
INTRODUCTION
Brain metastases are frequent findings in lung cancer patients, accounting for about 14% of newly diagnosed patients [1–2]. Particularly in lung adenocarcinoma, the rate of brain metastases has been reported to be up to 43% [3]. Lung cancers without distant metastases are potentially curable. Hence, accurate localization of brain metastatic lesions may lead to better selection of curative therapy or palliation.
Pretreatment imaging procedures for the evaluation of brain metastatic lesions in lung cancer patients remain controversial issue. In the guidelines of the European Respiratory Society, brain computed tomography (CT) is recommended in all lung cancer patients with neurological symptoms [4]. However, the diagnostic capability of brain CT in patients without neurological abnormalities is still not clear. The use of 18fluorodeoxyglucose positron emission tomography (18FDG PET)-CT is more efficient to detect distant metastases than the use of conventional imaging procedures [5]. However, 18FDG PET or PET-CT has limited diagnostic performance in the evaluation of brain metastatic lesions, mainly because of its difficulties in differentiating FDG-avid metastases from the normal surrounding hyper-metabolic parenchyma in brain tissue [6]. Magnetic resonance imaging (MRI) has been put forward as another one-stop-shop imaging technique for M staging of lung cancer patients [7, 8]. Compared with PET-CT, brain MRI has the potential to detect more brain metastatic lesions in lung cancer patients [7–9]. However, the application of a meta-analysis to directly compare the diagnostic capability of PET/PET-CT and MRI for the assessment of brain metastases in lung cancer patients has not been explored. In this study, we conducted a meta-analysis of available studies to systematically assess and compare their abilities for diagnosing brain metastatic lesions of lung cancer patients.
RESULTS
Study selection and description
The electronic search yielded 264 abstracts; Among 264 abstracts, we found that 11 articles were potentially eligible. After we read the full texts of these articles, 6 of the 11 relevant articles were excluded. The search and screening of relevant studies is summarised in Figure 1. Consequently, 5 studies [7, 8, 10–12] involving 941 patients were eligible for this meta-analysis (Figure 1). Characteristics of each eligible study are presented in Table 1. The total number of patients in a single study ranged from 52 to 442 (median, 165 patients). The reported age range was from 23 to 88 years. All studies were of the prospective design. In three studies (307 patients) [7, 8, 10], only non-small cell lung cancer patients were enrolled, in one study (442 patients) [12], only lung adenocarcinoma patients were enrolled, and in the last study (203 patients) [11], all pathological types of lung cancer patients were enrolled.
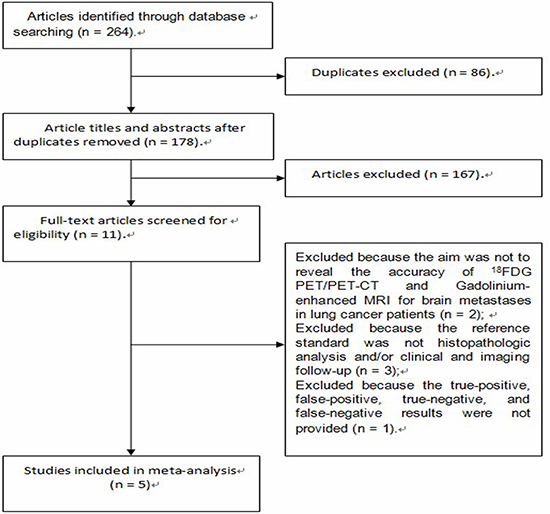
Figure 1: Flow chart of study selection.
