
INTRODUCTION
Colorectal cancer (CRC) is one of the leading causes of cancer-related morbidity and mortality [1]. Except for advanced age, family history, male sex, and lifestyle factors which contribute to the increased risk of CRC, many genetic factors has been identified to be associated with susceptibility [1–6]. High-penetrance germline mutations, mismatch repair genes, together with identified loci from genome-wide association studies (GWAS), account for about 14% of the familial risk of CRC [7]. However, a large part of heritable factors are warranted to be explored [7, 8]. Further exploration of the interactive mechanism between genes and environment is helpful for specific diagnosis, screening, and personal treatment [9, 10].
With the innovations in sequencing technologies, long noncoding RNAs (lncRNAs) are being identified and characterized for serial steps of cancer development, including tumor initiation, growth, and metastasis [11–18]. Previously, we identified that the allele del of lncRNA GAS5 rs145204276 was significantly associated with 21% decreased risk of CRC [19]. Carriers of allele del are less likely to get lymph node metastasis, which should that GAS5 rs145204276 were significantly associated with the susceptibility and progression of CRC [19]. Here, we explored effect of genetic variants of another lncRNA on CRC risk in a case-control study, Tissue differentiation-inducing non-protein coding RNA (TINCR), a key lncRNA required for somatic tissue differentiation and tumor progression [20, 21]. Loss of TINCR expression promoted proliferation, metastasis through activating EpCAM cleavage in colorectal cancer [22].
RESULTS
Demographic characteristics
As shown in Table 1, the characteristics of the subjects were generally comparable in two stages, as no significant difference were detected for age group, gender, alcohol status and smoking status between CRC cases and healthy controls (all the P value > 0.05).
Table 1: The characteristics of the study population
Variables |
Stage I |
Stage II |
||||
|---|---|---|---|---|---|---|
Cases (n=600) |
Controls (n=600) |
P value |
Cases (n=800) |
Controls (n=800) |
P value |
|
Age group |
||||||
≥60 |
255 (42.5%) |
264 (44.0%) |
0.600 |
365 (45.6%) |
362 (45.2%) |
0.880 |
<60 |
345 (57.5%) |
336 (56.0%) |
435 (54.4%) |
438 (54.8%) |
||
Gender |
||||||
Male |
369 (61.5%) |
372 (62.0%) |
0.859 |
480 (60.0%) |
468 (58.5%) |
0.542 |
female |
231 (38.5%) |
228 (38.0%) |
320 (40.0%) |
332 (41.5%) |
||
Smoking status |
||||||
Smokers |
186 (31.0%) |
171 (28.5%) |
0.344 |
232 (29.0%) |
212 (26.5%) |
0.264 |
Non-Smokers |
414 (69.0%) |
429 (71.5%) |
568 (71.0%) |
588 (73.5%) |
||
Alcohol status |
||||||
drinkers |
201 (33.5%) |
180 (30.0%) |
0.193 |
280 (35.0%) |
256 (32.0%) |
0.204 |
Non-drinkers |
399 (66.5%) |
420 (70.0%) |
520 (65.0%) |
544 (68.0%) |
||
Tumor site |
||||||
Colon |
340 (56.7%) |
466 (58.2%) |
||||
Rectum |
260 (43.3%) |
334 (41.8%) |
||||
Lymph node metastasis |
||||||
No |
390 (65.0%) |
500 (62.5%) |
||||
Yes |
210 (35.0%) |
300 (37.5%) |
||||
Distant metastasis |
||||||
No |
507 (84.5%) |
688 (86.0%) |
||||
Yes |
93 (15.5%) |
112 (14.0%) |
||||
Associations between TINCR polymorphisms and CRC susceptibility
Figure 1 shows the selection of tagSNPs for TINCR gene, including rs2288947, rs8105637, and rs12610531. The distribution of genotypes of all three tagSNPs in healthy controls in the two stage was in accordance with Hardy-Weinberg equilibrium (HWE, P > 0.05). As shown in Table 2, two SNPs, rs2288947 and rs8105637, were significantly associated with susceptibility of CRC in stage I (P=0.004 and 0.022, respectively). Thus, we replicated the associations of the two SNPs in an independent population (stage II, Table 3), which also presented statistically significant associations and same trend (P=0.007 and 0.009, respectively). When pooled together, the allele G was significantly associated with 23% decreased risk of CRC (OR=0.77; 95% CI=0.67-0.88; P value = 1.2×10-4) for SNP rs2288947. While for SNP rs8105637, the allele A was significantly associated with 22% increased risk of CRC (OR=1.22; 95% CI=1.09-1.37; P value = 6.2×10-4).
