP 60-80mg, HCPT 10-20mg |
Yan Shang, 2011 |
OXA 150mg, EPI 70-90mg, HCPT, 10mg |
Hai-ying Jiang, 2011 |
5-Fu 0.8-1.2g, DDP 80-100mg, EPI 80-120mg |
Zhen-kai Ye, 2013 |
Gem 0.8-1.4g |
Ji-qun Pan, 2013 |
5-Fu 0.75-1.0g, DDP 80-100mg, EPI 80-120mg |
Xiang-dong Lu, 2014 |
5-Fu 0.75-1.0g, DDP 80-100mg, EPI 80-120mg |
Xia Zhang, 2015 |
5-Fu 0.75-1.25g, DDP 80-120mg, OXA 200mg, EPI 80-140mg |
Di-yang Xie, 2015 |
OXA, 100-150mg, 5-Fu 1.0, MMC 10mg |
Cheng Zhang, 2015 |
5-Fu 1.0g, ADM 40mg/m2, MMC 10mg/m2 |
Kang Zheng, 2016 |
ADM 20-50mg |
Abbreviation: 5-Fu, 5-fluoro-2,4(1h, 3h)pyrimidinedione; ADM, Adriamycin; MMC, Mitomycin; OXA, Oxaliplatin; DDP, Cisplatin; EPI, Epirubicin; HCPT, Hydroxycamptothecine; Gem, Gemcitabine; NR, not reported; DOX, Doxorubicin.
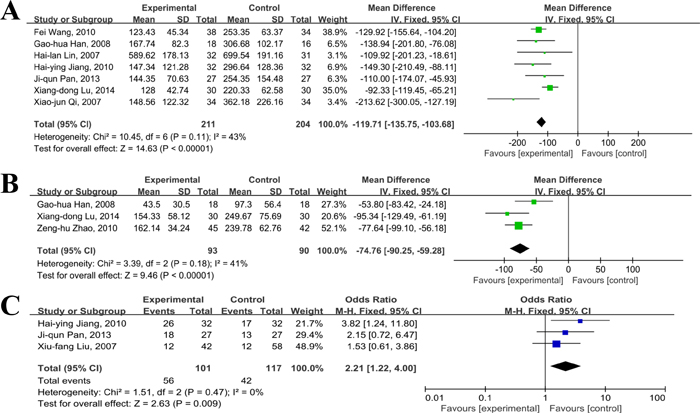
Figure 7: Comparison of changes of VEGF and AFP between thalidomide combined with TACE versus TACE alone in patients with primary HCC (A, changes of VEGF; B, changes of AFP; C, AFP reduction rates).
Adverse events
The common adverse events in the included studies [34, 39, 42, 44] were classed into hematological and non-hematological events(Figure 8). With regards to hematological toxicities, three studies [39, 42, 44] reported incidences of myelosuppression. The meta-analysis was performed based on the fixed effect model as there was no significant heterogeneity(I2%<10%). The results showed that the incidences of myelo-suppression were similar between thalidomide plus TACE group and TACE alone, and there was no significantly difference (OR=1.21, 95%CI:0.69-2.12; P=0.51). Non-hematological toxicities were mainly exhibited as drug rash, liver dysfunction, and gastrointestinal reactions. Three studies [39, 42, 44] provided events of drug rash and the detection of heterogeneity demonstrated negative finding (I2%=0%). The results of meta-analysis based on the fixed effect model revealed that there was significant difference in the incidence of drug rash in thalidomide plus TACE group when compared with TACE, indicating that the incidence of drug rash was higher in the combination group than that in the TACE alone group (OR=6.35, 95%CI: 2.75-14.68; P<0.01). Four studies [34, 39, 42, 44] reported the occurrence of gastrointestinal reactions. We used fixed effect model to calculate the combined result of gastrointestinal reactions, and the results showed that there was no statistically significant difference between thalidomide in combination with TACE group and TACE alone group (OR=1.30, 95%CI: 0.78-2.18; P=0.31). There RCTs showed the incidence of liver dysfunction and the combined results suggested that the events of liver dysfunction were similar between these two groups (OR=1.00, 95%CI: 0.57-1.77; P=0.99).
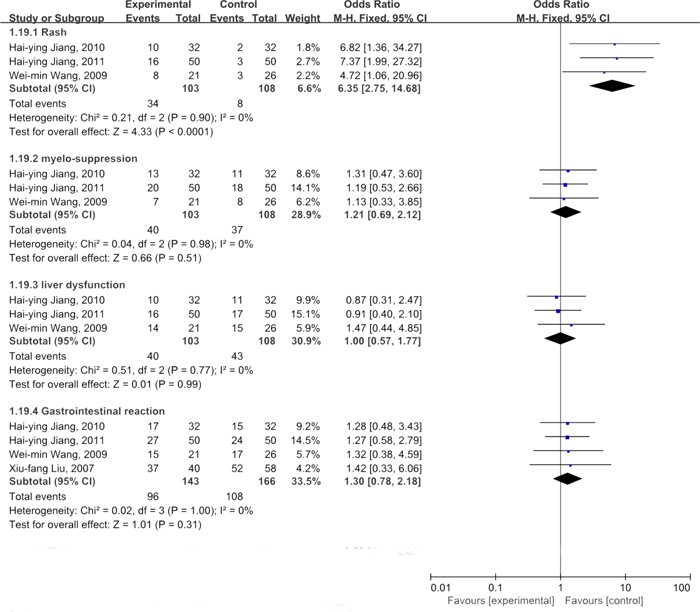
Figure 8: Comparison of common adverse events between thalidomide combined with TACE versus TACE alone in patients with primary HCC.
