
INTRODUCTION
Apoptosis plays an important role in cell fate and homeostasis which is a critically in biological process [1]. B cell lymphoma-2 (Bcl-2) is a important protein in apoptotic pathway, and is one of the most important oncogenes in the study of apoptosis. Bcl-2 mainly located on the mitochondrial outer membrane, or by the signal stimulation after the transfer to the mitochondrial outer membrane [2]. Currently research shows that cancer, neurodegenerative disorders, ischemia and autoimmune diseases are associated with Bcl-2 function abnormalities [3–5]. High expression of Bcl-2 is associated with different cancer types, and has been reported in esophageal cancer, non-small cell lung cancer, endometrial cancer, breast cancer, prostate cancer, lung cancer, chronic lymphocytic leukemia, diffuse large B-cell lymphoma etc [6–10]. There is increasing evidence that Bcl-2 gene polymorphism may be associated with cancer susceptibility and prognosis.
Human Bcl-2, located on chromosome 18q21.3, consists of two promoters, which called promoter 1 (P1) and promoter 2 (P2) [11]. P1 and P2 have different functions. More than 95% of the BCL-2 transcription is started by P1, it is at the initial point of about 1.7 KB upstream of translation, which has no typical TATA box, but have rich in GC box that can be combined with Sp-1. Also, P1 driven transcription mainly from GC box near the beginning, this is very similar with other housekeeping gene promoter. The chromosome structure of P1 analysis showed that it could be a constitutive promoter. P2 located downstream of the P1 at about 1.3kb (at translation starting point about 80bp upstream). Compared with P1, P2 is mainly an inducible promoter, and a small part of Bcl-2 transcription is driven by the P2 [12, 13]. Previous studies have identified rs2279115 which located in P2 promoter [14] have conflicting results between cancer susceptibility [15–36] and prognosis [15, 18, 19, 30, 37–46]. Furthermore, the correlation between rs1801018 single nucleotide polymorphisms (SNPs) and cancer susceptibility are somewhat contradictory [29, 30, 33, 36, 47].
To confirm whether Bcl-2 promoter polymorphisms are related to cancer, we performed this meta-analysis, aiming to measure the correlation between Bcl-2 promoter polymorphisms and cancer susceptibility and prognosis.
RESULTS
Studies retrieved and characteristics
Following an initial search, after duplicates removed, 189 studies were retrieved (PubMed: 173, Embase: 184). 6 review and 151 irrelevant studies and were excluded. Finally, 32 studies (6950 cases and 7984 controls) were chosen, and the data were extracted. A flow chart were carefully identified of the search process in Figure 1. The departure of Bcl-2 promoter polymorphisms frequencies from expectation under Hardy-Weinberg equilibrium (HWE) was assessed by chi-square in control group, and it was considered to be disequilibrium if P< 0.05. Six studies were excluded by HWE expectation (P< 0.05). The genotype distributions of all studies are summarized in Supplementary Table 1-3.
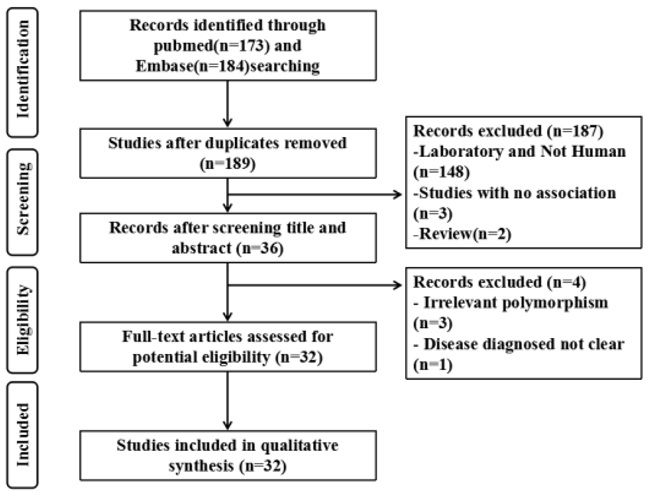
Figure 1: Flow diagram of the study selection process.