Table 1: The clinical characteristics of 18FDG PET/PET-CT and Gadolinium-enhanced MRI
Study |
Origin |
No. of Patients |
Age(y) |
Male (%) |
Follow-up Time |
MRI |
PET-CT |
||
|---|---|---|---|---|---|---|---|---|---|
Strengthen |
Sequences |
CE-CT |
Analysis Methods |
||||||
Ohno [11], 2007 |
Japan |
90 |
35–83 |
53.3 |
≥ 24 months |
1.5T |
T1,T2, CE-T1, FLAIR |
No |
QL |
Plathow [10], 2008 |
Germany |
52 |
49–71 |
69.2 |
Unclear |
1.5T |
T1,T2, CE-T1, STIR |
Enhanced by iodinated contrast agent |
QL + QN |
Yi [7], 2008 |
Korea |
165 |
34–82 |
75.8 |
592 days (mean) |
3.0T |
T1,T2, CE-T1 |
No |
QL |
Ohno [8], 2008 |
Japan |
203 |
47–85 |
53.7 |
≥ 12 months |
1.5T |
T1,T2, CE-T1, STIR |
No |
QL |
Lee [12], 2009 |
Korea |
442 |
23–88 |
53.8 |
≥ 30 months |
3.0T |
T1,T2, CE-T1, FLAIR |
No |
QL + QN |
Abbreviations: QL = qualitative; QN = quantitative; CE = contrast enhanced; STIR = short time inversion recovery; FLAIR = fluid-attenuation inversion-recovery.
Study quality
The results and Criteria of the methodological quality were presented in Table 2. Main disagreements were related to external validity (EV) 5, internal validity (IV) 3, and IV5. All studies had the valid reference tests (IV1). However, the reference tests were based in part on a comparison of initial and follow-up images in all studies [7, 8, 10–12] (IV3). In four studies [7, 8, 10, 12], the interpretation of 18F-FDG PET/CT was conducted without knowing any clinical information (IV5). In three studies [7, 8, 12], eligible patients were enrolled consecutively (EV5).
Table 2: Quality assessment of the 5 included articles in this meta-analysis
Study |
Internal Validity Criteria |
External Validity Criteria |
No. of items assessed as “yes” in the criteria |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
IV1 |
IV2 |
IV3 |
IV4 |
IV5 |
IV6 |
EV1 |
EV2 |
EV3 |
EV4 |
EV5 |
EV6 |
||
Ohno [11], 2007 |
Yes |
Yes |
No |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
9 |
Plathow [10], 2008 |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
10 |
Yi [7], 2008 |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
11 |
Ohno [8], 2008 |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
11 |
Lee [12], 2009 |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
11 |
The Methodological Quality Criteria Recommended by the Cochrane Methods Working Group on Diagnostic Meta-analysis [20].
Internal Validity (IV):
1. Valid reference test (Biopsy, or imaging follow-up);
2. Blind measurement of PET/PET- CT or MRI without knowledge of reference test results;
3. Blind measurement of reference test without knowledge of results of PET/PET-CT or MRI;
4. Assessment by reference test independent of results of PET/PET-CT or MRI;
5. PET/PET-CT or MRI interpreted independently of all clinical information (Mentioned in publication);
6. Prospective study (Mentioned in publication);
External Validity (EV):
1. Spectrum of disease (Primary stage of disease);
2. Demographic information (Age and sex information given);
3. Inclusion criteria (Mentioned in publication);
4. Exclusion criteria (Mentioned in publication);
5. Avoidance of selection bias (Consecutive series of patients);
6. Standard execution of PET/PET-CT or MRI (PET/PET-CT: Type of camera, dose of 18F-fluorodeoxyglucse, time interval, reconstruction; MRI: Strength, dose of contrast medium, sequences, reconstruction);
Summary estimates of sensitivity, specificity, DOR, PLR, and NLR
18FDG PET/PET-CT
The chi-square values of sensitivity, specificity, diagnostic odds ratio (DOR), positive likelihood ratio (PLR), and negative likelihood ratio (NLR) for 18FDG PET/PET-CT were 7.18 (p = 0.066 > 0.05), 1.39 (p = 0.709 > 0.05), 0.81 (p = 0.848 > 0.05), 0.23 (p = 0.973 > 0.05), and 2.73 (p = 0.435 > 0.05), respectively. The pooled sensitivity, specificity, DOR, PLR, and NLR values for 18FDG PET/PET-CT were 0.21 (95% confidence interval [CI] = 0.13 to 0.32), 1.00 (95% CI = 0.99 to 1.00), 235 (95% CI = 31 to 1799), 184.7 (95% CI = 24.8 to 1374.0), and 0.79 (95% CI = 0.70 to 0.89), respectively.