Results of publication bias
To assess the possibility of publication bias in ORR and 1-year survival rate, we introduced the Egg’s test and funnel plot. The results showed that the symmetries were good in both funnel plots, suggesting that there was low risk of publication bias (Figure 9). The results of Egg’s tests were 0.531 and 0.445 for ORR and 1-year survival rate. The risks of publication bias in DCR, parameters of cellular immunity, VEGF and adverse events were also evaluated, and the funnel plots were presented as supplementary figure. Overall, these funnel plots had good symmetry, suggesting that the results were less likely to be affected by publication bias.
Table 4: Evidence quality of combined effects
Endpoints |
N |
Combined effects |
Quality of evidence |
6-month survival |
382 |
OR=1.79, 95% CI:1.02-3.15 |
moderate |
12-month survival |
1185 |
OR=1.76, 95% CI:1.38-2.24 |
moderate |
18-month survival |
212 |
OR=4.72, 95% CI:2.64-8.43 |
moderate |
24-month survival |
1111 |
OR=1.78, 95% CI:1.37-2.30 |
moderate |
36-month survival |
308 |
OR=2.32, 95% CI:1.27-4.21 |
moderate |
ORR |
1120 |
OR=1.89, 95% CI:1.48-2.42 |
moderate |
DCR |
986 |
OR=2.62, 95% CI:1.90-3.63 |
moderate |
Reduction of VEGF |
415 |
MD=-119.71, 95% CI:-135.75--103.68 |
moderate |
Reduction of AFP |
183 |
MD=-74.76, 95%CI:-90.25- -59.28 |
moderate |
NK |
164 |
MD=9.74, 95%CI: 5.60-13.89 |
moderate |
CD4+/CD8+ |
64 |
MD=0.63, 95%CI: 0.45-0.80 |
moderate |
Rash |
211 |
OR=6.35, 95%CI: 2.75-14.68 |
moderate |
Abbreviation: OR, odds ratio; MD, mean difference; ORR, overall response rate; DCR, disease control rate; VEGF, vascular endothelial growth factor; AFP, alpha-fetoprotein; NK, natural killer.
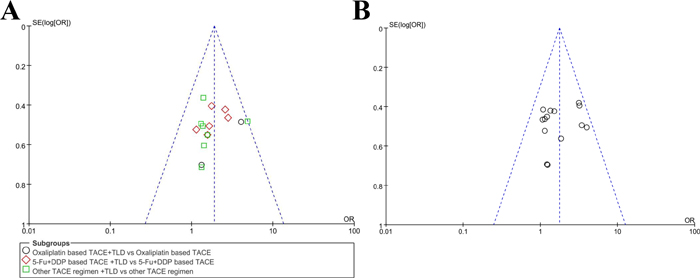
Figure 9: Funnel plot for publication bias (A, ORR; B, 1-year survival).
Discussion
Thalidomide has been widely used in clinical practice for treating several cancers including primary HCC. Several clinical trials suggested that thalidomide combined with TACE could significantly improve the clinical response rate, disease control rate, quality of life and survival rate in primary HCC, with tolerable adverse events. In this study, we systematically searched clinical studies on the topic of thalidomide combined with TACE versus TACE alone in patients with primary HCC, and used the synthesized data to determine the effect of thalidomide in improving the clinical efficacy of TACE. The combined results showed that thalidomide in combination with TACE had better ORR, DCR, quality of life and survival rates, and the decreases of AFP and VEGF were also significant, when compared with TACE alone. With regards to safety profile, administration of thalidomide significantly increased the incidence of drug rash, but not adverse events of gastrointestinal, myelo-suppression, and liver dysfunction.