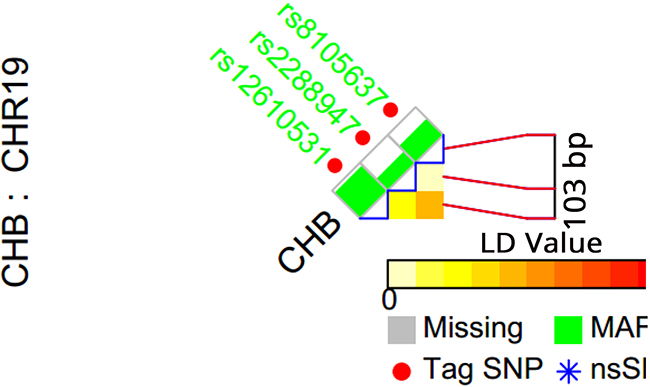
Figure 1: TagSNP selection for TINCR gene. Red point represents a TagSNP, while gray square means “missing”, and green square means MAF.
Table 2: Associations between TINCR gene polymorphisms and CRC susceptibility in stage I
Genotypes |
Cases (n, %) |
Controls (n, %) |
OR (95% CI)a |
P Value |
|---|---|---|---|---|
rs2288947 |
||||
AA |
384 (64.0%) |
342 (57.0%) |
1.00 (Reference) |
|
AG |
195 (32.5%) |
221 (36.8%) |
0.78 (0.61-0.99) |
0.047 |
GG |
21 (3.5%) |
37 (6.2%) |
0.51 (0.46-1.03) |
0.010 |
G vs A |
0.75 (0.62-0.91) |
0.004 |
||
rs8105637 |
||||
GG |
281 (46.8%) |
315 (52.5%) |
1.00 (Reference) |
|
AG |
264 (44.0%) |
245 (40.8%) |
1.21 (0.96-1.52) |
0.106 |
AA |
55 (9.2%) |
40 (6.7%) |
1.54 (1.01-2.35) |
0.045 |
A vs G |
1.22 (1.03-1.45) |
0.022 |
||
rs12610531 |
||||
AA |
186 (31.0%) |
173 (28.8%) |
1.00 (Reference) |
|
AG |
310 (51.7%) |
316 (52.7%) |
0.91 (0.70-1.18) |
0.489 |
GG |
104 (17.3%) |
111 (18.5%) |
0.87 (0.62-1.22) |
0.425 |
G vs A |
0.93 (0.79-1.10) |
0.411 |
a adjusted by age, gender, alcohol and smoking status
Table 3: Associations between selected TINCR gene polymorphisms and CRC susceptibility in stage II
Genotypes |
Cases (n, %) |
Controls (n, %) |
OR (95% CI)a |
P Value |
|---|---|---|---|---|
rs2288947 |
||||
Stage II |
||||
AA |
526 (65.8%) |
480 (60.0%) |
1.00 (Reference) |
|
AG |
240 (30.0%) |
270 (33.8%) |
0.81 (0.66-1.00) |
0.049 |
GG |
34 (4.2%) |
50 (6.2%) |
0.62 (0.39-0.97) |
0.037 |
G vs A |
0.79 (0.69-0.94) |
0.007 |
||
Pooled results |
||||
AA |
910 (65.0%) |
822 (58.7%) |
1.00 (Reference) |
|
AG |
435 (31.1%) |
491 (35.1%) |
0.80 (0.68-0.94) |
0.006 |
GG |
55 (3.9%) |
87 (6.2%) |
0.57 (0.40-0.81) |
0.002 |
G vs A |
0.77 (0.67-0.88) |
1.2×10-4 |
||
rs8105637 |
||||
Stage II |
||||
GG |
365 (45.6%) |
412 (51.5%) |
1.00 (Reference) |
|
AG |
354 (44.3%) |
328 (41.0%) |
1.22 (0.99-1.50) |
0.060 |
AA |
81 (10.1%) |
60 (7.5%) |
1.52 (1.06-2.18) |
0.022 |
A vs G |
1.22 (1.05-1.42) |
0.009 |
||
Pooled results |
||||
GG |
646 (46.1%) |
727 (51.9%) |
1.00 (Reference) |
|
AG |
618 (44.2%) |
573 (40.9%) |
1.21 (1.04-1.42) |
0.014 |
AA |
136 (9.7%) |
100 (7.1%) |
1.53 (1.16-2.02) |
0.003 |
