
INTRODUCTION
Bone metastasis is a common cause of serious morbidity in patients with breast cancer. It is associated with various debilitating skeletal-related events, which include bone fractures, hypercalcemia, nerve compression, and severe pain. The diagnosis of bone metastasis influences the patient’s prognosis, reducing overall survival (OS) [1]. The early detection of bone metastases in newly diagnosed breast cancer patients is important because it changes the ideal treatment strategies [2–4]. Recent guidelines recommend that stage IIIA breast cancer patients should undergo staging with either conventional bone scintigraphy or with 18F-Fluoride PET/CT [5]. While both 18F-fluoride (PET/CT) and 99mTc-MDP (conventional bone scintigraphy) are bone-seeking tracers used to identify bone remodeling and detect areas of increased bone remodeling due to metastases [6], when comparing the two imaging modalities for staging and restaging breast cancer patients, clearly 18F-fluoride PET/CT is ideal due to greater sensitivity, specificity and accuracy [7]. Furthermore, 18F-Fluoride PET/CT has been shown to alter treatment plan in approximately 39% of breast cancer patients [8].
Beyond lesion detection and staging, it is feasible to quantify skeletal tumor burden using 18F-Fluoride PET/CT. Determination of skeletal tumor burden has been shown to have a prognostic role in prostate cancer patients treated with 223Ra [9].
Studies have shown that calculation of the primary tumor metabolism using parameters such as total lesion glycolysis (TLG) and metabolic tumor volume (MTV) on 18F-FDG PET/CT images predicts survival in breast cancer patients at initial staging [10, 11]. However, when breast cancer patients develop bone metastases, there are no means to foresee which patients will have a shorter survival time. Even though breast cancer bone metastases are 18F-FDG-avid, unfortunately, quantification of whole-body tumor burden with this tracer is not practical because the areas of normal biodistribution.
Only one recent study investigated the prognostic role of 18F-Fluoride PET/CT in breast cancer patients semi-quantitatively [12]. While the authors did not find a significant correlation, the parameters that they used did not evaluate the entire bone disease extent on 18F-Fluoride images. To that effect, there are no studies that calculated the entire skeletal tumor burden turnover on 18F-Fluoride PET/CT and correlated with prognosis in breast cancer patients.
The purpose of this study was to correlate skeletal tumor burden determined by 18F-Fluoride PET/CT with clinical outcomes in breast cancer patients.
RESULTS
Patient characteristics
A total of 107 female patients, mean age 59.6 ± 13.3 years and a mean of 4.1 ± 4.9 years from primary diagnosis (0.1 – 20.3 years) were studied (Table 1). The median follow-up time was 19.5 months (2 - 83 months). Among the 107 patients studied, twenty-three patients died and, among these, two died very early after performing the 18F-Fluoride PET/CT study (2 and 7 months afterwards). Histology consisted of 91 (85%) invasive ductal carcinomas, 12 (11.2%) invasive lobular carcinomas, 3 adenocarcinomas (2.8%) and 1 sarcoma (1%). According to the TNM staging system, 30 (28%) patients were stage I, 29 (27%) were stage II, 35 (33%) were stage III and 13 (12%) had stage IV disease.
Table 1: Clinical characteristics of patients
N or median |
% or range |
||
|---|---|---|---|
Age |
59.6 |
30–93 |
|
Years of cancer |
4.0 |
0.1–20.3 |
|
PR positive |
69 |
64% |
|
ER positive |
78 |
73% |
|
Histology type |
Ductal |
91 |
85% |
Lobular |
12 |
11.2% |
|
Adenocarcinoma |
3 |
2.8% |
|
Others |
1 |
< 1%* |
|
Her-2 expression |
14 |
13% |
|
TNM stage at diagnosis |
I |
30 |
28% |
II |
29 |
27.1% |
|
III |
35 |
32.7% |
|
IV |
13 |
12.1% |
|
Previous treatments |
chemotherapy |
82 |
77% |
radiotherapy |
53 |
50% |
|
surgery |
57 |
53% |
|
hormone therapy |
87 |
81% |
|
no treatment |
2 |
1,9% |
ER = estrogen receptor; PR = progesterone receptor; * = sarcoma.
The patients were submitted to 18F-Fluoride PET/CT for detection of bone metastases. Forty patients underwent 18F-Fluoride PET/CT for primary staging of breast cancer. The remainder underwent 18F-Fluoride PET/CT with suspicion of bone metastases prior to or after some modality of treatment. The treatment consisted of one or more of the following: chemotherapy (82 patients), radiotherapy (53 patients), surgery (57 patients) and hormone therapy (87 patients).