The use of thalidomide has been proved to be beneficial in treating and delaying progression of several diseases, including HCC, multiple myeloma, and lung cancer. Several meta-analyses have evaluated the effectiveness of thalidomide in managements of multiple myeloma [17, 18, 55-61] and lung cancer [20]. These studies demonstrated that thalidomide maintenance therapy improved survival and disease control rates, which is in accordance with our main findings. The possible molecular mechanisms of thalidomide mainly includes anti-angiogenesis, inhibition of cytokines, such as TNF-á (tumor necrosis factor-á), bFGF (basic fibroblast growth factor) and VEGF(vascular endothelial growth factor) and modification of the expression of cell adhesion molecules [4, 17, 62]. The improvement in efficacy by adding thalidomide to TACE may be due to the anti-angiogenesis effect of thalidomide, as the VEGF level usually elevates after TACE [19, 37]. Compared with other anti-angiogenesis agents, especially sorafenib, thalidomide has been shown to be economical and practical benefits when combined with TACE and shows tolerable adverse events in primary HCC patients. Three meta-analyses [63-65] evaluated the effectiveness and safety of TACE plus sorafenib versus TACE alone for patients with unresectable HCC. The study of Liu et al. [63] reported that the DCR ranged from 18.4 to 91.2% in 10 noncomparative studies. Adding sorafenib to TACE may bring benefits for unresectable HCC in terms of TTP but not OS. In the study of Yang et al. [65], their meta-analysis of 6 studies including 1181 patients showed that the combination group of sorafenib and TACE had longer overall survival(HR=0.64, p<0.05) and TTP, and better response to treatment(RR=1.45, p<0.05) than TACE group. Fu et al. [64] also reported a similar conclusion that combination of sorafenib and TACE had survival and clinical benefits in patients with HCC, but associated with enhanced morbidity. In our included studies, the DCR ranged from 69 to 95%. The ORR data of these studies were available, and the combined data showed that application of thalidomide with TACE improved ORR in primary HCC patients. The DCR data from included studies were available, and the results showed a benefit of thalidomide for the improvement of DCR with non-significant heterogeneity. The combined benefits of using thalidomide in association with TACE in improving overall survival, progression free survival, and/or time to progression could not be calculated as relevant data was not provided by the included studies. However, by extracting data of survival rates at different follow-up, the synthesized results determined that thalidomide plus TACE had superior efficacy at 6, 12, 18, 24, 36 months, when compared with TACE alone. Indeed, several clinical trials[19, 66] and experimental studies [4, 24] also confirm the anti-tumor effects of thalidomide in HCC, and the results are encouraging.
As thalidomide shows effective outcomes in treating moderate and advanced HCC, whether tumor associated biomarker and angiogenesis related biomarker have roles in predicting its efficacy are being investigated [4, 25, 67]. In our meta-analysis, the changes of AFP and VEGF were reported by several included studies. Thalidomide with TACE reduced the serum level of AFP by a mean value of 141.95, better than TACE alone. Chen et al., [67] conducted a study to evaluate the clinical implications of AFP response in advanced HCC with thalidomide treatment. They included 42 patients for the final analysis, and defined AFP response as a 50% or greater reduction of AFP levels for 4 or more weeks during treatment. Radiographic response was determined by World Health Organization(WHO) criteria. The results showed that AFP response was obtained in 24% of patients, and it was independent prognostic factor for both PFS and OS. They concluded that AFP response after thalidomide therapy can more accurately reflect the biological response in HCC than radiographic response [67]. Another study conducted by Shao et al. [25], got a similar conclusion that early AFP response is a useful surrogate marker for predicting efficacy and prognosis in advanced HCC patients receiving thalidomide or sorafenib. With regard to VEGF, it has been proved to be a powerful pro-angiogenesis factor in several cancers including HCC [4, 68, 69]. In recent years, VEGF is also known as a prognostic biomarker in HCC patients treated with TACE or molecular targeted therapies [11, 70, 71]. In these studies, the level of VEGF before treatment is often used to predict clinical efficacy but not the changes of VEGF between prior- and post- treatments. Our results found that the mean level of VEGF was decreased by 123.64 in thalidomide plus TACE group than TACE group. These findings suggested that thalidomide could reduce the levels of AFP and VEGF, however, we could not determine whether the improved ORR, DCR and survival rates were associated with changed levels of AFP and VEGF. This needs well designed clinical trials and experimental studies to assess the relationship between changes of AFP and VEGF and prognosis and efficacy of thalidomide.
The quality of life in advanced HCC is always impaired and it gets worse when adverse events are emerged after treatments. How to enhance the anti-tumor effect of TACE without significantly affecting the quality of life and increasing the incidences of adverse events is extremely important. The pooled results showed that thalidomide treatment significantly improved quality of life in patients with HCC with tolerable safety events. Therefore, these points mentioned above may support the wide use of thalidomide in combination with TACE to obtain positive outcomes in terms of ORR, DCR, survival rates, quality of life and safety.
There were several limitations within this study. First, although all of the included studies were RCTs, differences in baseline characteristics, study design and clinical parameters of included patients were existed. For example, the ages, regions, performance status, and numbers of participants differed in included articles. Few studies reported detailed methods of randomization, and most of the studies did not report the method of blinding. The selective report bias may exist within the eligible studies, increasing the risk of publication bias. The different duration and doses of thalidomide treatment could increase the risk of heterogeneity, affecting the overall findings. Second, nearly all of the included studies were conducted in China, and they were small sample RCTs with limited number of participants. This could result in regional findings applicable for certain populations, decreasing the reliance of our results in clinical practice abroad. Even though, this meta-analysis was reliable and high quality as all of the selected studies were RCTs with relatively low risk of heterogeneity, and the results of this study could be used for guiding clinical treatment, especially for patients in China.