A vs G |
1.22 (1.09-1.37) |
6.2×10-4 |
a adjusted by age, gender, alcohol and smoking status
Associations between TINCR polymorphisms and CRC susceptibility stratified by tumor site
The associations between rs2288947, rs8105637 and CRC susceptibility were analyzed by Tumor site (Table 4). In colon and rectum cancers, the trend was not materially changed.
Table 4: Associations between TINCR gene polymorphisms and CRC susceptibility stratified by tumor site
Genotypes |
Colon cancer |
Rectum cancer |
||||||
|---|---|---|---|---|---|---|---|---|
Cases (n, %) |
Controls (n, %) |
OR (95% CI)a |
P value |
Cases (n, %) |
Controls (n, %) |
OR (95% CI)a |
P value |
|
rs2288947 |
||||||||
AA |
540 (67.0%) |
822 (58.7%) |
1.00 (Reference) |
370 (65.0%) |
822 (58.7%) |
1.00 (Reference) |
||
AG |
242 (30.0%) |
491 (35.1%) |
0.75 (0.62-0.91) |
0.003 |
193 (31.1%) |
491 (35.1%) |
0.87 (0.71-1.07) |
0.199 |
GG |
24 (3.0%) |
87 (6.2%) |
0.42 (0.27-0.66) |
1.7×10-4 |
31 (3.9%) |
87 (6.2%) |
0.79 (0.52-1.21) |
0.284 |
G vs A |
0.70 (0.60-0.82) |
1.3×10-5 |
0.88 (1.03-0.74) |
0.117 |
||||
rs8105637 |
||||||||
GG |
370 (45.9%) |
727 (51.9%) |
1.00 (Reference) |
276 (46.5%) |
727 (51.9%) |
1.00 (Reference) |
||
AG |
354 (43.9%) |
573 (40.9%) |
1.21 (1.01-1.46) |
0.037 |
264 (44.4%) |
573 (40.9%) |
1.21 (0.99-1.48) |
0.059 |
AA |
82 (10.2%) |
100 (7.1%) |
1.61 (1.17-2.21) |
0.003 |
54 (9.1%) |
100 (7.1%) |
1.53 (0.99-2.03) |
0.053 |
A vs G |
1.24 (1.09-1.42) |
0.001 |
1.19 º(1.03-1.38) |
0.018 |
||||
a adjusted by age, gender, alcohol and smoking status
Associations between TINCR polymorphisms and lymph node metastasis and distant metastasis of CRC
We also investigated the associations between rs2288947, rs8105637 and Lymph node metastasis and Distant metastasis of CRC. As shown in Table 5, the carriers of allele G are less likely to get lymph node metastasis (OR=0.77; 95% CI=0.63-0.94; P value = 0.011) for rs2288947, and the carriers of allele A are more likely to get lymph node metastasis (OR=1.22; 95% CI=1.03-1.43; P value = 0.019) for rs8105637. Due to the limited sample size and statistical power, the associations with distant metastasis of CRC were not significant (P>0.05).