Among the 107 patients enrolled, 49 patients (45.8%) were diagnosed with bone metastases. Analyzing only the population that performed the 18F-Fluoride PET/CT for staging, 32.5% (13 patients) were positive for bone metastasis.
The analysis of the tumor burden of these 49 patients was undertaken and compared to the 58 patients without bone, visceral or nodal metastases. Nineteen patients (17.7%) had visceral metastases (15 patients with lung metastases and 4 patients with liver metastases) at the time of the 18F-Fluoride PET/CT examination. All patients with hepatic lesions and 12 patients with lung lesions had also bone metastases. Thus, 16 patients (15%) had bone and visceral metastases. Although all patients had undergone CT scans of the chest, abdomen and pelvis for detection of visceral metastases, 20 patients (18.7%) also underwent an 18F-FDG PET/CT study within 3 months of the 18F-Fluoride PET/CT. In these cases, the 18F-FDG PET/CT exams were also considered when evaluating for visceral metastases.
Skeletal tumor burden (TLF10) analysis of the 49 patients with bone metastases
18F-Fluoride PET/CT images detected bone metastasis in 49 (45.8%) patients. The hSUV of the bone metastases for all patients (mean ± SD) was 46.7 ± 23.37 (range 12.6 - 96.5) and the Mean10 for all patients (mean ± SD) was 14.8 ± 5.2 (range 9.4 - 43.2). The mean FTV10 was 204.1 ml (range 0.5–1578 ml) and the mean TLF10 was 3395.3 (range 9.0–39410). TLF10 and FTV10 values were highly correlated (p = 0.95; P < 0.0001) and therefore only TLF10 was used for further analyses.
TLF10 and OS
At the end of the follow-up period, 84 patients were alive (30 with bone metastasis). The median overall survival was 15.2 months for patients with bone metastasis and 23.4 months for patients without bone metastasis.
TLF10 was significantly associated with OS on univariable analyses (p < 0.0001; HR = 1.136; 95% CI = 1.066–1.210). The presence of bone or visceral metastasis, hSUV, negative progesterone receptor (PR) status and ECOG status were also correlated with survival in the univariate analysis. Other parameters such as initial tumor characteristics (HER2 status, ER status, Ki-67 index), the current patient´s age, the time of disease, ECOG status, current pain score, and treatments (surgery, chemotherapy and radiotherapy) during the course of disease did not correlate with OS.
On multivariable analyses TLF10 (p < 0.0001; HR = 1.136; 95% CI = 1.062–1.216) and negative PR status of the primary tumor (p = 0.0025; HR = 4.648; 95% CI = 1.575–13.718) were the only two parameters significantly associated with OS (Table 2).
Table 2: Correlation of clinical, laboratory and imaging variables to overall survival
Variables |
HR |
95% CI |
p-value |
|
|---|---|---|---|---|
Univariable analyses |
||||
Age |
0.998 |
0.9131 |
||
Time of disease |
1.011 |
0.929 |
1.099 |
0.8046 |
Primary stage (III/IV vs I/II) |
1.117 |
0.423 |
2.953 |
0.8230 |
HER2 |
1.019 |
0.388 |
2.674 |
0.9697 |
ER status |
1.763 |
0.578 |
5.379 |
0.3192 |
PR status |
4.078 |
1.513 |
10.991 |
0.0055 |
Ki-67 |
1.020 |
0.999 |
1.042 |
0.095 |
Radiotherapy (y/n) |
1.140 |
0.445 |
2.917 |
0.7853 |
Hormonal therapy (y/n) |
1.783 |
0.657 |
4.831 |
0.2561 |
Surgery (y/n) |
2.067 |
0.762 |
5.604 |
0.1539 |
ECOG status |
4.101 |
1.517 |
11.083 |
0.0054 |
Pain score |
2.537 |
0.991 |
6.496 |
0.0524 |
Visceral metastases |
5.181 |
2.488 |
10.799 |
< 0.0001 |
Bone metastases |
6.461 |
2.190 |
19.062 |
0.0007 |
hSUV |
1.022 |
1.005 |
1.041 |
0.0139 |
Mean10 |
0.927 |
0.882 |
1.084 |
0.6647 |
TLF10 |
1.136 |
1.066 |
1.210 |
< 0.0001 |
Multivariable analysis |
||||
TLF10 |
1.136 |
1.062 |
1.216 |
< 0.001 |
PR status |
4.648 |
1.575 |
13.718 |
0.0025 |
y/n = yes versus no; OS = Overall survival; HR = Hazard ratio ; CI = Confidence interval ; PR = progesterone receptor; ER = estrogen receptor.