Conclusion
In summary, thalidomide with TACE was associated with a significant improvement in the response rate and better survival rates in primary HCC patients. These results were especially noteworthy for patients without consideration of surgical resection or transplantation in China. The therapeutic effects of thalidomide observed in this meta-analysis may be due to the reduction in serum AFP and VEGF levels. Our study provided new evidence for treatment of moderate or advanced HCC. Well-designed, large sample, multi-center, RCTs were required to support our findings.
materials and Methods
Search strategy
Electronic databases including the Cochrane Library, Pubmed, Embase, CNKI, and Wan Fang were searched for eligible studies with the deadline of August, 2016. The systematically search was conducted using the following terms with different combinations: “thalidomide” and “TACE or transcatheter arterial chemoembolization” and “primary hepatic carcinoma, liver cancer or hepatocellular carcinoma”. The whole process of search was conducted by two reviewers, independently.
Inclusion and exclusion criteria
The inclusion criteria for this study were as follows: (1) Study type: RCTs reporting clinical efficacy and safety of thalidomide combined with TACE versus TACE alone in treating patients with primary HCC, either in Chinese or English, regardless of blinding or allocation concealment; (2) Study subjects: patients were diagnosed as primary HCC with adequate evidence(histological diagnosis, imaging of liver enhanced MRI and/or CT )[8, 72], unsuitable for surgery, and Karnofsky score > 60, without limitation of sex, age, and race; (3)Interventions: thalidomide in combination with TACE versus TACE, thalidomide in combination with TACE and other treatments versus TACE and other treatments. The procedure and regimen for TACE were completely identical for both groups receiving TACE; (4)Endpoints: adequate and standard definition of primary endpoints included overall response rate(ORR), complete response(CR), partial response(PR), stable disease(SD) and progression disease(PD); adequate and standard definition of secondary endpoints were disease control rate(DCR), KPS score, survival rates at different times, changes of AFP and VEGF, and incidence of adverse events.
The exclusion criteria for this meta-analysis were as follows: (1) Study type: no clinical trials, no RCTs, retrospective studies; (2) duplicate publication; (3) un-reasonable design of methodology; (4) one-arm trial, case report, clinical experience, or review; (5) patients with poor performance status or unsuitable for TACE; (6) secondary or metastatic liver cancer; (7) no clear standards of diagnosis; (8) full-text without reporting required data.
Study selection
The selection of RCTs was completed by two reviewers, independently. First, the title and abstract of identified studies were reviewed and those did not meet the inclusion criteria were excluded; Next, to identify remaining studies, the full-texts of possibly eligible studies were checked. If there was disagreement to anyone of possible included studies, a third reviewer was involved to decide include or not.
Quality assessment
The methodological quality of included clinical trials were evaluated according to the standards of the Cochrane Reviewer Handbook 5.1.4. The risk of bias were classified as randomization, allocation concealment, blinding, incomplete data, selective data reporting and other potential sources of bias. The overall quality of included was defined as low, moderate, and high. Based on these standards, two reviewers independently assessed the bias of each eligible RCT. The inconsistent opinion on some RCT was solved by discussion or a third reviewer.
Data extraction
The baseline data of each eligible study was extracted by two reviewers based on the previously prepared data extraction table. Data needed to be recorded was as follows: (1) general information such as title, first author, publication year, and source; (2) data about participants such as sex, age, diagnosis criteria, numbers of cases for each group, and lost to follow-up; (3) data about study design and performance such as trial type, duration of study and follow-up, interventions for different groups and measurements; (4) data of outcomes, including efficacy, survival rate, changes of KPS and VEGF, incidence of adverse events. To obtain essential data, contact with corresponding authors if necessity.
Statistically analysis
All of the meta-analysis was performed using the RevMan 5.3 software. The methods used for statistically analysis were similar with previously published meta-analyses. Briefly, the heterogeneity between the included studies was analyzed by χ2 test. When the results of included studies were statistically homogeneous (P>0.1, I2<50%), the fixed effect model was used for meta-analysis. Otherwise, the random effect model was used for meta-analysis if the results of included studies were statistical heterogeneity (P <0.1, I2>50%). We also evaluated the possible factors that may contribute to heterogeneity, and subgroup analysis was performed based on these factors. In case of low-quality studies in meta-analysis, sensitivity analysis was used to test the stability and strength of the combined results. For dichotomous data, the pooled odd ratio(OR) were calculated with the 95% confidence interval (CI). For continuous data, the weighted mean differences(WMD) or Odds Ratio(OR) and their associated 95%CIs were calculated for every trial involved in the meta-analysis. We defined there was a statistically significant difference between combination group and TACE group if the p<0.05. The funnel plot was applied to detect possible publication bias, with the definition of p<0.1 as existing significant publication bias.
Acknowledgements
We thank Dr Yi-qiao Zhang for his contribution to this study.
Conflicts of Interest
The authors declare that there was no conflict of interest.