Gadolinium-enhanced MRI
The chi-square values of sensitivity, specificity, DOR, PLR, and NLR for Gadolinium-enhanced MRI were 7.87 (p = 0.097 > 0.05), 11.02 (p = 0.026 > 0.05), 2.08 (p = 0.026 < 0.05), 2.80 (p = 0.591 > 0.05), and 11.08 (p = 0.026 < 0.05), respectively. The pooled sensitivity, specificity, DOR, PLR, and NLR values for Gadolinium-enhanced MRI were 0.77 (95% CI = 0.60 to 0.89), 0.99 (95% CI = 0.97 to 1.00), 657 (95% CI = 112 to 3841), 149.6 (95% CI = 24.5 to 913.1), and 0.23 (95% CI = 0.12 to 0.43), respectively.
Summary receiver operating characteristic curves
The summary receiver operating characteristic (SROC) curves for 18FDG PET/PET-CT and Gadolinium-enhanced MRI were shown in Figures 2 and 3. The areas under the curve were 0.98 (95% CI = 0.96 to 0.89) and 0.97 (95% CI = 0.96 to 0.98), respectively.
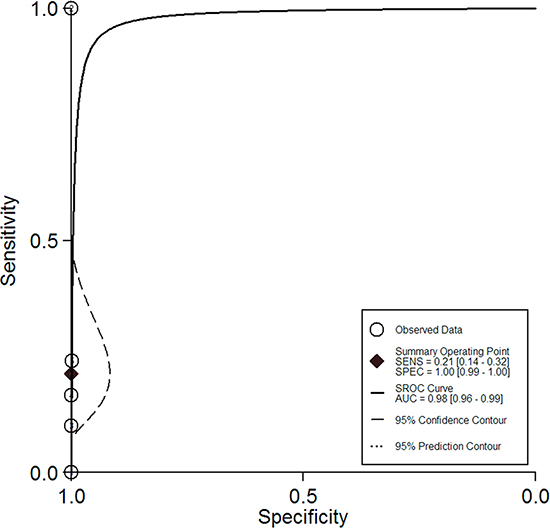
Figure 2: The summary receiver operating characteristic curve for the diagnostic performance of 18FDG PET/PET-CT.
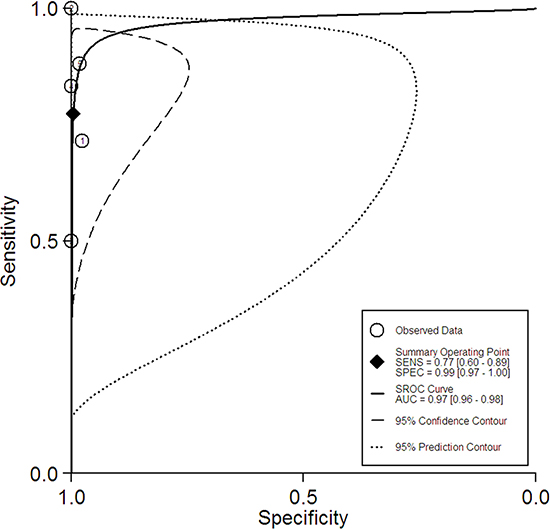
Figure 3: The summary receiver operating characteristic curve for the diagnostic performance of Gadolinium-enhanced MRI.
DISCUSSION
The brain is one of the most frequent distant-sites of lung cancer. Jena et al [13] reported that brain metastases accounted for 35.4% of patients with lung cancer (90% patients with IV-stage disease). In another study [14], brain metastases occurred in 11% of 442 lung cancer patients (28% patients with IV-stage disease). The median survival time of lung cancer patients with untreated brain metastatic lesions is less than three months, whereas the median survival time of lung cancer patients with brain metastases receiving palliative radiotherapy is about eight months [14, 15]. The brain is often the only site of distant metastatic disease [16]. Precise assessment of brain metastatic lesions can offer more opportunities to act early and elicit a better therapeutic effect.