The patient group that underwent 18F-Fluoride PET/CT examination for staging had a median TLF10 of 4376.7 (SD = 1078.2; Minimum = 9.0; Maximum = 39,409.8). Likewise, the patient group that underwent 18F-Fluoride PET/CT examination for restaging had a median TLF10 = 3040.9 (SD = 4572.6; Minimum = 10.2; Maximum = 4,950.1). When comparing the staging and re-staging groups in terms of OS, PFS and TLF10 values there were no significant differences (p = 0.4894, p = 0.1593, p = 0.3591).
Higher TLF10 values (meaning more metastases) were associated with worst survival (Figure 1). A TLF10 cutoff of 3,700 separated two groups in terms of survival. Patients with TLF10 > 3,700 had a significantly higher risk of death (median OS = 8.5 months) while patients with TLF10 < 3,700 had a median OS of 33.4 months (p = 0.0002; HR = 6.569; 95% CI = 2.419–17.835) (Figure 2).
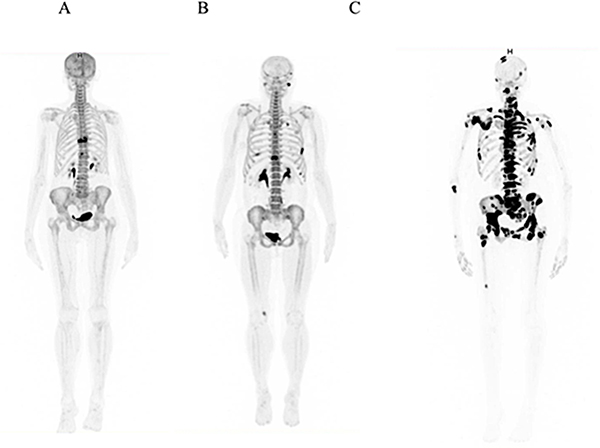
Figure 1: 18F-Fluoride PET/CT images of three women demonstrating differences in skeletal tumor burden extent and the outcome. (A) Image of a 70 yr-old patient with ductal breast cancer for 2.6 yrs demonstrating a metastasis in the 9th thoracic vertebrae on the 18F-Fluoride PET/CT. The skeletal tumor burden metrics was low (TLF10 = 641) and the patient remained 21 months with stable disease and event-free. (B) Image of a 43 yr-old woman with ductal breast cancer, diagnosed 3 months prior to 18F-Fluoride PET/CT images, demonstrating bone metastases in the spine, ribs and left temporal bone. Her skeletal tumor burden was intermediate (TLF10 = 1039.7) and although the patient indeed progressed, she was still alive after 17 months. (C) Image of a 63 yr-old woman with ductal breast cancer, diagnosed 4 months ago, and multiple metastasis. The skeletal tumor burden was extremely high (TLF10 = 39409). The patient progressed in 1.5 months and died in 2 months.
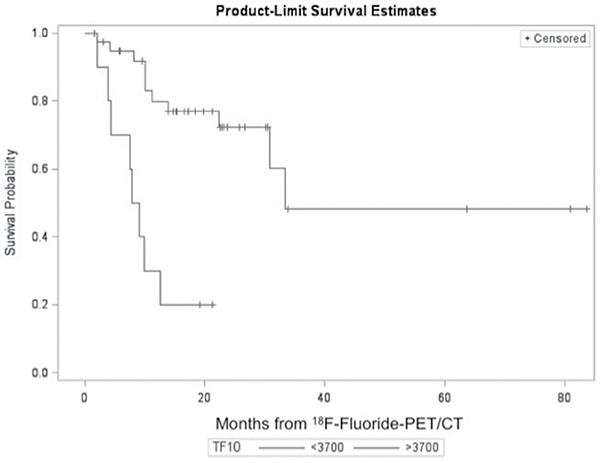
Figure 2: Overall survival according to TLF10 on 18F-Fluoride PET/CT. For TLF10 < 3700 the mean OS = 26.94 months (SD = 1.87) and median OS = 33.43 months. For TLF10 > 3700 the mean OS = 8.26 months (SD = 1.25) and median OS = 8.48 months.
TLF10 and PFS
At the end of follow-up, 32 patients (30%) progressed (eight had bone progression, four had nodal progression, 13 had visceral progression and seven had an increase in ECOG score by 2 points). Visceral metastases were located in the lungs and liver. Among these patients, 27 had bone metastasis prior to progression, one patient had a liver metastasis and the remaining four patients were disease-free. The most common site of progression of the 27 patients with known bone metastasis was visceral disease. Visceral (lung and liver) metastases occurred in 13 patients.
The median PFS for patients with vs without bone metastases was 4.7 vs 12.2 months, respectively. Analyzing only the 49 patients with bone metastases at the baseline 18F-Fluoride PET/CT scan, the mean TLF10 was 2.5 times greater for patients that progressed when compared to those that did not progress (TLF10 = 4,670 vs 1,831).
TLF10 was associated with PFS on univariable analyses (p < 0.0001; HR = 1.131; 95% CI = 1.068–1.198). The presence of bone metastases, visceral metastasis, negative progesterone receptor (PR), age and ECOG status also significantly correlated with PFS in the univariable analyses. All other parameters (HER2 status, ER status, Ki-67 index, time of disease, pain score, and treatments during the course of disease) did not correlate with PFS. On multivariable analyses however, TLF10 (p < 0.0001; OR = 1.120; 95% CI = 1.058–1.187) and a negative PR primary tumor status (p = 0.0413; HR = 2.266; 95% CI = 1.015–5.061) were again the only parameters associated with PFS (Table 3). Higher TLF10 values (meaning more metastases) were associated with higher risk of progressing (Figure 3). A TLF10 cutoff of 1,815 separated two groups in terms of progression (25.8 vs 4.13 months) (p = < 0.0001; HR = 5.384; 95% CI = 2.339–12.395).
Table 3: Correlation of clinical, laboratory and imaging variables to progression-free survival
Variables |
HR |
95% CI |
p-value |
|
|---|---|---|---|---|
Univariable analyses |
||||
Age |
0.970 |
0.941 |
0.999 |
0.0424 |
Time of disease |
0.987 |
0.923 |
1.058 |
0.7110 |
Primary stage (III/IV vs I/II) |
1.946 |
0.836 |
4.528 |
0.1225 |
HER2 |
1.657 |
0.792 |
3.511 |
0.1874 |
ER status |
1.301 |
0.494 |
3.423 |
0.5939 |
PR status |
2.808 |
1.323 |
5.957 |
0.0071 |
Ki-67 |
1.015 |
0.998 |
1.032 |
0.0868 |
Radiotherapy (y/n) |
1.485 |
0.688 |
3.208 |
0.3138 |
Hormonal therapy (y/n) |
1.002 |
0.445 |
2.256 |
0.9961 |
Surgery (y/n) |
1.372 |
0.610 |
3.086 |
0.4442 |
ECOG status |
2.278 |
1.102 |
4.706 |
0.0262 |
Pain score |
1.450 |
0.696 |
3.022 |
0.3212 |
Visceral metastases |
4.641 |
2.327 |
9.258 |
< 0.0001 |
Bone metastases |
8.873 |
3.692 |
21.325 |
< 0.0001 |
hSUV |
1.009 |
0.941 |
0.999 |
0.2073 |
Mean10 |
0.957 |
0.880 |
1.041 |
0.3098 |
TLF10 |
1.131 |
1.068 |
1.198 |
< 0.0001 |
Multivariable analysis |
||||
TLF10 |
1.120 |
1.058 |
1.187 |
< 0.001 |
PR status |
2.266 |
1.015 |
5.061 |
0.0413 |
y/n = yes versus no; OS = Overall survival; HR = Hazard ratio ; CI = Confidence interval ; PR = progesterone receptor; ER = estrogen receptor.
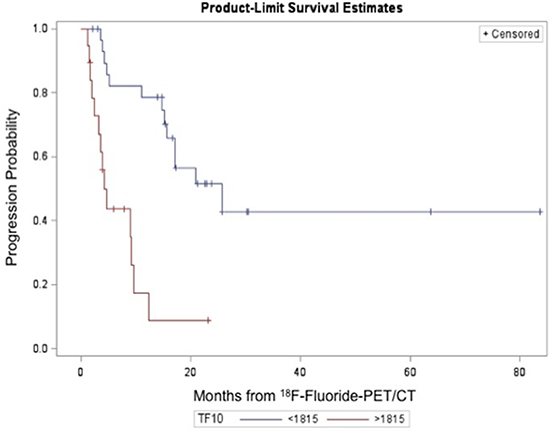
Figure 3: Progression probability according to TLF10 on 18F-Fluoride PET/CT. For TLF10 < 1815 the mean PFS = 19.01 months (SD = 1.66) and median PFS = 25.80 months. For TLF10 > 1815 the mean PFS = 6.16 months (SD = 0.99) and median PFS = 4.13 months.
Relation to TTBE
Bone events occurred in 12 patients (11.2%) and these were: spinal cord compression (2 patients), pathologic bone fracture (8 patients), surgical intervention (1 patient) and intractable bone pain (1 patient). The median TTBE was 9.8 months. The presence of bone metastasis (p = 0.0267; HR = 4.390; 95% CI = 1.186–16.244) and negative PR status (p = 0.0227; HR = 5.406; 95% CI = 1.267–23.075) were significant risk factors for developing a bone event. No other parameters (including TLF10) correlated with TTBE. On multivariable analyses again only the presence of bone metastasis and negative PR status were significantly associated with TTBE (p = 0.0448 and p = 0.0072, respectively) (Table 4).
Table 4: Correlation of clinical, laboratory and imaging variables to bone event
Variables |
HR |
95% CI |
p-value |
|
|---|---|---|---|---|
Univariable analyses |
||||
Age |
0.992 |
0.940 |
1.046 |
0.7594 |
Time of disease |
1.097 |
0.989 |
1.217 |
0.0814 |
Primary stage (III/IV vs I/II) |
1.053 |
0.261 |
4.246 |
0.9422 |
HER2 |
2.650 |
0.513 |
13.685 |
0.2445 |
ER status |
0.996 |
0.121 |
8.200 |
0.9971 |
PR status |
5.406 |
1.267 |
23.075 |
0.0227 |
Ki-67 |
1.009 |
0.969 |
1.051 |
0.6686 |
Radiotherapy (y/n) |
- |
- |
- |
0.0502 |
Hormonal therapy (y/n) |
2.795 |
0.348 |
22.445 |
0.3336 |
Surgery (y/n) |
- |
- |
- |
0.5081 |
ECOG status |
1.728 |
0.451 |
6.625 |
0.4252 |
Pain score |
1.052 |
0.253 |
4.293 |
0.9435 |
Visceral metastases |
1.608 |
0.345 |
7.496 |
0.5454 |
Bone metastases |
4.390 |
1.186 |
16.244 |
0.0267 |
hSUV |
0.995 |
0.967 |
1.024 |
0.7318 |
Mean10 |
0.986 |
0.879 |
1.107 |
0.8155 |
TLF10 |
1.082 |
0.987 |
1.186 |
0.0913 |
Multivariable analysis |
||||
Bone metastases |
1.118 |
1.003 |
1.247 |
0.0448 |
PR status |
10.454 |
1.890 |
57.824 |
0.0072 |
y/n = yes versus no; OS = Overall survival; HR = Hazard ratio ; CI = Confidence interval ; PR = progesterone receptor; ER = estrogen receptor.
DISCUSSION
Previous reports have demonstrated that skeletal tumor burden on 18F-Fluoride PET/CT, quantified by the simple method of obtaining the TLF10 (SUVmax threshold = 10) is a strong and independent prognostic biomarker in prostate cancer patients undergoing 223Ra [9]. To our knowledge, there have not been prior studies describing that skeletal tumor burden on 18F-Fluoride PET/CT is an independent prognostic biomarker in breast cancer patients. Actually, the few studies conducted to identify PET parameters that predict survival in metastatic breast cancer were performed with 18F-FDG PET or PET/CT. These studies (with 18F-FDG PET/CT) have demonstrated that total lesion glycolysis bears a strong correlation to OS [13, 14]. The only other investigation evaluating the prognostic role of 18F-Fluoride PET/CT that we found was conducted by Piccardo et al. in 32 breast cancer patients [12]. Although the authors did not discover a strong and independent association of 18F-Fluoride PET/CT with OS, their study was the first to attempt to use semi-quantitative parameters for this purpose. The discrepancy among their findings and ours may be due to the method of tumor burden quantification. We used the TLF10 parameter since we have conducted extensive studies with this metrics. We established the ideal cut-off values to separate normal bone from lesions and proved it a valuable independent prognostic imaging biomarker to predict OS in prostate cancer patients [9, 15].
In the clinical setting, while it seems obvious that breast cancer patients with very low bone tumor burden will have better outcomes than those patients with high tumor burden, it is still relevant to increase awareness by a scientific approach as opposed to mere observation. We found that the median overall survival was 15.2 months for patients with bone metastasis vs 23.4 months for patients without bone metastasis. Visual analysis of the presence vs absence of bone metastases also demonstrates a significant and high likelihood of death in patients presenting with bone metastases (p = 0.007; HR = 6.461). However, on a multivariable model, visual analysis does not correlate with OS and only TLF10 can independently define which patients have worst prognosis.
We did not decide on performing 18F-Fluoride PET/CT over 18F-FDG PET/CT in these breast cancer patients. We performed 18F-Fluoride PET/CT over conventional bone scintigraphy because of the higher sensitivity to detect bone lesions. In fact, 18.7% of these women were also submitted to 18F-FDG PET/CT scans during treatment, to evaluate response to therapy. However, the determination of whole-body tumor burden 18F-FDG PET/CT scans using TLG and MTV parameters in metastatic breast cancer patients (especially with bone lesions) is not feasible on a daily basis. Since in breast cancer patients, osteoblastic bone metastases predominate, we envisioned that the determination of skeletal tumor burden with 18F-Fluoride PET/CT might be a substitute for whole-body 18F-FDG tumor burden calculations in daily clinical practice.
Clinical, laboratory and imaging parameters are used to prognosticate patients with limited and advanced breast cancer. However, these parameters cannot be used independently. At initial staging of patients, ECOG status, primary tumor histology, serum laboratory measurements, tumor markers and conventional images have relevant prognostic value. Worse prognosis is associated with absence of hormone receptors, Her2-neu gene amplification and high percentage of Ki-67 positive cells [16]. However, these variables (clinical, laboratory and imaging) could lose the ability to be independent prognostic biomarkers as the disease becomes advanced. For example, Piccardo et al. [12] have found that in breast cancer patients with bone metastases, the 18F-FDG PET/CT findings have a stronger prognostic impact in OS with an independent association than conventional clinical and biological prognostic factors. Likewise, we demonstrated that among all variables evaluated (as ECOG status, pain score, treatments, presence of visceral metastases, patient age, time of cancer), only the PR status (at initial diagnosis) and the quantitative (i.e., objective) volumetric analysis (TLF10) of bone tumor burden (during the course of disease) independently separated survivors from non-survivors. The mean TLF10 of patients that were alive at the end of follow-up was four times lower than the TLF10 of the 19 patients that were dead (1,562 vs 6,288). With a cutoff TLF10 value of 3,700 there was a significant difference in survival (specificity = 93.3%). Furthermore, the prognostic impact of skeletal tumor burden (TLF10) was high for both staging and restaging in patients with bone metastases. Therefore, since skeletal tumor burden calculation will relate to OS and PFS (in both staging and restaging settings), it may help define future therapeutic strategies.
TFL10 was also an independent predictor of PFS in breast cancer patients, even among patients with visceral disease progression. Using the cutoff TLF10 value of 1,815 discriminated patients that were more likely to progress.
Earlier studies report bone events occurring in nearly 50% of patients with breast cancer with a median TTBE of 5.5 months [17, 18]. In our population however, only 12 patients (11.2%) had bone events and among these, nine of 49 (18%) had BE due to bone metastasis; the remaining three patients (without bone metastases) developed pathological fractures because of osteoporosis during follow-up. The median TTBE in our study was 9.8 months. This discrepancy of findings between the literature and ours may be due to differences in treatment of bone metastases, nowadays with more advanced drugs that protect bones from fractures. The TLF10 value (i.e. the determination of skeletal tumor burden) was not an indicator of TTBE. However, the presence of bone metastases increased 4 times the risk of developing a bone event.
One limitation of our study was its retrospective nature with patients undergoing multiple treatment regimens. However, because of the large sample size (107 patients) we were able to evaluate the bone burden of breast cancer patients with a variety of lesions, ranging from none to a near super-scan.
MATERIALS AND METHODS
Study design
The local Institutional Review Board approved this retrospective study (#46/2016) of patients with breast cancer that underwent whole-body 18F-Fluoride PET/CT images for investigation of bone metastases.
Patient population
Inclusion criteria consisted of histologically confirmed breast cancer patients, above 18 years, that underwent 18F-Fluoride PET/CT. All patients were followed-up for at least 12 months or until death. We excluded patients whose imaging study could not be retrieved and also patients lost to follow-up after the collection of the 18F-Fluoride PET/CT data.
18F-Fluoride PET/CT
All patients underwent a true whole-body PET/CT acquisition on two PET/CT scanners (Siemens Biograph True-Point PET/CT 64 or Siemens Biograph PET/CT 16, Siemens Healthcare, USA) 45 minutes after intravenous injection of 3.7MBq/kg of 18F-sodium fluoride. CT parameters included 5mm axial reconstruction and 120 kV or dose care kV tube voltage. PET images were acquired in 3-dimensional mode using 90s/bed position.
18F-Fluoride PET/CT Interpretation and Quantification
All 18F-Fluoride PET/CT images were blindly interpreted by three Nuclear Medicine physicians with over 12 years of experience with PET/CT images. All 18F-Fluoride PET/CT quantitative analyses were performed by two nuclear medicine physicians with 5 and 12 years of experience with PET/CT images, respectively.
Quantitative interpretation was performed on all 18F-Fluoride PET/CT images to determine whole-body skeletal tumor burden. 18F-Fluoride PET/CT images were quantified using METAVOL® software [19]. To calculate the skeletal tumor burden, a threshold for SUVmax = 10 to exclude normal bone was used, the details of the quantification is described in our previous study [15]. After processing the following parameters were automatically provided by the software:
hSUV: the highest SUVmax among all the metastases, Mean10: the mean SUVmax of all metastases, FTV10: the total volume of fluoride-avid bone metastases (in milliliters). This calculation is equivalent to the calculation of metabolic tumor volume (MTV) on 18F-FDG PET/CT images, TLF10: the skeletal tumor burden (VOI10x Mean10) i.e., the total activity of 18F-Fluoride-avid metastases. This calculation is comparable to the calculation of total lesion glycolysis (TLG) on 18F-FDG PET/CT images.
Statistical analyses
The following information of each patient was correlated with the skeletal tumor burden parameters: age, years of cancer, initial clinical stage, presence of bone metastases, presence of visceral metastases, primary tumor characteristics (Ki-67, hormone receptor status, HER-2, histology), previous treatments and clinical evaluation using performance status scale (ECOG) [20] and pain scale [21]. We did not collect CA15-3 and CA27.29 values at diagnosis or to monitor recurrence because it is not recommended by the American Society of Clinical Oncology [22]. Visceral metastases were evaluated by conventional CT scans of the chest, abdomen and pelvis or by the PET/CT scans (whether with 18F-FDG or 18F-sodium fluoride).
The primary end-point was overall survival (OS), established from date of 18F-Fluoride PET/CT until date of death from any cause, censoring data on last follow-up of living patients. Secondary end-points were progression free-survival (PFS) and time to bone event (TTBE). PFS was defined as length of time from the 18F-Fluoride PET/CT image until the date of objective tumor progression or death of any cause. Objective tumor progression was defined as a new lesion (whether bone or soft tissue or visceral) or a lesion that increased in size (RECIST criteria) leading to a change in current therapy or initiation of another therapy. TTBE was defined from the date of 18F-Fluoride PET/CT until the date of a bone event (surgical intervention, spinal cord compression, pathologic fracture, bone pain or rapid lesion progression requiring immediate intervention).
Numerical variables were described as mean value, standard deviation, minimum and maximum and median values, and categorical variables were described with absolute and percentage frequency. To evaluate the relationship between the variables and outcomes as predictors of survival the cox proportional hazards regression was applied. ROC curve was used to determine the cutoff points for measuring the TLF10 and the Kaplan-Meier survival curves to demonstrate survival time distributions. The level of significance was set at 5%.
CONCLUSIONS
The skeletal tumor burden determined with 18F-Fluoride-PET/CT is a powerful prognostic biomarker of OS and PFS in breast cancer patients. While the simple presence of bone metastases is associated with worst prognosis we have demonstrated that, among all patients with bone metastases, it is possible to objectively discriminate which ones will have worst outcome. This may help improve treatment strategies for breast cancer patients. To understand the relevance of our findings, more studies are necessary to evaluate if the skeletal tumor burden metrics will ultimately alter these treatment strategies.
Abbreviations
OS: Overall survival; TLG: Total lesion glycolysis; MTV: Metabolic tumor volume; PFS: Progression free-survival; TTBE: Time to bone event; TLF10: Skeletal Tumor Burden; PR: Progesterone receptor.
Author’s contributions
Conception and design: Elba C. Etchebehere; Collection and assembly of data: Ana E. Brito, Elba C. Etchebehere, Mariana Lima, Celso D. Ramos and Camila Mosci; Data analysis and interpretation: Ana E. Brito, Elba C. Etchebehere, Allan Santos, Paulo Oliveira, Tiago Souza, Barbara Amorim. Provision of study materials or patients: André Deeke Sasse and Cesar Cabello. Manuscript writing: All authors. Final approval of manuscript: All authors.
Ethical approval
The local Institutional Review Board approved this retrospective study (#46/2016).
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
ACKNOWLEDGMENTS
We thank the Institute of Research on Nuclear Energy (IPEN) for providing UNICAMP with the sodium fluoride-18F in order to perform the PET/CT scans. We are also grateful for the advice, availability and support of Dr. Kenji Hirata and his team, who developed Metavol.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
Fundacao de Amparo de Pesquisa do Estado de Sao Paulo (FAPESP). Faculdade de Ciências Médicas da UNiversitatde de Campinas (FCM - UNICAMP).
REFERENCES
1. Glendenning J, Cook G. Imaging breast cancer bone metastases: current status and future directions. Semin Nucl Med. 2013; 43:317–23.
2. Fogelman I, Cook G, Israel O, Van der Wall H. Positron emission tomography and bone metastases. Semin Nucl Med. 2005; 35:135–42.
3. Yamashita K, Koyama H, Inaji H. Prognostic significance of bone metastasis from breast cancer. Clin Orthop Relat Res. 199589–94.
4. Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001; 27:165–76.
5. Gradishar WJ, Anderson BO, Balassanian R, Blair SL, Burstein HJ, Cyr A, Elias AD, Farrar WB, Forero A, Giordano SH, Goetz M, Goldstein LJ, Hudis CA, et al. NCCN Guidelines Insights Breast Cancer, Version 1.2016. J Natl Compr Canc Netw. 2015; 13:1475–85.
6. Segall G, Delbeke D, Stabin MG, Even-Sapir E, Fair J, Sajdak R, Smith GT, and SNM. SNM practice guideline for sodium 18F-fluoride PET/CT bone scans 1.0. J Nucl Med. 2010; 51:1813–20.
7. Bortot DC, Amorim BJ, Oki GC, Gapski SB, Santos AO, Lima MC, Etchebehere EC, Barboza MF, Mengatti J, Ramos CD. 18F-Fluoride PET/CT is highly effective for excluding bone metastases even in patients with equivocal bone scintigraphy. Eur J Nucl Med Mol Imaging. 2012; 39:1730–36.
8. Hillner BE, Siegel BA, Hanna L, Duan F, Quinn B, Shields AF. 18F-fluoride PET used for treatment monitoring of systemic cancer therapy: results from the National Oncologic PET Registry. J Nucl Med. 2015; 56:222–28.
9. Etchebehere EC, Araujo JC, Fox PS, Swanston NM, Macapinlac HA, Rohren EM. Prognostic Factors in Patients Treated with 223Ra: The Role of Skeletal Tumor Burden on Baseline 18F-Fluoride PET/CT in Predicting Overall Survival. J Nucl Med. 2015; 56:1177–84.
10. Carkaci S, Sherman CT, Ozkan E, Adrada BE, Wei W, Rohren EM, Mawlawi OR, Ueno NT, Buchholz TA, Yang WT. (18)F-FDG PET/CT predicts survival in patients with inflammatory breast cancer undergoing neoadjuvant chemotherapy. Eur J Nucl Med Mol Imaging. 2013; 40:1809–16.
11. Gallamini A, Zwarthoed C, Borra A. Positron Emission Tomography (PET) in Oncology. Cancers (Basel). 2014; 6:1821–89.
12. Piccardo A, Puntoni M, Morbelli S, Massollo M, Bongioanni F, Paparo F, Altrinetti V, Gonella R, Gennari A, Iacozzi M, Sambuceti G, DeCensi A. 18F-FDG PET/CT is a prognostic biomarker in patients affected by bone metastases from breast cancer in comparison with 18F-NaF PET/CT. Nucl Med (Stuttg). 2015; 54:163–72.
13. Marinelli B, Espinet-Col C, Ulaner GA, McArthur HL, Gonen M, Jochelson M, Weber WA. Prognostic value of FDG PET/CT-based metabolic tumor volumes in metastatic triple negative breast cancer patients. Am J Nucl Med Mol Imaging. 2016; 6:120–27.
14. Son SH, Lee SW, Jeong SY, Song BI, Chae YS, Ahn BC, Lee J. Whole-Body Metabolic Tumor Volume, as Determined by (18)F-FDG PET/CT, as a Prognostic Factor of Outcome for Patients With Breast Cancer Who Have Distant Metastasis. AJR Am J Roentgenol. 2015; 205:878–85.
15. Rohren EM, Etchebehere EC, Araujo JC, Hobbs BP, Swanston NM, Everding M, Moody T, Macapinlac HA. Determination of Skeletal Tumor Burden on 18F-Fluoride PET/CT. J Nucl Med. 2015; 56:1507–12.
16. Fitzgibbons PL, Page DL, Weaver D, Thor AD, Allred DC, Clark GM, Ruby SG, O’Malley F, Simpson JF, Connolly JL, Hayes DF, Edge SB, Lichter A, Schnitt SJ. Prognostic factors in breast cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med. 2000; 124:966–78.
17. Jensen AØ, Jacobsen JB, Nørgaard M, Yong M, Fryzek JP, Sørensen HT. Incidence of bone metastases and skeletal-related events in breast cancer patients: a population-based cohort study in Denmark. BMC Cancer. 2011; 11:29.
18. Plunkett TA, Smith P, Rubens RD. Risk of complications from bone metastases in breast cancer. implications for management. Eur J Cancer. 2000; 36:476–82.
19. Hirata K, Kobayashi K, Wong KP, Manabe O, Surmak A, Tamaki N, Huang SC. A Semi-Automated Technique Determining the Liver Standardized Uptake Value Reference for Tumor Delineation in FDG PET-CT. PLoS One. 2014; 9:e105682.
20. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, Carbone PP. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982; 5:649–55.
21. World Health Organization. Traitement de la douleur cancéreuse. Geneva; 1987.
22. Harris L, Fritsche H, Mennel R, Norton L, Ravdin P, Taube S, Somerfield MR, Hayes DF, Bast RC Jr, and American Society of Clinical Oncology. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J Clin Oncol. 2007; 25:5287–312.