References
1. Zhu RX, Seto WK, Lai CL, Yuen MF. Epidemiology of Hepatocellular Carcinoma in the Asia-Pacific Region. Gut Liver. 2016; 10:332–39.
2. Yuan P, Chen P, Qian Y. Evaluation of Antiviral Therapy Performed after Curative Therapy in Patients with HBV-Related Hepatocellular Carcinoma: An Updated Meta-Analysis. Can J Gastroenterol Hepatol. 2016; 2016: 5234969.
3. Chiou HE, Wang TE, Wang YY, Liu HW. Efficacy and safety of thalidomide in patients with hepatocellular carcinoma. World J Gastroenterol. 2006; 12:6955–60.
4. Ch’ang HJ. Optimal combination of antiangiogenic therapy for hepatocellular carcinoma. World J Hepatol. 2015; 7:2029–40.
5. Bimonte S, Leongito M, Piccirillo M, de Angelis C, Pivonello C, Granata V, Izzo F. Radio-frequency ablation-based studies on VX2rabbit models for HCC treatment. Infect Agent Cancer. 2016; 11:38.
6. Yi PS, Zhang M, Zhao JT, Xu MQ. Liver resection for intermediate hepatocellular carcinoma. World J Hepatol. 2016; 8:607–15.
7. Zou JH, Zhang L, Ren ZG, Ye SL. Efficacy and safety of cTACE versus DEB-TACE in patients with hepatocellular carcinoma: a meta-analysis. J Dig Dis. 2016; 17:510–17.
8. Guo W, He X, Li Z, Li Y. Combination of Transarterial Chemoembolization (TACE) and Radiofrequency Ablation (RFA) vs. Surgical Resection (SR) on Survival Outcome of Early Hepatocellular Carcinoma: A Meta-Analysis. Hepatogastroenterology. 2015; 62:710–14.
9. Zhang L, Hu P, Chen X, Bie P. Transarterial chemoembolization (TACE) plus sorafenib versus TACE for intermediate or advanced stage hepatocellular carcinoma: a meta-analysis. PLoS One. 2014; 9:e100305.
10. Geschwind JF, Gholam PM, Goldenberg A, Mantry P, Martin RC, Piperdi B, Zigmont E, Imperial J, Babajanyan S, Foreman PK, Cohn A. Use of Transarterial Chemoembolization (TACE) and Sorafenib in Patients with Unresectable Hepatocellular Carcinoma: US Regional Analysis of the GIDEON Registry. Liver Cancer. 2016; 5:37–46.
11. Ranieri G, Ammendola M, Marech I, Laterza A, Abbate I, Oakley C, Vacca A, Sacco R, Gadaleta CD. Vascular endothelial growth factor and tryptase changes after chemoembolization in hepatocarcinoma patients. World J Gastroenterol. 2015; 21:6018–25.
12. Wan X, Zhai X, Yan Z, Yang P, Li J, Wu D, Wang K, Xia Y, Shen F. Retrospective analysis of transarterial chemoembolization and sorafenib in Chinese patients with unresectable and recurrent hepatocellular carcinoma. Oncotarget. 2016; 7:83806–16. doi: 10.18632/oncotarget.11514
13. Ranieri G, Marech I, Lorusso V, Goffredo V, Paradiso A, Ribatti D, Gadaleta CD. Molecular targeting agents associated with transarterial chemoembolization or radiofrequency ablation in hepatocarcinoma treatment. World J Gastroenterol. 2014; 20:486–97.
14. Trojan J, Zangos S, Schnitzbauer AA. Diagnostics and Treatment of Hepatocellular Carcinoma in 2016: standards and Developments. Visc Med. 2016; 32:116–20.
15. Dmoszynska A, Podhorecka M, Manko J, Bojarska-Junak A, Rolinski J, Skomra D. The influence of thalidomide therapy on cytokine secretion, immunophenotype, BCL-2 expression and microvessel density in patients with resistant or relapsed multiple myeloma. Neoplasma. 2005; 52:175–81.
16. Feng N, Chen H, Fu S, Bian Z, Lin X, Yang L, Gao Y, Fang J, Ge Z. HIF-1α and HIF-2α induced angiogenesis in gastrointestinal vascular malformation and reversed by thalidomide. Sci Rep. 2016; 6:27280.
17. Gao M, Kong Y, Wang H, Xie B, Yang G, Gao L, Zhang Y, Zhan F, Dai B, Tao Y, Shi J. Thalidomide treatment for patients with previously untreated multiple myeloma: a meta-analysis of randomized controlled trials. Tumour Biol. 2016; 37:11081–98.
18. Lyu WW, Zhao QC, Song DH, Zhang JJ, Ding ZX, Li BY, Wei CM. Thalidomide-based Regimens for Elderly and/or Transplant Ineligible Patients with Multiple Myeloma: A Meta-analysis. Chin Med J (Engl). 2016; 129:320–25.