Now the differences of the efficacy between PET/PET-CT and MRI for the assessment of brain metastatic lesions were still controversial. In this study, we obtained summary estimates and SROC curves for the clinical value of PET/PET-CT and MRI. 18FDG PET/PET-CT has limited diagnostic performance for the assessment of brain metastatic lesions. Gadolinium-enhanced MRI has higher sensitivity (77% vs 21%) than 18FDG PET/PET-CT. Gadolinium-enhanced MRI should be performed additionally to PET-CT for additional information to PET-CT in lung cancer patients with a curative option. It may, however, be noted that the high specificity of a positive PET/PET-CT finding may provide important clinical information in a setting where the brain is routinely included in the PET/PET-CT scan and contraindications for the apply of MRI.
The DOR is a single metric of test accuracy that combines sensitivity and specificity into a single number [17]. The higher value of DOR indicates better discriminatory test performance. The pooled DOR values for 18FDG PET/PET-CT and Gadolinium-enhanced MRI in this study were 235 and 657, indicating a higher level of accuracy for these two modalities. Likelihood ratios are also the indicators that take into account the interaction between the sensitivity and the specificity in their calculation. The values of PLR > 10 and NLR < 0.1 are considered convincing evidence to rule in or rule out disease [18, 19]. The pooled PLR values of for 18FDG PET/PET-CT and Gadolinium-enhanced MRI were 184.7 and 149.6, which were therefore high enough to diagnose brain metastatic lesions of lung cancer. The pooled NLR values for 18FDG PET/PET-CT and Gadolinium-enhanced MRI were 0.79 and 0.23, indicating that the negative results of these two modalities couldn’t be used alone to exclude brain metastatic lesions of lung cancer.
In this study, we searched with a systematic search strategy, selected available studies according to the strict criteria of inclusion, and assessed the methodological quality using uniform criteria. All these steps can increase the reliability of the results. However, several inevitable limitations must also be addressed when interpreting the results of this meta-analysis. First, imaging follow-up was used as one part of the reference standard in all studies. It might not correctly classify brain metastatic lesions in some patients with a refusal of biopsy. Besides, some parameters (such as pathological type, staging, diagnosis standards, glucose, radiotracer dose and uptake period of PET) were not considered in our study because of incomplete data. This may affect the accuracy of these two modalities. Third, publication bias was not tested because the few number of included studies may induce potential bias. Fourth, the MRI data in 4 of the 5 available studies is from the whole-body MRI procedures. The MRI technique of brain used in such whole-body protocols is probably not the most efficient protocol for the assessment of brain metastatic lesions. This may decrease the real sensitivity of gadolinium-enhanced MRI, which is compared to brain MRI examinations fully dedicated to brain metastatic lesions. Nevertheless, this will not change the final conclusion of this meta-analysis.
In conclusion, Gadolinium-enhanced MRI has higher sensitivity than 18FDG PET/PET-CT for the assessment of brain metastatic lesions in lung cancer patients. Gadolinium-enhanced brain MRI examinations may provide some additional information to 18FDG PET-CT for definitive exclusion of brain metastatic lesions.
MATERIALS AND METHODS
Literature search
A comprehensive literature search was performed to identify articles about the diagnostic capacity of 18FDG PET/PET-CT and Gadolinium-enhanced MRI for the assessment of brain metastatic lesions in lung cancer patients. The MEDLINE and EMBASE databases (last update December 2016) were used for searching relevant articles with the following combination of search terms: PET, “positron emission tomography”, MRI, “magnetic resonance imaging”, “distant metastases”, staging, “brain metastases”, NSLC, SLC, AND “lung cancer”. The sample search strategy is presented in Table 3. We had no language restrictions for searching and identifications relevant studies. To expand our search, references of relevant articles were screened for potentially suitable studies.
Table 3: The search strategy used for the MEDLINE and EMBASE databases
# |
Search string |
|---|---|
1 |
PET OR “positron emission tomography” |
2 |
MRI OR “magnetic resonance imaging” |
3 |
“distant metastases” OR staging OR “brain metastases” |
4 |
NSLC OR SLC OR “lung cancer” |
5 |
#1 AND #2 AND #3 AND #4 |
Study selection
Studies comparing the accuracy of 18FDG PET/PET-CT and Gadolinium-enhanced MRI for the assessment of brain metastatic lesions in lung cancer patients were eligible for inclusion. Studies with the data on a per-patient analysis were included. Studies with only one imaging modality (PET/PET-CT or MRI) were excluded. Review articles, editorials, abstracts, case reports, and guidelines for management and studies with less than ten participants were excluded. Studies were excluded if brain metastases were not confirmed by histopathologic analysis and/or imaging follow-up. Studies that didn’t provide sufficient data to construct a 2 × 2 contingency table for the calculation of sensitivity and specificity were also excluded. When data were presented in more than one article, the article with the largest number of patients or the article with the most details was chosen. Studies in which PET/PET-CT and MRI were not performed within one month of one another were also excluded.
Two reviewers (L.L, GQ.J) independently reviewed the titles and abstracts of the retrieved articles, applying the inclusion and exclusion criteria mentioned above. Articles were rejected if they were clearly ineligible. The same two reviewers (L.L, GQ.J) then independently reviewed the full-text version of the remaining articles to determine their eligibility for inclusion. Disagreements were resolved in consensus meetings.
Data extraction
Two reviewers (L.L, GQ.J) independently extracted the relevant data from each article and recorded these data on a standardized form. And any disagreement was resolved in consensus meetings. Data was extracted from the studies, including study authors , publication time, study design, number of participants, and imaging technical characteristics of 18FDG PET/PET-CT or Gadolinium-enhanced MRI, the reference standard, and totals of true positives, false positives, true negatives, and false negatives.
Quality assessment
We assessed the methodological quality of the included studies using the criteria list recommended by the Cochrane Methods Working Group on Diagnostic Meta-analysis [20]. Some items on the list for internal validity (IV) and external validity (EV) were modified for this meta-analysis (Table 2). Every criteria was assessed as ‘‘Yes’’ or ‘‘No’’.
Statistical analysis
Data on the diagnostic performance of PET/PET-CT and MRI were combined quantitatively across eligible studies. The degree of heterogeneity among eligible studies was reported using the chi-square statistic. The threshold for significance in this chi-square statistic was defined as p < 0.05. We calculated the sensitivities, specificities, positive likelihood ratios (PLR), negative likelihood ratios (NLR), and diagnostic odds ratios (DOR) with 95% confidence intervals (CI) for PET/PET-CT and MRI using the bivariate model [21]. This bivariate model allows for more between- and within-study variability than do the fixed-effect models. We also constructed the SROC curves to show the summary trade-off between sensitivity and specificity across the eligible studies and calculated the areas under curve for PET/PET-CT and MRI, respectively [22]. All analyses were performed using Stata version 12.0 (Stata Corporation, College Station, TX).
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Ferrigno D, Buccheri G. Cranial computed tomography as a part of the initial staging procedures for patients with non small cell lung cancer. Chest. 1994; 106:1025–1029.
2. Salbeck R, Grau HC, Artmann H. Cerebral tumor staging in patients with bronchial carcinoma by computed tomography. Cancer. 1990; 66:2007–2011.
3. Mujoomdar A, Austin JH, Malhotra R, Powell CA, Pearson GD, Shiau MC, Raftopoulos H. Clinical predictors of metastatic disease to the brain from non-small cell lung carcinoma: primary tumor size, cell type, and lymph node metastases. Radiology. 2007; 242: 882–888.
4. The American Thoracic Society and The European Respiratory Society. Pretreatment evaluation of non-small cell lung cancer. Am J Respir Crit Care Med. 1997;156:320–332.
5. Shim SS, Lee KS, Kim BT, Chung MJ, Lee EJ, Han J, Choi JY, Kwon OJ, Shim YM, Kim S. Non-small cell lung cancer: prospective comparison of integrated FDG PET/CT and CT alone for preoperative staging. Radiology. 2005; 236:1011–1019.
6. Marom EM, McAdams HP, Erasmus JJ, Goodman PC, Culhane DK, Coleman RE, Herndon JE, Patz EF Jr. Staging non-small cell lung cancer with whole-body PET. Radiology. 1999; 212:803–809.
7. Yi CA, Shin KM, Lee KS, Kim BT, Kim H, Kwon OJ, Choi JY, Chung MJ. Non-small cell lung cancer staging: efficacy comparison of integrated PET/CT versus 3.0-T whole-body MR imaging. Radiology. 2008; 248:632–642.
8. Ohno Y, Koyama H, Onishi Y, Takenaka D, Nogami M, Yoshikawa T, Matsumoto S, Kotani Y, Sugimura K. Non-small cell lung cancer: whole-body MR examination for M-stage assessment--utility for whole-body diffusion-weighted imaging compared with integrated FDG PET/CT. Radiology. 2008; 248:643–654.
9. Goeckenjan G, Sitter H, Thomas M, Branscheid D, Flentje M, Griesinger F, Niederle N, Stuschke M, Blum T, Deppermann KM, Ficker JH, Freitag L, Lübbe AS, et al. Prävention, Diagnostic, Therapie und Nachsorge des Lungenkarzinoms. Interdisziplin e S3-Leitlinie der Deutschen Gesellschaft für Pneumologie und Be -atmungsmedizin und der Deutschen Krebsgesell-schaft. Pneumologie. 2010; 64:e1–e164.
10. Plathow C, Aschoff P, Lichy MP, Eschmann S, Hehr T, Brink l, Claussen CD, Pfannenberg C, Schlemmer HP. Positron emission tomography/computed tomography and whole-body magnetic resonance imaging in staging of advanced non small cell lung cancer--initial results. Invest Radiol. 2008; 43:290–297.
11. Ohno Y, Koyama H, Nogami M, Takenaka D, Yoshikawa T, Yoshimura M, Kotani Y, Nishimura Y, Higashino T, Sugimura K. Whole-body MR imaging vs. FDG-PET: comparison of accuracy of M-stage diagnosis for lung cancer patients. J Magn Reson Imaging. 2007; 26:498–509.
12. Lee HY, Lee KS, Kim BT, Cho YS, Lee EJ, Yi CA, Chung MJ, Kim TS, Kwon OJ, Kim H. Diagnostic efficacy of PET/CT plus brain MR imaging for detection of extrathoracic metastases in patients with lung adenocarcinoma. J Korean Med Sci. 2009; 24:1132–1138.
13. Jena A, Taneja S, Talwar V, Sharma JB. Magnetic resonance (MR) patterns of brain metastasis in lung cancer patients: correlation of imaging findings with symptom. J Thorac Oncol. 2008; 3:140–144.
14. Sorensen JB, Hansen HH, Hansen M, Dombernowsky P. Brain metastases in adenocarcinoma of the lung: frequency, risk groups, and prognosis. J Clin Oncol. 1998; 6:1474–1480.
15. Zabel A, Milker-Zabel S, Thilmann C, Zuna I, Rhein B, Wannenmacher M, Debus J. Treatment of brain metastases in patients with non-small cell lung cancer (NSCLC) by stereotactic linac-based radiosurgery: prognostic factors. Lung Cancer. 2002; 37:87–94.
16. Yokoi K, Kamiya N, Matsuguma H, Machida S, Hirose T, Mori K, Tominaga K. Detection of brain metastasis in potentially operable non-small cell lung cancer: a comparison of CT and MRI. Chest. 1999; 115:714–719.
17. Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. 2003; 56:1129–1135.
18. Deeks JJ. Systematic reviews of evaluations of diagnostic and screening tests. In: Egger M, Smith GD, Altman DG, eds. Systematic reviews in health care: meta-analysis in context. London, UK: BMJ Publishing Group. 2001; 248–282.
19. Jaeschke R, Guyatt G, Lijmer J. Diagnostic tests. In: Guyatt G, Rennie D, eds. Users’ guides to the medical literature: a manual for evidence-based clinical practice. Chicago, IL: AMA Press. 2002; 121–140.
20. Wang HY, Ding HJ, Chen JH, Chao CH, Lu YY, Lin WY, Kao CH. Meta-analysis of the diagnostic performance of [18F]FDG-PET and PET/CT in renal cell carcinoma. Cancer Imaging. 2012; 12:464–474.
21. Chu H, Cole SR. Bivariate meta-analysis of sensitivity and specificity with sparse data: a general linear mixed model approach. J Clin Epidemiol. 2006; 59:1331–1332.
22. Jaeschke R, Guyatt GH, Sackett DL. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group. JAMA. 1994; 271:703–707.