Table 5: Associations between TINCR gene polymorphisms and Lymph node metastasis and Distant metastasis of CRC
Genotypes |
Lymph node metastasis |
Distant metastasis |
||||||
|---|---|---|---|---|---|---|---|---|
Event (n, %) |
No event (n, %) |
OR (95% CI)a |
P trend |
Event (n, %) |
No event (n, %) |
OR (95% CI)a |
Ptrend |
|
rs2288947 |
||||||||
AA |
352 (69.0%) |
552 (62.0%) |
1.00 (Reference) |
137 (66.8%) |
773 (64.7%) |
1.00 (Reference) |
||
AG |
140 (27.5%) |
298 (33.5%) |
0.74 (0.58-0.94) |
61 (31.3%) |
374 (31.3%) |
0.92 (0.66-1.27) |
||
GG |
18 (3.5%) |
40 (4.5%) |
0.70 (0.40-1.25) |
7 (3.4%) |
48 (4.0%) |
0.82 (0.37-1.85) |
||
G vs A |
0.77 (0.63-0.94) |
0.011 |
0.91 (0.70-1.20) |
0.517 |
||||
rs8105637 |
||||||||
GG |
215 (42.1%) |
431 (48.4%) |
1.00 (Reference) |
89 (43.4%) |
557 (46.6%) |
1.00 (Reference) |
||
AG |
238 (46.7%) |
380 (42.7%) |
1.25 (1.00-1.58) |
93 (45.4%) |
525 (43.9%) |
1.11 (0.81-1.52) |
||
AA |
57 (11.2%) |
79 (8.9%) |
1.45 (0.99-2.11) |
23 (11.2%) |
113 (9.5%) |
1.27 (0.77-2.10) |
||
A vs G |
1.22 (1.03-1.43) |
0.019 |
1.12 (0.90-1.40) |
0.319 |
||||
a adjusted by age, gender, alcohol and smoking status
DISCUSSION
The current study systematically explored the potential associations between three tagSNPs of lncRNA TINCR, including rs2288947, rs8105637, and rs12610531, and risk and progression of CRC in in a two-stage, case-control study in Chinese population. To be best of our knowledge, this should be the first study which aims to evaluated the associations between genetic variation of lncRNA TINCR and susceptibility and progression of CRC.
Recent studies have elucidated the important role and mechanism of lncRNAs in cancer development and progression, although the specific functions of most lncRNAs remain unknown [13, 14, 16–18, 23–25]. The most focused lncRNA, HOTAIR which cooperate with Polycomb complex PRC2 and reprogram chromatin organization, could promote cancer metastasis in colorectal cancer [26]. Its genetic variations have been confirmed to be associated with susceptibility of ovarian cancer, cervical cancer, breast cancer, and gastric cancer [27–32]. Very recently, Ma et al [33] reported tagSNPs of lncRNA TINCR could affect the genetic susceptibility to gastric cancer in a Chinese population. Consistent with our results, they found, the variant AG, GG, and GG+AG genotypes and G allele of rs2288947 were correlated with a remarkably reduced risk of GC (P= 0.026, 0.026, 0.008 and 0.037 respectively), compared with the AA genotype and A allele [33]. Different with our results, rs8105637 was not associated with GC risk in the report of Ma et al [33]. Using HaploReg v4.1 [34], we found rs2288947 could alter 5 motifs, including CTCF_disc9, Nanog_disc3, Rad21_disc10, SMC3_disc3, and SP1_disc3. While rs8105637 could alter expression of Pitx2, TCF12. These motifs have been confirmed to be associated with carcinogenesis and metastasis [35–40].
In the stratified analyses, we observed difference in the association between rs2288947 genotype and CRC risk according to tumor site. The association was more significant for colon cancer while not significant for rectal cancer, although the exact mechanisms for these differences are currently unclear. We also didn’t detected significant association between lncRNA TINCR rs2288947, rs8105637 and distant metastasis of CRC. They might be caused by to the limited sample size of the event cases and the insufficient statistical power.
Our study has several strengths. First, the implement of the two-stage, case-control study design, which is suggested for genetic association studies [41, 42]. Second, we have sufficient statistic power to detect such associations. Using QUANTO software (http://biostats.usc.edu/Quanto.html), we found that the statistic power for the log additive model of rs2288947 was 98%, and 92% for that of rs8105637. There are also limitations in the current study. Such as the lack of independent replication with different ethnic background, and mechanism research. Further investigations are required to gain insight into the mechanisms by which TINCR regulates the occurrence progress of CRC.
Taken together, this is the first study demonstrating the potential associations between genetic variation of lncRNA TINCR with susceptibility and progression of CRC in Chinese population. Our results firstly indicate that SNP rs2288947 and rs8105637 may act as independent biomarkers associated with occurrence and progression of CRC. This study provided valuable clues for better understanding the underlying contribution of genetic variation of lncRNA TINCR to carcinogenesis of CRC. Future functional studies should be conducted to further explore the role of lncRNA TINCR in the development and progression of CRC basing on the epidemiological findings.
PATIENTS AND METHODS
Study subjects
In this two-stage, cases-control study, we totally recruited 1400 CRC cases and 1400 healthy controls between 2010 and 2015, which were matched by age group, gender, alcohol and smoking status. We have described these in a previous study which evaluated the functional of LncRNA GAS5 in development and progression of CRC [19]. Five milliliter peripheral blood was collected from all subjects, and demographic information were face to face interviewed by the project staff. The study was approved by appropriate Research Ethics Committee (REC) of Renmin Hospital of Wuhan University, and written informed consent was obtained from all participants.
TagSNP selection, DNA extraction and genotyping
TagSNP selection was conducted using SNPinfo (https://snpinfo.niehs.nih.gov/). Qiagen genomic DNA purification kit were used for extraction of the genomic DNA from blood samples. Genotyping was performed using the TaqMan allelic discrimination assay on the ABI PRISM 7900HT Sequence Detection System. The genotyping results were determined by using the SDS 2.3 Allelic Discrimination Software (Applied
Biosystems, Carlsbad, CA). Quality control was conducted by direct sequencing 5% duplicate samples in blind, with a concordance rate of 100%. Furthermore, a 5% random selected sample was replicated in duplicate by different persons, and the concordance rate was 100%.
Statistical analysis
Unconditional Logistic regression model was used to calculate the Odds ratios (ORs) and 95% confidence intervals (95% CIs) for the associations between TINCRpolymorphisms and risk of CRC and its Lymph node metastasis and Distant metastasis, adjusted for age group, gender, alcohol and smoking status. Hardy-Weinberg equilibrium was tested for with a goodness of fit χ2 test with one degree of freedom to compare the observed genotype frequencies among the subjects with the expected genotype frequencies. All statistics were performed using SPSS software 19.0 (SPSS Inc., Chicago, IL, USA), and P values were two sided with the statistical significance criteria of P < 0.05 all through the study.
ACKNOWLEDGMENTS
This study was sponsored by National Natural Science Foundation of China (81372553).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
1. Kolligs FT. Diagnostics and Epidemiology of Colorectal Cancer. Visc Med. 2016; 32: 158-64. doi: 10.1159/000446488.
2. Lee DH, Keum N, Giovannucci EL. Colorectal Cancer Epidemiology in the Nurses’ Health Study. Am J Public Health. 2016; 106: 1599-607. doi: 10.2105/AJPH.2016.303320.
3. Zanke BW, Greenwood CM, Rangrej J, Kustra R, Tenesa A, Farrington SM, Prendergast J, Olschwang S, Chiang T, Crowdy E, Ferretti V, Laflamme P, Sundararajan S, et al. Genome-wide association scan identifies a colorectal cancer susceptibility locus on chromosome 8q24. Nat Genet. 2007; 39: 989-94. doi: 10.1038/ng2089.
4. Tomlinson I, Webb E, Carvajal-Carmona L, Broderick P, Kemp Z, Spain S, Penegar S, Chandler I, Gorman M, Wood W, Barclay E, Lubbe S, Martin L, et al. A genome-wide association scan of tag SNPs identifies a susceptibility variant for colorectal cancer at 8q24.21. Nat Genet. 2007; 39: 984-8. doi: 10.1038/ng2085.
5. Broderick P, Carvajal-Carmona L, Pittman AM, Webb E, Howarth K, Rowan A, Lubbe S, Spain S, Sullivan K, Fielding S, Jaeger E, Vijayakrishnan J, Kemp Z, et al. A genome-wide association study shows that common alleles of SMAD7 influence colorectal cancer risk. Nat Genet. 2007; 39: 1315-7. doi: 10.1038/ng.2007.18.
6. de la Chapelle A. Genetic predisposition to colorectal cancer. Nat Rev Cancer. 2004; 4: 769-80. doi: 10.1038/nrc1453.
7. Ma X, Zhang B, Zheng W. Genetic variants associated with colorectal cancer risk: comprehensive research synopsis, meta-analysis, and epidemiological evidence. Gut. 2014; 63: 326-36. doi: 10.1136/gutjnl-2012-304121.
8. Peters U, Hutter CM, Hsu L, Schumacher FR, Conti DV, Carlson CS, Edlund CK, Haile RW, Gallinger S, Zanke BW, Lemire M, Rangrej J, Vijayaraghavan R, et al. Meta-analysis of new genome-wide association studies of colorectal cancer risk. Hum Genet. 2011. doi: 10.1007/s00439-011-1055-0.
9. Schumacher FR, Schmit SL, Jiao S, Edlund CK, Wang H, Zhang B, Hsu L, Huang SC, Fischer CP, Harju JF, Idos GE, Lejbkowicz F, Manion FJ, et al. Genome-wide association study of colorectal cancer identifies six new susceptibility loci. Nat Commun. 2015; 6: 7138. doi: 10.1038/ncomms8138.
10. Wu CW, Ng SS, Dong YJ, Ng SC, Leung WW, Lee CW, Wong YN, Chan FK, Yu J, Sung JJ. Detection of miR-92a and miR-21 in stool samples as potential screening biomarkers for colorectal cancer and polyps. Gut. 2012; 61: 739-45. doi: 10.1136/gut.2011.239236.
11. Yang G, Lu X, Yuan L. LncRNA: a link between RNA and cancer. Biochim Biophys Acta. 2014; 1839: 1097-109. doi: 10.1016/j.bbagrm.2014.08.012.
12. Chang L, Wang G, Jia T, Zhang L, Li Y, Han Y, Zhang K, Lin G, Zhang R, Li J, Wang L. Armored long non-coding RNA MEG3 targeting EGFR based on recombinant MS2 bacteriophage virus-like particles against hepatocellular carcinoma. Oncotarget. 2016; 7:23988-4004. doi: 10.18632/oncotarget.8115.
13. Du M, Wang W, Jin H, Wang Q, Ge Y, Lu J, Ma G, Chu H, Tong N, Zhu H, Wang M, Qiang F, Zhang Z. The association analysis of lncRNA HOTAIR genetic variants and gastric cancer risk in a Chinese population. Oncotarget. 2015; 6:31255-62. doi: 10.18632/oncotarget.5158.
14. Feng T, Shao F, Wu Q, Zhang X, Xu D, Qian K, Xie Y, Wang S, Xu N, Wang Y, Qi C. miR-124 downregulation leads to breast cancer progression via LncRNA-MALAT1 regulation and CDK4/E2F1 signal activation. Oncotarget. 2016; 7:16205-16. doi: 10.18632/oncotarget.7578.
15. Gong X, Wei W, Chen L, Xia Z, Yu C. Comprehensive analysis of long non-coding RNA expression profiles in hepatitis B virus-related hepatocellular carcinoma. Oncotarget. 2016; 7:42422-42430. doi: 10.18632/oncotarget.9880.
16. Li H, An J, Wu M, Zheng Q, Gui X, Li T, Pu H, Lu D. LncRNA HOTAIR promotes human liver cancer stem cell malignant growth through downregulation of SETD2. Oncotarget. 2015; 6:27847-64. doi: 10.18632/oncotarget.4443.
17. Li L, Dang Q, Xie H, Yang Z, He D, Liang L, Song W, Yeh S, Chang C. Infiltrating mast cells enhance prostate cancer invasion via altering LncRNA-HOTAIR/PRC2-androgen receptor (AR)-MMP9 signals and increased stem/progenitor cell population. Oncotarget. 2015; 6: 14179-90. doi: 10.18632/oncotarget.3651.
18. Li S, Hua Y, Jin J, Wang H, Du M, Zhu L, Chu H, Zhang Z, Wang M. Association of genetic variants in lncRNA H19 with risk of colorectal cancer in a Chinese population. Oncotarget. 2016; 7:25470-7. doi: 10.18632/oncotarget.8330.
19. Zheng Y, Song D, Xiao K, Yang C, Ding Y, Deng W, Tong S. LncRNA GAS5 contributes to lymphatic metastasis in colorectal cancer. Oncotarget. 2016; 7:83727-83734. doi: 10.18632/oncotarget.13384.
20. Kretz M, Siprashvili Z, Chu C, Webster DE, Zehnder A, Qu K, Lee CS, Flockhart RJ, Groff AF, Chow J, Johnston D, Kim GE, Spitale RC, et al. Control of somatic tissue differentiation by the long non-coding RNA TINCR. Nature. 2013; 493: 231-5. doi: 10.1038/nature11661.
21. Chen Z, Liu Y, He A, Li J, Chen M, Zhan Y, Lin J, Zhuang C, Liu L, Zhao G, Huang W, Cai Z. Theophylline controllable RNAi-based genetic switches regulate expression of lncRNA TINCR and malignant phenotypes in bladder cancer cells. Sci Rep. 2016; 6: 30798. doi: 10.1038/srep30798.
22. Zhang ZY, Lu YX, Chang YY, Zheng L, Yuan L, Zhang F, Hu YH, Zhang WJ, Li XN. Loss of TINCR expression promotes proliferation, metastasis through activating EpCAM cleavage in colorectal cancer. Oncotarget. 2016; 7: 22639-49. doi: 10.18632/oncotarget.8141.
23. Li H, Yu B, Li J, Su L, Yan M, Zhu Z, Liu B. Overexpression of lncRNA H19 enhances carcinogenesis and metastasis of gastric cancer. Oncotarget. 2014; 5: 2318-29. doi: 10.18632/oncotarget.1913.
24. Li W, Zhai L, Wang H, Liu C, Zhang J, Chen W, Wei Q. Downregulation of LncRNA GAS5 causes trastuzumab resistance in breast cancer. Oncotarget. 2016; 7:27778-86. doi: 10.18632/oncotarget.8413.
25. Li Y, Chen H, Pan T, Jiang C, Zhao Z, Wang Z, Zhang J, Xu J, Li X. LncRNA ontology: inferring lncRNA functions based on chromatin states and expression patterns. Oncotarget. 2015; 6: 39793-805. doi: 10.18632/oncotarget.5794.
26. Gupta RA, Shah N, Wang KC, Kim J, Horlings HM, Wong DJ, Tsai MC, Hung T, Argani P, Rinn JL, Wang Y, Brzoska P, Kong B, et al. Long non-coding RNA HOTAIR reprograms chromatin state to promote cancer metastasis. Nature. 2010; 464: 1071-6. doi: 10.1038/nature08975.
27. Qiu H, Wang X, Guo R, Liu Q, Wang Y, Yuan Z, Li J, Shi H. HOTAIR rs920778 polymorphism is associated with ovarian cancer susceptibility and poor prognosis in a Chinese population. Future Oncol. 2016. doi: 10.2217/fon-2016-0290.
28. Liu FT, Zhou L, Qiu C, Xia G, Zhu PQ, Luo HL. Association of the HOTAIR rs4759314 polymorphism with cancer risk: a meta-analysis. J BUON. 2016; 21: 1016-23. doi:
29. Qiu H, Liu Q, Li J, Wang X, Wang Y, Yuan Z, Pei DS. Analysis of the association of HOTAIR single nucleotide polymorphism (rs920778) and risk of cervical cancer. APMIS. 2016; 124: 567-73. doi: 10.1111/apm.12550.
30. Bayram S, Sumbul AT, Dadas E. A functional HOTAIR rs12826786 C>T polymorphism is associated with breast cancer susceptibility and poor clinicopathological characteristics in a Turkish population: a hospital-based case-control study. Tumour Biol. 2016; 37: 5577-84. doi: 10.1007/s13277-015-4430-y.
31. Bayram S, Ulger Y, Sumbul AT, Kaya BY, Rencuzogullari A, Genc A, Sevgiler Y, Bozkurt O, Rencuzogullari E. A functional HOTAIR rs920778 polymorphism does not contributes to gastric cancer in a Turkish population: a case-control study. Fam Cancer. 2015; 14: 561-7. doi: 10.1007/s10689-015-9813-0.
32. Bayram S, Sumbul AT, Batmaci CY, Genc A. Effect of HOTAIR rs920778 polymorphism on breast cancer susceptibility and clinicopathologic features in a Turkish population. Tumour Biol. 2015; 36: 3863-70. doi: 10.1007/s13277-014-3028-0.
33. Ma X, Huang C, Luo D, Wang Y, Tang R, Huan X, Zhu Y, Xu Z, Liu P, Yang L. Tag SNPs of long non-coding RNA TINCR affect the genetic susceptibility to gastric cancer in a Chinese population. Oncotarget. 2016; 7:87114-87123. doi: 10.18632/oncotarget.13513.
34. Ward LD, Kellis M. HaploReg: a resource for exploring chromatin states, conservation, and regulatory motif alterations within sets of genetically linked variants. Nucleic Acids Res. 2012; 40: D930-4. doi: 10.1093/nar/gkr917.
35. He J, Shen S, Lu W, Zhou Y, Hou Y, Zhang Y, Jiang Y, Liu H, Shao Y. HDAC1 promoted migration and invasion binding with TCF12 by promoting EMT progress in gallbladder cancer. Oncotarget. 2016; 7: 32754-64. doi: 10.18632/oncotarget.8740.
36. Chen WS, Chen CC, Chen LL, Lee CC, Huang TS. Secreted heat shock protein 90alpha (HSP90alpha) induces nuclear factor-kappaB-mediated TCF12 protein expression to down-regulate E-cadherin and to enhance colorectal cancer cell migration and invasion. J Biol Chem. 2013; 288: 9001-10. doi: 10.1074/jbc.M112.437897.
37. Lee CC, Chen WS, Chen CC, Chen LL, Lin YS, Fan CS, Huang TS. TCF12 protein functions as transcriptional repressor of E-cadherin, and its overexpression is correlated with metastasis of colorectal cancer. J Biol Chem. 2012; 287: 2798-809. doi: 10.1074/jbc.M111.258947.
38. Jezkova E, Kajo K, Zubor P, Grendar M, Malicherova B, Mendelova A, Dokus K, Lasabova Z, Plank L, Danko J. Methylation in promoter regions of PITX2 and RASSF1A genes in association with clinicopathological features in breast cancer patients. Tumour Biol. 2016. doi: 10.1007/s13277-016-5324-3.
39. Lee WK, Chakraborty PK, Thevenod F. Pituitary homeobox 2 (PITX2) protects renal cancer cell lines against doxorubicin toxicity by transcriptional activation of the multidrug transporter ABCB1. Int J Cancer. 2013; 133: 556-67. doi: 10.1002/ijc.28060.
40. Hirose H, Ishii H, Mimori K, Tanaka F, Takemasa I, Mizushima T, Ikeda M, Yamamoto H, Sekimoto M, Doki Y, Mori M. The significance of PITX2 overexpression in human colorectal cancer. Ann Surg Oncol. 2011; 18: 3005-12. doi: 10.1245/s10434-011-1653-z.
41. Milne RL, Fagerholm R, Nevanlinna H, Benitez J. The importance of replication in gene-gene interaction studies: multifactor dimensionality reduction applied to a two-stage breast cancer case-control study. Carcinogenesis. 2008; 29: 1215-8. doi: 10.1093/carcin/bgn120.
42. Zuo Y, Zou G, Zhao H. Two-stage designs in case-control association analysis. Genetics. 2006; 173: 1747-60. doi: 10.1534/genetics.105.042648.