19. Wu J, Ng J, Christos PJ, Goldenberg AS, Sparano J, Sung MW, Hochster HS, Muggia FM. Chronic thalidomide and chemoembolization for hepatocellular carcinoma. Oncologist. 2014; 19:1229–30.
20. Liu Y, He S, Ding Y, Huang J, Zhang Y, Chen L. The efficacy and safety of thalidomide-based therapy in patients with advanced non-small cell lung cancer: a meta-analysis. Contemp Oncol (Pozn). 2014; 18:39–47.
21. Huang YT, Cheng CC, Chiu TH, Lai PC. Therapeutic potential of thalidomide for gemcitabine-resistant bladder cancer. Int J Oncol. 2015; 47:1711–24.
22. Wang-Yuan Z, Jiang-Zheng Z, Lu YD, Hao XB, Hong T, Huang F, Lei JH, He ZH, Huang MZ. Clinical efficacy of metronomic chemotherapy after cool-tip radiofrequency ablation in the treatment of hepatocellular carcinoma. Int J Hyperthermia. 2016; 32:193–98.
23. Liang PC, Ch’ang HJ, Hsu C, Chen LT, Shih TT, Liu TW. Perfusion parameters of dynamic contrast-enhanced magnetic resonance imaging predict outcomes of hepatocellular carcinoma receiving radiotherapy with or without thalidomide. Hepatol Int. 2015; 9:258–68.
24. Nagy LI, Molnár E, Kanizsai I, Madácsi R, Ózsvári B, Fehér LZ, Fábián G, Marton A, Vizler C, Ayaydin F, Kitajka K, Hackler L Jr, Mátés L, et al. Lipid droplet binding thalidomide analogs activate endoplasmic reticulum stress and suppress hepatocellular carcinoma in a chemically induced transgenic mouse model. Lipids Health Dis. 2013; 12:175.
25. Shao YY, Lin ZZ, Hsu C, Shen YC, Hsu CH, Cheng AL. Early alpha-fetoprotein response predicts treatment efficacy of antiangiogenic systemic therapy in patients with advanced hepatocellular carcinoma. Cancer. 2010; 116:4590–96.
26. Yau T, Chan P, Wong H, Ng KK, Chok SH, Cheung TT, Lam V, Epstein RJ, Fan ST, Poon RT. Efficacy and tolerability of low-dose thalidomide as first-line systemic treatment of patients with advanced hepatocellular carcinoma. Oncology. 2007; 72:67–71.
27. Chuah B, Lim R, Boyer M, Ong AB, Wong SW, Kong HL, Millward M, Clarke S, Goh BC. Multi-centre phase II trial of Thalidomide in the treatment of unresectable hepatocellular carcinoma. Acta Oncol. 2007; 46:234–38.
28. Hao MZ, Lin HL, Chen Q, Wu H, Yu WC, Chen TG. Efficacy of transcatheter arterial chemoembolization combined thalidomide on hepatocellular carcinoma: a controlled randomized trial. Chin J Cancer. 2007; 26:861–65.
29. Hsu C, Chen CN, Chen LT, Wu CY, Yang PM, Lai MY, Lee PH, Cheng AL. Low-dose thalidomide treatment for advanced hepatocellular carcinoma. Oncology. 2003; 65: 242-9.
30. Weisheng Z, Qiang C, Yunbin Y, Hailan L, Mingzhi H, Wenchang Y, Kongzhi Z, Qizhong C. Influence of treatment of HCC with thalidomide in combination with TACE on Quality of life. CHINESE JOURNAL OF CLINICAL ONCOLOGY AND REHABILITATION. 2007: 478-80.
31. Hai-lan L, Yun-bin HM-zZW-sY, Jian-xiong CQ-zCJ-bZ. The changes of vascular endothelial growth factor after treatment of thalidomide combined with TACE for HCC. Zhongguo Jieru Yingxiang Yu Zhiliaoxue. 2007:440–43.
32. Hao MZ, Lin HL, Chen Q, Wu H, Yu WC, Chen TG. [Efficacy of transcatheter arterial chemoembolization combined thalidomide on hepatocellular carcinoma: a controlled randomized trial] [Article in Chinese]. Ai Zheng. 2007; 26:861–65.
33. Xiao-jun Q, Yu-dong J. Treatment of primary hepatic cancer by transcatheter hepatic artery chemoembolization therapy combined with thalidomide. Chinese Journal Of Cancer Prevention And Treatment. 2007: 788-9.
34. Xiu-fang L, Hai Z, Bing-sheng W, Jian-yu Z. Efficacy of combined thalidomide and interventional therapy in treatment of advanced hepatocellular carcinoma. Chinese Journal of Clinical Oncology And Rehabilitation. 2007; 546-7:50.
35. Long F, Wu-hua G, Lin L, Jian-bing W, Chun-ying X. The Preliminary Observation of the Therapeutic Effect of Transcather Arterial Chemoembolization Combined with Thalidomide on Advanced Hepatic Carcinoma. PRACTICAL CLINICAL MEDICINE. 2008; 29-30:4.
36. Chang-nan C, Qi-zuo P, Yun-xiao L, Ming-jun S, Huo-xun H, Jia-kang Z, Miao-wen Z, Jin-song Y. Effect of thalidomide combined with TACE on recurrence and survival of primary liver cancer. China Trop Med. 2008:406–08.
37. Cheng Z, Changnan C, Yunxiao L, Mingjun S, Zhijian L, Qizuo P, Bingzhao L, Chanjuan C, Tingjie R, Feng X. Clinical effect of transcatheter arterial chemoembolization combined with gimeracil and oteracil potassium and thalidomide in treatment of advanced hepatocellular carcinoma. Journal of Modern Oncology. 2015; 2475-8.
38. Xiao-bing Y, Xing-long H, Xiang S, Shi-wu Y, Cheng-fa L, Man M. Clinical research on advanced primary carcinoma of liver treated with transcatheter arterial chemoembolization combined Thalidomide. Anhui Medical and Pharmaceutical Journal. 2009: 1270-2.
39. Wei-min W, Shi-wu Y, Xiang S, Cheng-fa L, Ma M, Xiao-bing Y, Meng-qin H, Rong-jie Y, Ying-xing C. Clinical research on middle - high dose Thalidomide Combined TACE treatment of primary liver cancer. Anhui Medical Journal. 2009: 1419-22.
40. Yun-xiao L, Chan-nan C, Qi-zuo P, Huo-xun Z. The Combination of Thalidomide with Transcatheter Arterial Chemoembolization in Treating Primary Liver Cancer. Journal of Gannan Medical University. 2010: 44-5.
41. Zenghu Z, Xiufang L, Ruiliang D, Quanfu N. Clinical study of TACE combined with thalidomide and traditional Chinese medicine in patients with intermediate or advanced HCC. Journal of Emergency in Traditional Chinese Medicine. 2010: 1492-3.
42. Haiying J, Xiaodong X, Mei Z. The Analyses of Efficacy of Thalidomide Combined with Transcatheter Arterial Chemoembolization of Advanced Hepatocellular Carcinoma. JOURNAL OF BASIC AND CLINICAL ONCOLOGY. 2010: 226-8.
43. Fei W. Therapeutic effect of thalidomide plus TACE for patients with intermediate or advanced primary hepatocellular carcinoma. Guide of China medicine. 2010: 228-9.
44. Hai-ying J, Xiao-dong X, Mei Z. Combination of thalidomide and transcatheter arterial chemoembolization for advanced hepatocellular carcinoma. China J Cancer Prev Treat. 2011; 871-3:81.
45. Yan S, Hui-bin CM-cJ, Xue-ming X, Shu-xun L. Clinical study of transcatheter arterial chemoembolization combined with thalidomide on advanced hepatic carcinoma. Chinese Journal of Cancer Prevention and Treatment. 2011: 1043-5.
46. Jiqun P, Bai LGS, Bingshan X, Xiaomei L, Zhijian Y. Efficacy of the regimen of transcatheter arterial chemoembolization sequential thalidomide in advanced hepatocellular carcinoma. Journal of Modern Oncology. 2013: 811-3.
47. Zhenkai Y, Yaozhen L, Yan LJC. Effect of advanced hepatocellular carcinoma treated by conformal radiotherapy after thalidomide combined with trancather arterial chemoembolization. Journal of Modern Oncology. 2013: 2276-9.
48. Xia Z, Guangping L, Jiqun P. Effect of thalidomide combined with TACE on T lymphocytes and erythrocyte immune function of primary liver cancer. Shandong Yiyao. 2015: 70–72.
49. Lu Xd, Zhang Dr, Huang Xz. Clinical observation of efficacy of thalidomide combined with TACE for patients with intermediate or advanced stage primary hepatocellular carcinoma. Jiangsu Med J. 2014: 95-6.
50. Kang Z, Mengguo H, Zhixiang W. Therapeutic effect of transcatheter arterial chemoembolization combined with thalidomide or sorafenib in treatment of unresectable primary liver cancer: a comparative analysis. J Clin Hepatol. 2016: 899-903.
51. Xie D, Zhang L, Zhang J, Xie X, Yin X, Xue T, Chen R, Wang Y, Zhang B, Ren Z. Randomized controlled trial of thalidomide combined with transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: an interim analysis. National Liver Cancer Conference. 2015: 71.
52. Weisheng Z, Qiang C, Yunbin Y, Hailan L, Mingzhi H, Wenchang Y, Kongzhi Z, Qizhong C. The Changes of Cellular Immunity Function After Treatment of Thalidomide Combined with TACE for HCC. JOURNAL OF BASIC AND CLINICAL ONCOLOGY. 2007: 145-7.
53. Yun-xiao L, Chan-nan C, Qi-zuo P, Huo-xun H. The Combination of Thalidomide with Transcatheter Arterial Chemoembolization in Treating Primary Liver Cancer. JOURNAL OF GANNAN MEDICAL UNIVERSITY. 2009: 176-7.
54. Hailan L, Zhenhua Z, Mingzhi H, Qiang C, Hui W, Wenchang Y, Kongzhi Z, Qizhong C. The impact of thalidomide on the disease progression time after TACE in patients with primary heaptocellular carcinoma. Fujian Med J. 2007:14–16.
55. Huang H, Zhou L, Peng L, Fu W, Zhang C, Hou J. Bortezomib-thalidomide-based regimens improved clinical outcomes without increasing toxicity as induction treatment for untreated multiple myeloma: a meta-analysis of phase III randomized controlled trials. Leuk Res. 2014; 38:1048–54.
56. Leiba M, Kedmi M, Duek A, Freidman T, Weiss M, Leiba R, Nagler A, Avigdor A. Bortezomib-cyclophosphamide-dexamethasone (VCD) versus bortezomib-thalidomide-dexamethasone (VTD) -based regimens as induction therapies in newly diagnosed transplant eligible patients with multiple myeloma: a meta-analysis. Br J Haematol. 2014; 166:702–10.
57. Wang L, Xu YL, Zhang XQ. Bortezomib in combination with thalidomide or lenalidomide or doxorubicin regimens for the treatment of multiple myeloma: a meta-analysis of 14 randomized controlled trials. Leuk Lymphoma. 2014; 55:1479–88.
58. Palumbo A, Waage A, Hulin C, Beksac M, Zweegman S, Gay F, Gimsing P, Leleu X, Wijermans P, Sucak G, Pezzatti S, Juliusson G, Pégourié B, et al. Safety of thalidomide in newly diagnosed elderly myeloma patients: a meta-analysis of data from individual patients in six randomized trials. Haematologica. 2013; 98:87–94.
59. Kagoya Y, Nannya Y, Kurokawa M. Thalidomide maintenance therapy for patients with multiple myeloma: meta-analysis. Leuk Res. 2012; 36:1016–21.
60. Wang L, Cui J, Liu L, Sheng Z. Postrelapse survival rate correlates with first-line treatment strategy with thalidomide in patients with newly diagnosed multiple myeloma: a meta-analysis. Hematol Oncol. 2012; 30:163–69.
61. Morgan GJ, Gregory WM, Davies FE, Bell SE, Szubert AJ, Brown JM, Coy NN, Cook G, Russell NH, Rudin C, Roddie H, Drayson MT, Owen RG, et al, and National Cancer Research Institute Haematological Oncology Clinical Studies Group. The role of maintenance thalidomide therapy in multiple myeloma: MRC Myeloma IX results and meta-analysis. Blood. 2012; 119:7–15.
62. Adlard JW. Thalidomide in the treatment of cancer. Anticancer Drugs. 2000; 11:787–91.
63. Liu L, Chen H, Wang M, Zhao Y, Cai G, Qi X, Han G. Combination therapy of sorafenib and TACE for unresectable HCC: a systematic review and meta-analysis. PLoS One. 2014; 9:e91124.
64. Fu QH, Zhang Q, Bai XL, Hu QD, Su W, Chen YW, Su RG, Liang TB. Sorafenib enhances effects of transarterial chemoembolization for hepatocellular carcinoma: a systematic review and meta-analysis. J Cancer Res Clin Oncol. 2014; 140:1429–40.
65. Yang M, Yuan JQ, Bai M, Han GH. Transarterial chemoembolization combined with sorafenib for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Mol Biol Rep. 2014; 41:6575–82.
66. Demeria D, Birchall I, Bain VG. Dramatic reduction in tumour size in hepatocellular carcinoma patients on thalidomide therapy. Can J Gastroenterol. 2007; 21:517–18.
67. Chen LT, Liu TW, Chao Y, Shiah HS, Chang JY, Juang SH, Chen SC, Chuang TR, Chin YH, Whang-Peng J. alpha-fetoprotein response predicts survival benefits of thalidomide in advanced hepatocellular carcinoma. Aliment Pharmacol Ther. 2005; 22:217–26.
68. Zucman-Rossi J, Villanueva A, Nault JC, Llovet JM. Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology. 2015; 149: 1226-39 e4.
69. Tirumani SH, Fairchild A, Krajewski KM, Nishino M, Howard SA, Baheti AD, Rosenthal MH, Jagannathan JP, Shinagare AB, Ramaiya NH. Anti-VEGF molecular targeted therapies in common solid malignancies: comprehensive update for radiologists. Radiographics. 2015; 35:455–74.
70. Cao G, Li X, Qin C, Li J. Prognostic Value of VEGF in Hepatocellular Carcinoma Patients Treated with Sorafenib: A Meta-Analysis. Med Sci Monit. 2015; 21:3144–51.
71. Matsui D, Nagai H, Mukozu T, Ogino YU, Sumino Y. VEGF in patients with advanced hepatocellular carcinoma receiving intra-arterial chemotherapy. Anticancer Res. 2015; 35:2205–10.
72. Tsurusaki M, Murakami T. Surgical and Locoregional Therapy of HCC: TACE. Liver Cancer. 2015; 4:165–75.