Overall, eighteen studies evaluating rs2279115 (6950 cases and 7984 controls) polymorphism in cancer susceptibility, three studies (1260 and 1440) evaluating rs1801018 polymorphism in cancer susceptibility, thirteen studies (4013 and 5319) evaluating rs2279115 polymorphism in cancer prognosis, and five studies (1889 and 2110) evaluating rs1801018 polymorphism in cancer prognosis. As for studies investigating the association between rs2279115 polymorphism and cancer susceptibility in cancer type, two studies evaluating rs2279115 polymorphism in cancer susceptibility in hematopoietic cancer and endocrine system cancer, three studies evaluating rs2279115 polymorphism in cancer susceptibility in digestive system cancers and respiratory cancer, four studies evaluating rs2279115 polymorphism in cancer susceptibility in breast Cancer. As for studies investigating the association between rs2279115 polymorphism and cancer susceptibility in ethnicity, eleven studies evaluating rs2279115 polymorphism in cancer susceptibility in Asia, seven studies evaluating rs2279115 polymorphism in cancer susceptibility in Caucasian. As for studies investigating the association between rs2279115 polymorphism and cancer prognostic in ethnicity, six studies evaluating rs2279115 polymorphism in cancer prognostic in Asia, seven studies evaluating rs2279115 polymorphism in cancer prognostic in Caucasian. Furthermore, three studies evaluating rs1801018 polymorphism in cancer susceptibility in Asia, and five studies evaluating rs1801018 polymorphism in cancer prognostic.
Meta-analysis of BCL-2 promoter polymorphisms and cancer susceptibility
Overall, our results showed that rs2279115 was correlated with a significantly higher risk of cancer susceptibility in allelic, dominant, recessive, and additive models(OR= 1.16, 95% CI:1.05,1.29, P= 0.004, allelic models respectively). However, rs1801018 had no correlation with the risk of cancer susceptibility in allelic, dominant, recessive, and additive models(OR= 1.48, 95% CI:0.90,2.44, P= 0.119, allelic model respectively) in Table 1.
Table 1: Meta-analysis of BCL-2 promoter polymorphisms and cancer risk
No.of |
PQ |
I2 |
OR |
95% CI |
PZ |
Model |
|
|---|---|---|---|---|---|---|---|
rs2279115 |
18(6950/7984) |
||||||
C vs. A |
0.000 |
74.4% |
1.16 |
1.05,1.29 |
0.004 |
Random-effects model |
|
CC+ CA vs. AA |
0.000 |
65.3% |
1.19 |
1.01,1.41 |
0.039 |
Random-effects model |
|
CC vs. CA+AA |
0.000 |
67.5% |
1.23 |
1.08,1.41 |
0.002 |
Random-effects model |
|
CC vs. CA |
0.004 |
53.8% |
1.20 |
1.07,1.35 |
0.003 |
Random-effects model |
|
rs1801018 |
3(1260/1440) |
||||||
A vs. G |
0.034 |
70.4% |
1.48 |
0.90,2.44 |
0.119 |
Random-effects model |
|
AA+AG vs. GG |
0.626 |
0.00% |
1.39 |
0.66,2.93 |
0.394 |
Fixed-effects model |
|
AA vs.AG+GG |
0.039 |
69.1% |
1.50 |
0.90,2.52 |
0.122 |
Random-effects model |
|
AA vs. AG |
0.057 |
65.0% |
1.46 |
0.89,2.39 |
0.134 |
Random-effects model |
|
Stratification was performed by cancer type, and a significant higher risk correlation between rs2279115 and cancer susceptibility was found in digestive system cancers and in allelic, dominant, recessive and additive models(OR= 1.31, 95% CI:1.18,1.45, P= 0.000, allelic model respectively), but not in breast Cancer (OR= 1.05, 95%CI:0.87,1.28, P=0.599, allelic model respectively), respiratory cancer (OR= 1.32, 95%CI:0.89,1.97, P=0.170, allelic model respectively) and Hematopoietic cancer(OR=1.19, 95%CI:0.78,1.81, P=0.418, allelic model respectively). Furthermore, we found rs2279115 was correlated with a significantly higher risk in endocrine system cancer risk in allelic (OR=1.34, 95%CI:1.06,1.71, P=0.016) and recessive model(OR=1.49, 95%CI:1.06,2.09, P=0.023), but not in dominant (OR=1.45, 95%CI:0.57,3.71, P=0.439) and additive model(OR=1.42, 95%CI:0.99,2.04, P=0.058). This is may because lack of large sample size in endocrine system cancer. Therefore, consider the inconsistency of these results, large sample size is needed in rs2279115 polymorphism and cancer susceptibility in different cancer type. Table 2 displays the results of subgroup analysis in cancer type.
Table 2: Meta-analysis of rs2279115 polymorphism and cancer risk in cancer type
rs2279115 |
No.of |
PQ |
I2 |
OR |
95% CI |
PZ |
Model |
|---|---|---|---|---|---|---|---|
Cancer type |
|||||||
Hematopoietic cancer |
2(333/333) |
||||||
C vs. A |
0.144 |
53.1% |
1.19 |
0.78,1.81 |
0.418 |
Random-effects model |
|
CC+ CA vs. AA |
0.586 |
0.00% |
0.99 |
0.63,1.57 |
0.978 |
Fixed-effects model |
|
CC vs. CA+AA |
0.130 |
56.4% |
1.40 |
0.75,2.63 |
0.296 |
Random-effects model |
|
CC vs. CA |
0.136 |
54.9% |
1.48 |
0.74,2.82 |
0.272 |
Random-effects model |
|
Digestive system cancers |
3(1628/1640) |
||||||
C vs. A |
0.610 |
0.00% |
1.31 |
1.18,1.45 |
<0.001 |
Fixed-effects model |
|
CC+ CA vs. AA |
0.371 |
0.00% |
1.30 |
1.07,1.58 |
0.008 |
Fixed-effects model |
|
CC vs. CA+AA |
0.756 |
0.00% |
1.51 |
1.31,1.74 |
<0.001 |
Fixed-effects model |
|
CC vs. CA |
0.701 |
0.00% |
1.47 |
1.27,1.72 |
<0.001 |
Fixed-effects model |
|
Endocrine system cancer |
2(210/435) |
||||||
C vs. A |
0.203 |
38.3% |
1.34 |
1.06,1.71 |
0.016 |
Fixed-effects model |
|
CC+ CA vs. AA |
0.045 |
75.1% |
1.45 |
0.57,3.71 |
0.439 |
Random-effects model |
|
CC vs. CA+AA |
0.649 |
0.00% |
1.49 |
1.06,2.09 |
0.023 |
Fixed-effects model |
|
CC vs. CA |
0.856 |
0.00% |
1.42 |
0.99,2.04 |
0.058 |
Fixed-effects model |
|
Breast Cancer |
4(1470/1628) |
||||||
C vs. A |
0.082 |
55.3% |
1.05 |
0.87,1.28 |
0.599 |
Random-effects model |
|
CC+ CA vs. AA |
0.005 |
76.5% |
1.16 |
0.69,1.96 |
0.577 |
Random-effects model |
|
CC vs. CA+AA |
0.574 |
0.00% |
1.07 |
0.92,1.25 |
0.374 |
Fixed-effects model |
|
CC vs. CA |
0.893 |
0.00% |
1.03 |
0.87,1.21 |
0.742 |
Fixed-effects model |
|
Respiratory cancer |
3(1537/2057) |
||||||
C vs. A |
0.000 |
92.6% |
1.32 |
0.89,1.97 |
0.170 |
Random-effects model |
|
CC+ CA vs. AA |
0.001 |
84.7% |
1.46 |
0.82,2.58 |
0.198 |
Random-effects model |
|
CC vs. CA+AA |
0.000 |
91.6% |
1.45 |
0.86,2.46 |
0.163 |
Random-effects model |
|
CC vs. CA |
0.000 |
86.9% |
1.37 |
0.88,2.14 |
0.163 |
Random-effects model |
|
Stratification was performed by ethnicity, rs2279115 was correlated with a significantly higher risk of cancer susceptibility in Asia (OR= 1.28, 95% CI:1.11,1.48, P= 0.001, allelic models respectively) but not in Caucasian (OR=1.01, 95% CI:0.85,1.21, P=0.879, allelic models respectively) in allelic, dominant, recessive, and additive models. Simultaneously, rs1801018 had no correlation with the risk of cancer susceptibility in Asia in allelic, dominant, recessive, and additive models(OR= 1.48, 95% CI:0.90,2.44, P= 0.119, allelic model respectively). There is lack of data in Caucasian. Table 3 displays the results of subgroup analysis in ethnicity.
Table 3: Meta-analysis of rs2279115 polymorphism and cancer risk in ethnicity
rs2279115 |
No.of |
PQ |
I2 |
OR |
95% CI |
PZ |
Model |
|---|---|---|---|---|---|---|---|
Ethnicity |
|||||||
Asia |
11(3869/4717) |
||||||
C vs. A |
0.000 |
76.2% |
1.28 |
1.11,1.48 |
0.001 |
Random-effects model |
|
CC+ CA vs. AA |
0.000 |
70.6% |
1.39 |
1.07,1.82 |
0.014 |
Random-effects model |
|
CC vs. CA+AA |
0.000 |
70.9% |
1.39 |
1.16,1.67 |
<0.001 |
Random-effects mode |
|
CC vs. CA |
0.005 |
60.0% |
1.33 |
1.13,1.57 |
0.001 |
Random-effects mode |
|
Caucasian |
7(3081/3267) |
||||||
C vs. A |
0.075 |
56.6% |
1.01 |
0.85,1.21 |
0.879 |
Random-effects mode |
|
CC+ CA vs. AA |
0.076 |
56.4% |
1.01 |
0.74,1.40 |
0.931 |
Random-effects mode |
|
CC vs. CA+AA |
0.337 |
11.2% |
1.03 |
0.89,1.19 |
0.710 |
Fixed-effects model |
|
CC vs. CA |
0.709 |
0.00% |
1.02 |
0.87,1.19 |
0.814 |
Fixed-effects model |
|
Meta-analysis of BCL-2 promoter polymorphism and cancer prognosis
Overall, our results showed that rs2279115 polymorphism was significantly correlated with the cancer prognosis in all four genetic models (HR=1.09, 95% CI:1.03,1.51, P= 0.000, allelic models respectively). Stratification was performed by ethnicity, rs2279115 was correlated with a significantly higher risk of cancer prognosis in Asia (HR= 1.17, 95% CI:1.01,1.41, P= 0.000, allelic models respectively) but not in Caucasian (HR=1.01, 95%CI:0.90,1.41, P=0.878, allelic models respectively). Simultaneously, there is no correlation between rs1801018 and cancer prognosis (HR=95, 95%CI:0.68,1.36, P=0.547). Table 4 displays the results of analysis.
Table 4: Meta-analysis of BCL-2 promoter polymorphisms and cancer prognosis
Genetic model |
No.of |
PQ |
I2 |
HR |
95% CI |
PZ |
Model |
|---|---|---|---|---|---|---|---|
rs2279115 |
|||||||
Total |
13(4013/5319) |
||||||
CC vs. CA |
0.011 |
59.6% |
1.09 |
1.03,1.51 |
<0.001 |
Random-effects model |
|
CC vs. AA |
0.018 |
58.5% |
1,18 |
1.07,1.66 |
<0.001 |
Random-effects model |
|
CA vs. AA |
0.677 |
0.00% |
1.31 |
1.12,2.61 |
<0.001 |
Fixed-effects model |
|
CC vs. CA+AA |
0.000 |
84.8% |
1.26 |
1.16,1.71 |
<0.001 |
Random-effects model |
|
Asia |
6(2813/3124) |
||||||
CC vs. CA |
0.000 |
55.5% |
1.17 |
1.01,1.41 |
<0.001 |
Random-effects model |
|
CC vs. AA |
0.000 |
38.4% |
1.50 |
1.01,2.15 |
<0.001 |
Fixed-effects model |
|
CA vs. AA |
0.000 |
55.1% |
1.38 |
1.03,1.87 |
<0.001 |
Random-effects model |
|
CC vs. CA+AA |
0.000 |
53.4% |
1.21 |
1.06,1.75 |
<0.001 |
Random-effects model |
|
Caucasian |
7(1200/2195) |
||||||
CC vs. CA |
0.651 |
0.0% |
1.01 |
0.90,1.13 |
0.878 |
Fixed-effects model |
|
CC vs. AA |
0.392 |
5.2% |
1.04 |
0.89,1.21 |
0.937 |
Fixed-effects model |
|
CA vs. AA |
0.299 |
15.2% |
1.07 |
0.92,1.45 |
0.430 |
Fixed-effects model |
|
CC vs. CA+AA |
0.180 |
29.9% |
1.35 |
0.72,2.52 |
0.829 |
Fixed-effects model |
|
rs1801018 |
5(1889/2110) |
||||||
AA vs. AG+GG |
0.088 |
43.6% |
0.95 |
0.68,1.36 |
0.547 |
Fixed-effects model |
|
AG vs. GG |
0.610 |
0.0% |
1.51 |
0.74,2.13 |
0.429 |
Fixed-effects model |
|
Sensitivity analysis
Sensitivity analysis was conducted to assess the stability of the results. The results show rs2279115 in four genetic model were stable in Supplementary Figure 1-4, and rs1801018 in four genetic model were stable in Supplementary Figure 5-8.
Publication bias
Each studies in this meta-analysis were performed to evaluate the publication bias by both Begg’s funnel plot and Egger’s test. P>0.05 was considered no publication bias. The results show no obvious evidence of publication bias was found in allelic, dominant, recessive or additive genetic model in rs2279115 and rs1801018 in Table 5.
Table 5: Publication bias analysis of the meta-analysis
Genetic model |
Test |
t |
95% CI |
P |
|---|---|---|---|---|
rs2279115 |
||||
C vs. A |
Begg’s test |
0.120 |
||
Egger’s test |
-2.73 |
-9.59,-1.21 |
0.107 |
|
CC+ CA vs. AA |
Begg’s test |
0.272 |
||
Egger’s test |
-4.09 |
-0.84,-027 |
0.125 |
|
CC vs. CA+AA |
Begg’s test |
0.472 |
||
Egger’s test |
3.27 |
1.11,5.21 |
0.231 |
|
CC vs. CA |
Begg’s test |
0.791 |
||
Egger’s test |
1.85 |
-0.48,6.99 |
0.403 |
|
rs1801018 |
||||
A vs. G |
Begg’s test |
0.602 |
||
Egger’s test |
-4.82 |
-2.60,1.17 |
0.130 |
|
AA+AG vs. GG |
Begg’s test |
0.117 |
||
Egger’s test |
-9.04 |
-0.09,0.02 |
0.070 |
|
AA vs.AG+GG |
Begg’s test |
0.602 |
||
Egger’s test |
-5.03 |
-3.15,1.36 |
0.125 |
|
AA vs. AG |
Begg’s test |
0.602 |
||
Egger’s test |
-5.22 |
-2.82,1.17 |
0.121 |
|
DISCUSSION
Bcl-2 is an important anti-apoptotic protein that can regulate cell death and is thus classified as an oncogene [48]. There is increasing evidence that Bcl-2 gene polymorphism may be associated with cancer susceptibility and prognosis. Recently,polymorphism in Bcl-2 gene, variant in promoter region rs2279115 and rs1801018, have been reported to be associated with cancer susceptibility and prognosis many times. Whether Bcl-2 promoter polymorphisms are related to cancer susceptibility and prognosis, however, the results are incompatible. This might be the first meta-analysis regarding Bcl-2 promoter polymorphisms in cancer susceptibility and prognosis.
In this study, we found that rs2279115 have a significantly higher risk of cancer susceptibility and prognosis in allelic, dominant, recessive, and additive models. However, rs1801018 had no associated with cancer susceptibility and prognosis in allelic, dominant, recessive, and additive model. Subgroups analysis indicated that rs2279115 was associated with a significantly higher risk of cancer in Asia but not in Caucasian. Furthermore, rs2279115 was associated with a significantly higher risk of cancer in digestive system cancer and endocrine system cancer but not in breast cancer, respiratory cancer and hematopoietic cancer. This is may because lack of large sample size in breast cancer, respiratory cancer and hematopoietic cancer. Therefore, consider the inconsistency of these results, large sample size is needed in rs2279115 polymorphism and cancer susceptibility in different cancer type. Simultaneously,rs2279115 was correlated with a significantly higher risk of cancer prognosis in Asia but not in Caucasian. Considering these promising results, rs2279115 may be a tumor marker for cancer therapy in Asia.
Although, we performed this meta-analysis very carefully, however, some limitations must be considered in the current meta-analysis. First, we performed stratification only by ethnicity and cancer type, without referring other factors. Further research should be conducted in other cancer type and other ethnicity population. Second, we only select literature that written by English, other language should be chosen in the further. Third, in the subgroup analysis in cancer type, there might be insufficient statistical power to check an association.
In conclusion, our meta-analysis suggests a role BCL-2 promoter polymorphisms in cancer susceptibility and prognosis, rs2279115 but not rs1801018 may be a tumor marker for cancer therapy in Asia. However, large sample size, different ethnic population and different cancer type is warranted to validate this association.
MATERIALS AND METHODS
Literature search
We searched PubMed and Embase databases up to August 30, 2016, with keywords including “cancer” and “BCL-2 or B cell lymphoma-2” and “single nucleotide polymorphism or mutation or variation or SNP”. We also manually checked reference lists to identify other potential studies and restricted the search to human studies. The database search was performed independently by Binhui Yang and Zhongqiu Liu and the disagreements were resolved through consensus by all of the authors.
Inclusion and exclusion criteria
If the following inclusion were satisfied, studies would be included in our meta-analysis: 1) case-control studies focused on association between the Bcl-2 promoter polymorphism and cancer susceptibility or prognostic significance. 2) Studies provided sufficient data to estimate the odds ratio (OR) or hazard ratio (HR) and 95% confidence intervals (CI) according to Bcl-2 promoter polymorphisms. 3) When study patients overlapped with patients in other included studies, we selected the first study published. The two researchers (Wei Li and Qihua He) read the titles and abstracts independently and excluded the uncorrelated studies; then the full-texts were examined by our review team and the disagreements were resolved through consensus by all of the authors. The studies would be selected according to the inclusion criteria.
Data extraction
The following information in studies investigating the association between Bcl-2 promoter polymorphisms and susceptibility was extracted by two independent researchers: (1) first author; (2) publication year; (3) mean value of age; (4) country and ethnicity; (5) cancer type; (6) cases and controls sample size; (7)genotype. As for studies investigating the association between Bcl-2 polymorphism and cancer prognostic, two researchers independently extracted the following information from the article:(1) first author; (2) publication year; (3) mean value of age; (4) country and ethnicity; (5) cancer type; (6) cases and controls sample size; (7) genotype; (8) HR estimation. The two researchers (Wei Li and Qihua He) read the reports independently, and the disagreements were resolved through consensus by all of the authors.
Statistical analysis
STATA software 12.0 (STATA Corp, College Station, TX, USA) were used to evaluate the relationships between Bcl-2 promoter polymorphisms and cancer susceptibility and prognosis. Studies were assessed by chi-square in control group under Hardy-Weinberg equilibrium (HWE) to calculate frequencies of BCL-2, and if P< 0.05, study was considered to be disequilibrium. The strength of the relationship between Bcl-2 polymorphisms including rs2279115 and rs1801018 and cancer susceptibility were evaluated by odd ratios (ORs) with corresponding 95% confidence intervals (CIs). The correlation between Bcl-2 polymorphisms and cancer prognosis were measured by hazard ratios (HRs). By using Q test and I2 statistic to assess heterogeneity among studies in rs2279115 in the allelic (C vs. A), dominant (CC+ CA vs. AA), recessive (CC vs. CA+AA), and additive (CC vs. CA) and in rs1801018 in the allelic (A vs. G), dominant (AA+AG vs. GG), recessive (AA vs.AG+GG), and additive (AA vs. AG) genetic models. Random-effect model was chosen if PQ< 0.10 or I2>50%, otherwise, fixed-effect mode was applied. Sensitivity analysis was conducted to assess the stability of the results. Begg’s and Egger’s tests were to assess the publication bias of each study. P< 0.05 was considered signifcant for all tests.
ACKNOWLEDGMENTS
No financial support and sponsorship support this work.
COMPETING FINANCIAL INTERESTS
No conflict of financail interests is stated by authors.
Author contributions
Binhui Yang and Zhongqiu Liu performed search, Wei Li and Qihua He prepared tables and figures, Xingchun Peng and Zhongqiang Yao wrote the manuscript and performed power calculation.
REFERENCES
1. Cory S, Adams JM. The Bcl2 family: regulators of the cellular life-or-death switch. Nat Rev Cancer. 2002; 2: 647-56.
2. Safaeian L, Abed A, Vaseghi G. The role of Bcl-2 family proteins in pulmonary fibrosis. Eur J Pharmacol. 2014; 741: 281-9.
3. Ethell DW, Buhler LA. Fas ligand-mediated apoptosis in degenerative disorders of the brain. J Clin Immunol. 2003; 23: 439-46.
4. Almeida S, Sarmento-Ribeiro AB, Januario C, Rego AC, Oliveira CR. Evidence of apoptosis and mitochondrial abnormalities in peripheral blood cells of Huntington’s disease patients. Biochem Biophys Res Commun. 2008; 374: 599-603.
5. Johnson CH, Bonzo JA, Cheng J, Krausz KW, Kang DW, Luecke H, Idle JR, Gonzalez FJ. Cytochrome P450 regulation by alpha-tocopherol in Pxr-null and PXR-humanized mice. Drug Metab Dispos. 2013; 41: 406-13.
6. Bonnefoy-Berard N, Aouacheria A, Verschelde C, Quemeneur L, Marcais A, Marvel J. Control of proliferation by Bcl-2 family members. Biochim Biophys Acta. 2004; 1644: 159-68.
7. Johnson MI, Robinson MC, Marsh C, Robson CN, Neal DE, Hamdy FC. Expression of Bcl-2, Bax, and p53 in high-grade prostatic intraepithelial neoplasia and localized prostate cancer: relationship with apoptosis and proliferation. Prostate. 1998; 37: 223-9.
8. Anagnostou VK, Lowery FJ, Zolota V, Tzelepi V, Gopinath A, Liceaga C, Panagopoulos N, Frangia K, Tanoue L, Boffa D, Gettinger S, Detterbeck F, Homer RJ, et al. High expression of BCL-2 predicts favorable outcome in non-small cell lung cancer patients with non squamous histology. BMC Cancer. 2010; 10: 186.
9. Sanchez-Beato M, Sanchez-Aguilera A, Piris MA. Cell cycle deregulation in B-cell lymphomas. Blood. 2003; 101: 1220-35.
10. Davis RE, Staudt LM. Molecular diagnosis of lymphoid malignancies by gene expression profiling. Curr Opin Hematol. 2002; 9: 333-8.
11. Tsujimoto Y, Gorham J, Cossman J, Jaffe E, Croce CM. The t(14;18) chromosome translocations involved in B-cell neoplasms result from mistakes in VDJ joining. Science. 1985; 229: 1390-3.
12. Young RL, Korsmeyer SJ. A negative regulatory element in the bcl-2 5’-untranslated region inhibits expression from an upstream promoter. Mol Cell Biol. 1993; 13: 3686-97.
13. Seto M, Jaeger U, Hockett RD, Graninger W, Bennett S, Goldman P, Korsmeyer SJ. Alternative promoters and exons, somatic mutation and deregulation of the Bcl-2-Ig fusion gene in lymphoma. EMBO J. 1988; 7: 123-31.
14. Park BL, Kim LH, Cheong HS, Cho HY, Kim EM, Shin HD, Kim YS, Lee C. Identification of variants in cyclin D1 ( CCND1) and B-Cell CLL/lymphoma 2 ( BCL2). J Hum Genet. 2004; 49: 449-54.
15. Zenz T, Benner A, Duhrsen U, Durig J, Dohner H, Siffert W, Stilgenbauer S, Nuckel H. BCL2-938C>A polymorphism and disease progression in chronic lymphocytic leukemia. Leuk Lymphoma. 2009; 50: 1837-42.
16. Zhang N, Li X, Tao K, Jiang L, Ma T, Yan S, Yuan C, Moran MS, Liang F, Haffty BG, Yang Q. BCL-2 (-938C > A) polymorphism is associated with breast cancer susceptibility. BMC Med Genet. 2011; 12: 48.
17. Wang YX, Zhao L, Wang XY, Liu CM, Yu SG. Role of Caspase 8, Caspase 9 and Bcl-2 polymorphisms in papillary thyroid carcinoma risk in Han Chinese population. Med Oncol. 2012; 29: 2445-51.
18. Hirata H, Hinoda Y, Nakajima K, Kikuno N, Suehiro Y, Tabatabai ZL, Ishii N, Dahiya R. The bcl2 -938CC genotype has poor prognosis and lower survival in renal cancer. J Urol. 2009; 182: 721-7.
19. Hirata H, Hinoda Y, Kikuno N, Suehiro Y, Shahryari V, Ahmad AE, Tabatabai ZL, Igawa M, Dahiya R. Bcl2 -938C/A polymorphism carries increased risk of biochemical recurrence after radical prostatectomy. J Urol. 2009; 181: 1907-12.
20. Mou X, Li T, Wang J, Ali Z, Zhang Y, Chen Z, Deng Y, Li S, Su E, Jia Q, He N, Ni J, Cui D. Genetic Variation of BCL2 (rs2279115), NEIL2 (rs804270), LTA (rs909253), PSCA (rs2294008) and PLCE1 (rs3765524, rs10509670) Genes and Their Correlation to Gastric Cancer Risk Based on Universal Tagged Arrays and Fe3O4 Magnetic Nanoparticles. J Biomed Nanotechnol. 2015; 11: 2057-66.
21. Moazami-Goudarzi M, Farshdousti-Hagh M, Hoseinpour-Feizi A, Talebi M, Movassaghpour-Akbari AA, Shams-Asanjan K, Eyvazi-Ziyaee J, Seifi M. The acute lymphoblastic leukemia prognostic scoring whether it is possible by BCL-2, BAX gene promoter genotyping. Caspian J Intern Med. 2016; 7: 105-13.
22. Bhushann Meka P, Jarjapu S, Vishwakarma SK, Nanchari SR, Cingeetham A, Annamaneni S, Mukta S, Triveni B, Satti V. Influence of BCL2-938 C>A promoter polymorphism and BCL2 gene expression on the progression of breast cancer. Tumour Biol. 2016; 37: 6905-12.
23. Yang X, Gao F, Ma F, Ren Y, Chen H, Liang X, Han S, Xiong X, Pan W, Zhou C, Zhou L, Yang M. Association of the functional BCL-2 rs2279115 genetic variant and small cell lung cancer. Tumour Biol. 2016; 37: 1693-8.
24. Fernandes AT, Rocha NP, Vendrame E, Russomano F, Grinsztejn BJ, Friedman RK, Pinto AC, Klumb EM, Avvad E, Macedo J, Martinez-Maza O, Bonecini-Almeida Mda G. Polymorphism in apoptotic BAX (-248G>A) gene but not in anti-apoptotic BCL2 (-938C>A) gene and its protein and mRNA expression are associated with cervical intraepithelial neoplasia. Apoptosis. 2015; 20: 1347-57.
25. Pan W, Yang J, Wei J, Chen H, Ge Y, Zhang J, Wang Z, Zhou C, Yuan Q, Zhou L, Yang M. Functional BCL-2 regulatory genetic variants contribute to susceptibility of esophageal squamous cell carcinoma. Sci Rep. 2015; 5: 11833.
26. Cingeetham A, Vuree S, Dunna NR, Gorre M, Nanchari SR, Edathara PM, Meka P, Annamaneni S, Digumarthi R, Sinha S, Satti V. Influence of BCL2-938C>A and BAX-248G>A promoter polymorphisms in the development of AML: case-control study from South India. Tumour Biol. 2015; 36: 7967-76.
27. Oliveira C, Lourenco GJ, Rinck-Junior JA, Cintra ML, Moraes AM, Lima CS. Association between genetic polymorphisms in apoptosis-related genes and risk of cutaneous melanoma in women and men. J Dermatol Sci. 2014; 74: 135-41.
28. Li W, Qian C, Wang L, Teng H, Zhang L. Association of BCL2-938C>A genetic polymorphism with glioma risk in Chinese Han population. Tumour Biol. 2014; 35: 2259-64.
29. Wang WL, Tao YP, Han XL, Li X, Zi YM, Yang C, Li JD. Role of polymorphisms in BCL-2 and BAX genes in modulating the risk of developing non-Hodgkin lymphoma. Leuk Lymphoma. 2014; 55: 1602-8.
30. Xu P, Liu L, Wang J, Zhang K, Hong X, Deng Q, Xiang J, Zhang X, He M, Wu T, Guo H. Genetic variation in BCL2 3’-UTR was associated with lung cancer risk and prognosis in male Chinese population. PLoS One. 2013; 8: e72197.
31. Meyer A, Coinac I, Bogdanova N, Dubrowinskaja N, Turmanov N, Haubold S, Schurmann P, Imkamp F, von Klot C, Merseburger AS, Machtens S, Bremer M, Hillemanns P, et al. Apoptosis gene polymorphisms and risk of prostate cancer: a hospital-based study of German patients treated with brachytherapy. Urol Oncol. 2013; 31: 74-81.
32. Searle CJ, Brock IW, Cross SS, Balasubramanian SP, Reed MW, Cox A. A BCL2 promoter polymorphism rs2279115 is not associated with BCL2 protein expression or patient survival in breast cancer patients. Springerplus. 2012; 1: 38.
33. Liu Z, Sun R, Lu W, Dang C, Song Y, