
Introduction
There is a consensus that post-mastectomy radiotherapy (PMRT) is indicated for the breast cancer with locally advanced disease (T3-T4), or four or more positive axillary lymph nodes (LNs) [1, 2]. Additionally, based on the results of a recent meta-analysis [3], PMRT can be applied to one to three positive axillary LNs.
On the other hand, mastectomy is generally considered a sufficient local treatment method for node-negative breast cancer. Nevertheless, a high rate of local recurrence has been reported in a subset of patients with aggressive clinicopathologic factors such as young age, large tumor size, high tumor grade, lymphovascular invasion (LVI), or positive/close resection margin [4]. As the understanding of the molecular biology of breast cancer improves, the biological subtype is receiving attention as a possible prognostic factor with which to distinguish patients with a high versus low risk of local recurrence [5-7]. In the setting of mastectomy, however, the effects of the biological subtype on local recurrence are not consistent [5, 8-10].
The purpose of this study was to identify the risk factors for locoregional recurrence (LRR) and any first recurrence (AFR) in node-negative patients treated with mastectomy but not PMRT, thus defining a subgroup of patients who may benefit from PMRT.
Results
Patient and tumor characteristics
The median follow-up period was 5.9 years (range: 0.7-10.4 years). Table 1 summarizes the patient and tumor characteristics. Adjuvant systemic treatment was delivered at the physician’s discretion. A total of 182 patients (10.0%) received no systemic treatment. A total of 966 patients (52.8%) received adjuvant chemotherapy; 772 received an anthracycline-based regimen; 126 received a combination regimen comprising cyclophosphamide, methotrexate, and 5-fluorouracil; and only 31 received a taxane-containing regimen. A total of 1,260 patients (68.9%) received endocrine treatment. Among 467 HER2+ patients, only 107 (22.9%) were confirmed to have been treated with trastuzumab (not done, n = 292; unknown, n = 68). Among 255 triple negative (TN) patients, 193 (75.7%) were treated with cytotoxic chemotherapy (not done, n = 62).
Table 1: Patient, tumor, and treatment characteristics (n = 1,828)
Variables |
n |
% |
Age, median (range) |
51 (22-87) |
|
Menopausal status |
||
Premenopausal |
852 |
46.6 |
Postmenopausal |
848 |
46.4 |
Unknown |
128 |
7.0 |
Histology |
||
IDCa |
1695 |
92.7 |
Others |
133 |
7.3 |
T stage |
||
T1 |
1141 |
62.4 |
T2 |
687 |
37.6 |
Tumor histologic grade |
||
Low-intermediate |
1076 |
58.9 |
High |
671 |
36.7 |
Unknown |
81 |
4.4 |
Resection margin |
||
Negative (≥2mm) |
1400 |
76.6 |
Close (<2mm) |
415 |
22.7 |
Positive |
11 |
0.6 |
Unknown |
2 |
0.1 |
Axillary management |
||
SLNBx |
912 |
49.9 |
ALND |
914 |
50.0 |
Not done |
2 |
0.1 |
Number of nodes examined |
||
Median, SLNBx |
4 (0-43) |
|
Median, ALND |
11 (1-48) |
|
<10 |
1157 |
63.3 |
≥10 |
662 |
36.2 |
Unknown |
9 |
0.5 |
Hormonal receptor |
||
Positive |
1265 |
69.2 |
Negative |
563 |
30.8 |
HER2 status |
||
Positive |
467 |
25.5 |
Negative |
1189 |
65.0 |
Unknown (all IHC2+, FISH not done) |
172 |
9.4 |
Systemic treatment |
||
Endocrine therapy alone |
680 |
37.2 |
Chemotherapy alone |
386 |
21.1 |
Both |
580 |
31.7 |
Neither |
182 |
10.0 |
Trastuzumab on HER2(+) |
||
Trastuzumab(+) |
107 |
5.9 |
Trastuzumab(-) |
292 |
16.0 |
unknown |
68 |
3.7 |
Biological subtype |
||
Luminal A |
719 |
39.3 |
Luminal B |
162 |
8.9 |
Luminal HER2 |
201 |
11.0 |
HER2+ |
266 |
14.6 |
Triple negative |
255 |
13.9 |
Unknown |
225 |
12.3 |
Abbreviations: IDCa = infiltrating ductal carcinoma; SLNBx = sentinel lymph node biopsy; ALND = axillary lymph node dissection; IHC = immunohistochemical staining; FISH = fluorescence in situ hybridization.
Locoregional recurrence
Of all 1,828 patients, 52 developed LRR. There were 31 (59.6%) ipsilateral chest wall recurrences, 28 (53.8%) ipsilateral LN recurrences (axillary, 18; internal mammary, 7; supraclavicular, 8; site unspecified, 2), and 7 (13.4%) ipsilateral chest wall and nodal recurrences. The cumulative rates for LRR at 5, 7, and 10 years were 2.8%, 3.8%, and 3.8%, respectively.
When performing univariate and multivariate analysis, patients with unknown information were not included, and the factors associated or marginally associated with each end point by univariate analysis were subject to multivariate analysis.
On univariate analysis, an age of ≤ 40 years (p < 0.001) and T2 stage (p = 0.006) were significantly associated with a high risk of LRR, and the biological subtype was marginally associated with high LRR. With respect to the biologic subtypes, the 7-year cumulative incidence of LRR was 2.2% for luminal A, 7.0% for luminal B, 5.1% for luminal HER2, 4.4% for HER2+, and 5.1% for TN (p = 0.095). The use of trastuzumab in patients with HER2+ did not affect LRR (Table 2). On multivariate analysis (Table 3), an age of ≤ 40 years (HR, 3.3; p < 0.001) and T2 stage (HR, 1.3; p = 0.013) were independently associated with a high risk of LRR.
Table 2: Univariate analysis for locoregional recurrence, distant metastasis, any first recurrence, and overall mortality
Variables |
Total (n= 1828) |
Locoregional recurrence (n= 52) |
p |
Distant metastasis (n= 61) |
p |
Any first recurrence (n= 98) |
p |
Any death (n= 44) |
p |
Age |
|||||||||
≤40 years |
255 |
17 |
0.000 |
14 |
0.053 |
28 |
0.000 |
7 |
0.721 |
>40 years |
1573 |
35 |
47 |
70 |
37 |
||||
T stage |
|||||||||
T1 |
1141 |
23 |
0.006 |
20 |
0.000 |
40 |
0.000 |
19 |
0.011 |
T2 |
687 |
29 |
41 |
58 |
25 |
||||
Resection margin |
|||||||||
Negative |
1400 |
35 |
0.124 |
45 |
0.620 |
70 |
0.240 |
33 |
0.910 |
Close+positive |
426 |
17 |
16 |
28 |
11 |
||||
Unknown * |
2 |
0 |
0 |
0 |
0 |
||||
Axillary dissection |
|||||||||
SLNBx |
912 |
25 |
0.994 |
25 |
0.273 |
43 |
0.404 |
22 |
0.481 |
ALND |
914 |
27 |
36 |
55 |
22 |
||||
not done * |
2 |
0 |
0 |
0 |
0 |
||||
Chemotherapy |
|||||||||
Yes |
966 |
30 |
0.642 |
44 |
0.006 |
65 |
0.017 |
24 |
0.941 |
No |
862 |
22 |
17 |
33 |
20 |
||||
HER2 status |
|||||||||
Negative |
1189 |
36 |
0.637 |
44 |
0.763 |
70 |
0.701 |
25 |
0.205 |
Positive & trastuzumab(+) |
107 |
2 |
2 |
4 |
1 |
||||
Positive & trastuzumab(-) |
292 |
11 |
11 |
19 |
10 |
||||
Positive & trastuzumab(unknown) * |
68 |
1 |
3 |
3 |
3 |
||||
Unknown * |
172 |
2 |
1 |
2 |
5 |
||||
Tumor histologic grade |
|||||||||
Low-intermediate |
1076 |
26 |
0.259 |
27 |
0.009 |
46 |
0.011 |
19 |
0.026 |
High |
671 |
22 |
32 |
47 |
23 |
||||
Unknown * |
81 |
4 |
2 |
5 |
2 |
||||
Biological subtype |
|||||||||
Triple negative |
255 |
12 |
0.075 |
16 |
0.011 |
24 |
0.006 |
12 |
0.009 |
Others |
1401 |
38 |
44 |
72 |
27 |
||||
Unknown * |
172 |
2 |
1 |
2 |
5 |
||||
Luminal A |
719 |
14 |
0.095 |
15 |
0.004 |
25 |
0.000 |
7 |
0.011 |
Luminal B |
162 |
8 |
11 |
18 |
5 |
||||
Luminal HER2 |
201 |
7 |
8 |
12 |
6 |
||||
HER2+ |
266 |
7 |
8 |
14 |
8 |
||||
Triple negative |
255 |
12 |
16 |
24 |
12 |
||||
Unknown * |
225 |
4 |
3 |
5 |
6 |
Abbreviations: SLNBx = sentinel lymph node biopsy; ALND = axillary lymph node dissection
* Patients with unknown information were not included in statistical analyses.
Table 3: Multivariate analysis for locoregional recurrence, any first recurrence, and distant metastasis
Variable |
Locoregional recurrence |
Distant metastasis |
Any first recurrence |
|||
Hazard ratio (95% CI) |
p |
Hazard ratio (95% CI) |
p |
Hazard ratio (95% CI) |
p |
|
Age (>40 years vs. ≤40 years) |
3.290 (1.792-6.041) |
0.000 |
1.951 (1.068-3.563) |
0.030 |
2.606 (1.661-4.090) |
0.000 |
T stage (1 vs. 2) |
1.279 (1.053-1.554) |
0.013 |
1.482 (1.234-1.779) |
0.000 |
1.304 (1.132-1.502) |
0.000 |
Biologic subtype (others vs. triple negative) |
- |
- |
1.632 (1.011-2.636) |
0.045 |
||
Tumor grade (low-intermediate vs. high) |
- |
- |
- |
|||
Chemotherapy (yes vs. no) |
- |
- |
- |
|||
Abbreviations: CI = confidence interval
Distant metastasis
Sixty-one patients developed distant metastasis (DM). Thirteen patients developed DM with synchronous LRR, and two patients developed DM 6 and 11 months after LRR. Forty-six patients had isolated DM. The cumulative rates for DM at 5, 7, and 10 years were 3.2%, 4.1%, and 5.3%, respectively.
Any first recurrence
In total, 98 cases developed AFR; 13 LRR with synchronous DM, 39 LRR without DM, and 46 DM only. Additional two DM was reported after the first recurrence, and the total cases of DM were 61. The cumulative rates for AFR at 5, 7 and 10 years were 5.3%, 6.7% and 7.9%, respectively. On univariate analysis (Table 2), an age of ≤ 40 years (p < 0.001), T2 stage (p < 0.001), a high tumor grade (p = 0.011), and biological subtype (p < 0.001) were significantly associated with a high risk of AFR. With respect to the biologic subtype, the 7-year cumulative incidence of AFR was 4.4% for luminal A, 13.9% for luminal B, 8.2% for luminal HER2, 7.2% for HER2+, and 9.1% for TN (p < 0.001). The use of trastuzumab in patients with HER2 and luminal HER2 subtypes was not associated with AFR (Table 2). To facilitate comparison between the groups in the multivariate analysis, these five subtypes were redefined as binary variables based on the results of the univariate analysis: TN tumors and others (p = 0.006). The use of chemotherapy was significantly associated with a high risk of AFR (p = 0.017), and this was attributed to the development of DM as a first recurrence. On multivariate analysis (Table 3), an age of ≤ 40 years (HR, 2.6; p < 0.001), T2 stage (HR, 1.3; p < 0.001), and the TN biological subtype (HR, 1.6; p = 0.045) were independently associated with a high risk of AFR.
Table 4: Recurrences in pT1-2N0 patients treated with mastectomy without post-mastectomy radiotherapy (studies performed after 1990s) [4]
10-year locoregional recurrence rate |
10-year Any first recurrence rate |
|||||||||
author |
year |
n |
Median follow-up |
Overall |
High risk group |
Overall |
High risk group |
Definition of high risk |
||
Truong [16] |
1989-1999 |
1505 |
7.0 Years |
7.8% |
21.2% |
- |
- |
LVI, Grade 3 |
||
Yildirim [12] |
1990-2004 |
502 |
6.4 Years |
≤40 Years |
7.0% (6.4 Years) |
53.0% |
19.0% (total) |
- |
LVI, size >2 cm |
|
>40 Years |
1.7% (6.4 Years) |
33.0% |
- |
LVI, size >3 cm, Grade 3 |
||||||
Sharma [11]* |
1997-2002 |
753 |
7.5 years |
2.1% |
18.6% |
8.6% |
- |
T2N0, age ≤40 years |
||
Truong [10] |
1998-2009 |
1994 |
4.3 Years |
1.8%-3.1% (5 Years) |
12.5% (5 Years) |
- |
- |
TN, close/positive RM |
||
Our study |
2005-2011 |
1828 |
6.9 Years |
3.8% |
12.4% |
LVI, size >2 cm |
||||
7.9% |
18.1% |
LVI, size >2 cm, TN |
||||||||
Abbreviations: LVI = lympho-vascular invasion; TN = tripe negative; RM = resection margin
* Patients with pN1 were included in the study.
Overall mortality
In total, 44 patients died, and 29 of them had developed tumor recurrence before death. The cumulative rates for overall mortality at 5, 7, and 10 years were 1.8%, 2.9%, and 3.6%, respectively.
Identification of patients at high risk of LRR and AFR
To identify patients at higher risk of recurrence, we defined subgroups according to risk factors proven on multivariate analysis for LRR and ARF.
For LRR, patient age ( ≤ 40 vs. > 40 years) and tumor size (T1 vs. T2) were used to stratify the risk groups. Of all 1,828 patients, 974 (53.3%) had no risk factors, 766 (41.9%) had one risk factor, and 88 (4.8%) had two risk factors. The 5-year cumulative LRR rates were 1.6% with no risk factors, 3.2% with one risk factor, and 12.4% with two to three risk factors. The latter was defined as the high-risk group for LRR. The 7-year and 10-year cumulative LRR rates were 2.5% with no risk factors, 4.5% with one risk factor, and 12.4% with two risk factors (Figure 1).
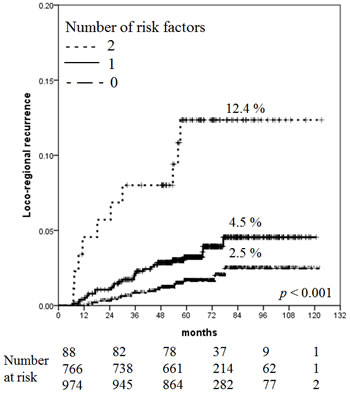
Figure 1: Increased risk of LRR with increasing number of risk factors.
For ARF, three risk factors were used to stratify the risk groups: patient age, tumor size, and biological subtype. Of 1,656 analyzable patients (172, unknown), 748 (45.2%) had no risk factors and 694 (41.9%), 194 (11.7%), and 20 (1.2%) patents had one, two, and three risk factors, respectively. Because of the small number of patients with three risk factors, patients with two to three risk factors were assigned to the high-risk group (214, 12.9%). The 5-year cumulative ARF rates were 2.8% with no risk factors, 5.9% with one risk factor, and 14.7% with two to three risk factors. The 7-year cumulative ARF rates were 3.9% with no risk factors, 8.4% with one risk factor, and 15.7% with two to three risk factors (Figure 2). The 10-year cumulative ARF rates were 3.9% with no risk factors, 10.6% with one risk factor, and 18.1% with two to three risk factors.
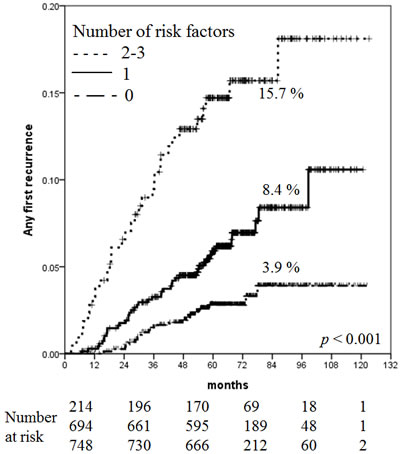
Figure 2: Increased risk of AFR with increasing number of risk factors.
The effect of chemotherapy regimen
We performed an additional analysis comparing anthracycline-based chemotherapy (772 out of 966, 80%) and other regimens. There was no difference in LRR (p = 0.150), DM (p = 0.543), AFR (p = 0.829), and OS (p = 0.334) between two groups.
Discussion
The present study showed that the 7-year overall incidence of LRR was 3.8% in patients with pT1-2N0 breast cancer treated with mastectomy but not PMRT. Additionally, the 7-year LRR rate of patients aged less than or equal to 40 years with T2 tumors, who were considered at high risk, was 12.4%. Since no LRR was reported after 7 years, the LRR rate at 7-year and 10-year were identical (Figure 1). These results are in agreement with those of recent studies (Table 4).
The indications for PMRT have traditionally been based on the risk of LRR. Although numerous studies have reported the prognostic value of clinicopathologic factors predicting LRR, such as patient age, menopausal status, tumor size, tumor grade, LVI, or resection margin status, variation exists in terms of the significance or magnitude of those factors in the setting of mastectomy without PMRT for pT1-2N0. Among them, young age and large tumor size, which were proven as significant prognostic factors in our analysis, are widely accepted variables associated with a high rate of LRR. With respect to patient age, Sharma et al. [11], Karlsson et al. [6], and Yildirim et al. [12] identified an age of ≤ 40 years as an independent predictor of high LRR, and Abi-Raad et al. [13] and Wallgren et al. [14] reported ages of ≤ 50 and ≤ 60 years as cutoffs, respectively. Similarly, Jagsi et al. [15] showed that a premenopausal status was an independent predictor of LRR. Regarding tumor size, T2 tumors (≥ 2 cm) were the most commonly reported cutoff point predicting a high risk of LRR [14-16].
Although the EBCTCG adopted AFR (irrespective of LRR or DM) as the primary endpoint for the effect of RT in patients with breast cancer [17], there are little data regarding AFR in mastectomy without PMRT among patients with pT1-2N0 cancer. We performed an analysis using AFR as another primary endpoint and stratified the risk groups based on three factors proven to be significant in the multivariate analysis: age of ≤ 40 years, T2 tumors, and TN subtype. The 10-year AFR rate of the high-risk groups with two to three adverse factors was 18.1%. There are scarce data with which to directly compare our findings.
Notably, the EBCTCG meta-analysis reported that LRR and AFR occurred more frequently in the no-RT group treated with axillary sampling than in the no-RT group treated with axillary dissection; however, the difference disappeared when PMRT was added, irrespective of axillary management. In contrast, we found no difference in the LRR or AFR rate according to axillary management. Moreover, the 10-year LRR and AFR rates were far superior to the outcomes of the EBCTCG in node-negative patients (the 10-year AFR and LRR rates were 7.9% and 3.8%, respectively). Even for the high-risk group defined in our study, the 10-year AFR and LRR rates were 18.1% and 12.4%, respectively. Considering the period of patient enrollment (1964-1986 in the EBCTCG meta-analysis vs. 2005-2011 in our study), it is reasonable that this reduction in recurrence is attributable to improved nodal examination, such as sentinel LN detection or pathologic evaluation, and progress in systemic treatments such as HER2 targeted therapy. Importantly, routine use of systemic treatment, which was given to 90% of our study cohort, could also explain these superior outcomes, in that recent large clinical trials emphasized the impact of systemic treatment in terms of not only DM and survival, but also local control [18-20].
We defined the high-risk group as described above and found a high rate of recurrence in that subset. The remaining question is how many recurrences justify the recommendation for PMRT. Olivotto and Truong suggested that PMRT is indicated when LRR exceeds 25%, but not when it is < 10%, based on the magnitude of absolute LRR reduction and the absolute survival benefit (4:1 ratio according to the EBCTCG) [21]. If the LRR rate is 12.8% (the 10-year rate in our high-risk group), patients’ priorities and preferences should be considered when making decisions regarding PMRT. The EBCTCG suggested a new ratio: for every 1.5 patients in whom AFR is avoided at 10 years, there is an additional survivor at 20 years [17]. This works well for pT1-2N1 patients with mastectomy, but not for pT1-2N0 patients, as previously described [3]. Despite the reduction in AFR by PMRT (34.2% in no-RT vs. 22.1% in RT at 10 years, 2p = 0.0003) in patients who underwent mastectomy and only axillary sampling, breast cancer mortality did not differ (35.8% in no-RT vs. 32.0% in RT at 20 years, 2p > 0.1). Even if PMRT reduced the AFR rate of 18.1% (the 10-year rate in our high-risk group) to a certain degree, it is reasonable that the absolute survival benefit would be small. This small survival benefit cannot be considered as grounds for routine use of PMRT for all high-risk patients with pT1-2N0 cancer. However, considering that most patients in our high-risk group were aged ≤ 40 years, even a small survival benefit may be important. Furthermore, the reduction in LRR or AFR would enable patients to work and live without a disease burden.
It is important to recognize the limitations of this study, including those inherent to retrospective studies. First, the follow-up period was not long enough to show all recurrences considering the long natural history of breast cancer. This might weaken the study’s statistical power. Second, our study could not directly address the survival benefits in association with reductions in the LRR or AFR by PMRT, because our data regarding patient death included all-cause mortality rather than breast cancer mortality. Despite these limitations, our study is clinically valuable. Although breast-conserving treatment has been generalized for node-negative breast cancer over the past several years, some patients still undergo mastectomy for various reasons, such as the presence of multifocal breast cancer or the patient’s preference for breast reconstruction after mastectomy. However, most such reference studies were performed from the 1960s to the 1990s. The present work was a multi-institutional study performed in the 2000s and included a large number of patients with pT1-2N0 breast cancer (n = 1,828) treated with mastectomy without PMRT. The conclusions that can be drawn from our analyses are more relevant to contemporary practice, in that we adopted current diagnostic and therapeutic strategies.
This analysis was performed only in the population who did not receive radiation after mastectomy, prospective study to compare those who received PMRT to those who did not is being planned. Furthermore, the study regarding hypofractionated RT after mastectomy could be considered. Some investigators have suggested that hypofractionated RT is also an alternative option for PMRT [22], although it has not been thoroughly studied as in post-breast conserving surgery RT [23-25].
In conclusion, our study found that the overall recurrence and LRR rates were substantially low in patients with pT1-2N0 breast cancer treated with mastectomy and systemic therapy without PMRT. This finding shows that mastectomy without PMRT is a sufficient local treatment for pT1-2N0M0 breast cancer. However, there was a patient group at high risk for recurrence: the 7-year LRR rate in patients aged ≤ 40 years with T2 tumors was 12.4%, and the 7-year AFR rate of patients with two to three adverse factors, among those aged ≤ 40 years, T2 tumors and the TN subtype, was 15.7%. PMRT might be considered for these high-risk patients.
Materials and Methods
This multi-institutional retrospective study was approved by the Korean Radiation Oncology Group (KROG 14-22) and the Institutional Review Board of each of 10 participating institutions in Korea. After obtaining this approval, we reviewed the medical records of patients with breast cancer treated by mastectomy from 2005 to 2010. The eligibility criteria were (1) a tumor size of ≤ 5 cm (pT1 and pT2), (2) negative LNs (pN0) proven by axillary dissection or sentinel LN biopsy, and (3) no treatment with adjuvant PMRT. The exclusion criteria were (1) male gender, (2) the presence of distant metastasis (DM) at diagnosis, (3) neoadjuvant systemic treatment, (4) a history of radiotherapy (RT) to the chest or neck, (5) a history of malignancies other than papillary/follicular thyroid cancer, and (6) bilateral breast cancer. We identified 1,842 patients according to these eligibility criteria. We then excluded 14 patients who were lost to follow-up < 6 months from the mastectomy date. Finally, 1,828 patients with breast cancer were included in this study.
The collected clinicopathological information was presented in Table 1. Positivity of ER, PR, HER2, and Ki-67 was determined by immunohistochemical staining. HER2-positivity was defined as a 3+ immunohistochemical result or a 2+ immunohistochemical result, confirmed by fluorescence in situ hybridization. Using the histologic grade as a surrogate for Ki-67 based on the St. Gallen Expert Consensus [14], we approximated five breast cancer subtypes based on hormone receptor (ER and PR) status, HER2 status, and histologic grade: luminal A (ER+ or PR+/HER2−/low-intermediate grade), luminal B (ER+ or PR+/HER2−/high grade), HER2+ (ER−/PR−/HER2+), luminal HER2 (ER+ or PR+/HER2+), and triple-negative (TN) (ER−/PR−/HER2−).
The primary endpoints were AFR and LRR. AFR was defined as the first tumor recurrence, irrespective of LRR or DM. LRR was defined as any LRR as a first event with or without synchronous DM. Diagnosis of DM within 3 months of an LRR was considered synchronous. LRR occurring after DM was not considered as an LRR event. LRR indicated tumor recurrence in the ipsilateral chest wall; ipsilateral axillary, infraclavicular, internal mammary, or supraclavicular node recurrence; or a combination of these. DM indicated tumor recurrence outside regions identified as LRR sites. The secondary endpoints were DM and overall mortality. The information on date of death was taken from Korea’s national database, in which death by breast cancer is not distinguished from death by other causes. Time to any recurrence or death was measured from the date of mastectomy.
Cumulative incidence function curves for AFR, LRR, DM, and overall mortality were constructed using the Kaplan-Meier method, and comparisons between groups were performed using log-rank tests. A Cox proportional hazards model was used to estimate hazard ratios (HRs), and to identify correlations between outcomes and risk variables. All statistical analyses were carried out with SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). P values < 0.05 were considered statistically significant.
Acknowledgments
This work was supported by Research Resettlement Fund for the new faculty of Seoul National University.
Conflicts of interest
The authors declare that they have no conflict of interest.
References
1. Recht A, Edge SB, Solin LJ, Robinson DS, Estabrook A, Fine RE, Fleming GF, Formenti S, Hudis C, Kirshner JJ, Krause DA, Kuske RR, Langer AS, et al. Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol. 2001; 19:1539-69.
2. Gradishar WJ, Anderson BO, Balassanian R, Blair SL, Burstein HJ, Cyr A, Elias AD, Farrar WB, Forero A, Giordano SH, Goetz M, Goldstein LJ, Hudis CA, et al. Invasive Breast Cancer Version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2016; 14:324-54.
3. Sharma A, Digumarthy SR, Kalra MK, Lanuti M, Shepard JA. Reversible locoregional lymph node enlargement after radiofrequency ablation of lung tumors. AJR Am J Roentgenol. 2010; 194:1250-6.
4. Kent C, Horton J, Blitzblau R, Koontz BF. Whose Disease Will Recur After Mastectomy for Early Stage, Node-Negative Breast Cancer? A Systematic Review. Clin Breast Cancer. 2015; 15:403-12.
5. Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005; 365:1687-717.
6. Karlsson P, Cole BF, Price KN, Coates AS, Castiglione-Gertsch M, Gusterson BA, Murray E, Lindtner J, Collins JP, Holmberg SB, Fey MF, Thurlimann B, Crivellari D, et al. The role of the number of uninvolved lymph nodes in predicting locoregional recurrence in breast cancer. J Clin Oncol. 2007; 25:2019-26.
7. Arvold ND, Taghian AG, Niemierko A, Abi Raad RF, Sreedhara M, Nguyen PL, Bellon JR, Wong JS, Smith BL, Harris JR. Age, breast cancer subtype approximation, and local recurrence after breast-conserving therapy. J Clin Oncol. 2011; 29:3885-91.
8. Voduc KD, Cheang MC, Tyldesley S, Gelmon K, Nielsen TO, Kennecke H. Breast cancer subtypes and the risk of local and regional relapse. J Clin Oncol. 2010; 28:1684-91.
9. Selz J, Stevens D, Jouanneau L, Labib A, Le Scodan R. Prognostic value of molecular subtypes, ki67 expression and impact of postmastectomy radiation therapy in breast cancer patients with negative lymph nodes after mastectomy. Int J Radiat Oncol Biol Phys. 2012; 84:1123-32.
10. Truong PT, Sadek BT, Lesperance MF, Alexander CS, Shenouda M, Raad RA, Taghian AG. Is biological subtype prognostic of locoregional recurrence risk in women with pT1-2N0 breast cancer treated with mastectomy? Int J Radiat Oncol Biol Phys. 2014; 88:57-64.
11. Sharma R, Bedrosian I, Lucci A, Hwang RF, Rourke LL, Qiao W, Buchholz TA, Kronowitz SJ, Krishnamurthy S, Babiera GV, Gonzalez-Angulo AM, Meric-Bernstam F, Mittendorf EA, et al. Present-day locoregional control in patients with t1 or t2 breast cancer with 0 and 1 to 3 positive lymph nodes after mastectomy without radiotherapy. Ann Surg Oncol. 2010; 17:2899-908.
12. Yildirim E, Berberoglu U. Can a subgroup of node-negative breast carcinoma patients with T1-2 tumor who may benefit from postmastectomy radiotherapy be identified? Int J Radiat Oncol Biol Phys. 2007; 68:1024-9.
13. Abi-Raad R, Boutrus R, Wang R, Niemierko A, Macdonald S, Smith B, Taghian AG. Patterns and risk factors of locoregional recurrence in T1-T2 node negative breast cancer patients treated with mastectomy: implications for postmastectomy radiotherapy. Int J Radiat Oncol Biol Phys. 2011; 81:e151-7.
14. Wallgren A, Bonetti M, Gelber RD, Goldhirsch A, Castiglione-Gertsch M, Holmberg SB, Lindtner J, Thurlimann B, Fey M, Werner ID, Forbes JF, Price K, Coates AS, et al. Risk factors for locoregional recurrence among breast cancer patients: results from International Breast Cancer Study Group Trials I through VII. J Clin Oncol. 2003; 21:1205-13.
15. Jagsi R, Raad RA, Goldberg S, Sullivan T, Michaelson J, Powell SN, Taghian AG. Locoregional recurrence rates and prognostic factors for failure in node-negative patients treated with mastectomy: implications for postmastectomy radiation. Int J Radiat Oncol Biol Phys. 2005; 62:1035-9.
16. Truong PT, Lesperance M, Culhaci A, Kader HA, Speers CH, Olivotto IA. Patient subsets with T1-T2, node-negative breast cancer at high locoregional recurrence risk after mastectomy. Int J Radiat Oncol Biol Phys. 2005; 62:175-82.
17. Early Breast Cancer Trialists’ Collaborative G, Darby S, McGale P, Correa C, Taylor C, Arriagada R, Clarke M, Cutter D, Davies C, Ewertz M, Godwin J, Gray R, Pierce L, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011; 378:1707-16.
18. Ragaz J, Jackson SM, Le N, Plenderleith IH, Spinelli JJ, Basco VE, Wilson KS, Knowling MA, Coppin CM, Paradis M, Coldman AJ, Olivotto IA. Adjuvant radiotherapy and chemotherapy in node-positive premenopausal women with breast cancer. N Engl J Med. 1997; 337:956-62.
19. Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, Andersson M, Kamby C, Kjaer M, Gadeberg CC, Rasmussen BB, Blichert-Toft M, Mouridsen HT. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999; 353:1641-8.
20. Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F, Kjaer M, Gadeberg CC, Mouridsen HT, Jensen MB, Zedeler K. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med. 1997; 337(14):949-55.
21. Olivotto IA, Truong PT, Chua B. Postmastectomy radiation therapy: who needs it? J Clin Oncol. 2004; 22:4237-9.
22. Kouloulias V, Mosa E, Zygogianni A, Kypraiou E, Georgakopoulos J, Platoni K, Antypas C, Kyrgias G, Tolia M, Papadimitriou C, Psyrri A, Patatoukas G, Dilvoi M, et al. A Retrospective Analysis of Toxicity and Efficacy for 2 Hypofractionated Irradiation Schedules Versus a Conventional One for Post-Mastectomy Adjuvant Radiotherapy in Breast Cancer. Breast Care (Basel). 2016; 11:328-32.
23. START Trialists’ Group, Bentzen SM, Agrawal RK, Aird EG, Barrett JM, Barrett-Lee PJ, Bentzen SM, Bliss JM, Brown J, Dewar JA, Dobbs HJ, Haviland JS, Hoskin PJ, et al. The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet. 2008; 371:1098-107.
24. Kang JK, Kim MS, Jang WI, Seo YS, Kim HJ, Cho CK, Yoo HJ, Paik EK, Cha YJ, Song HJ. The clinical utilization of radiation therapy in Korea between 2009 and 2013. Radiat Oncol J. 2016; 34:88-95.
25. Kim KS, Shin KH, Choi N, Lee SW. Hypofractionated whole breast irradiation: new standard in early breast cancer after breast-conserving surgery. Radiat Oncol J. 2016; 34:81-7.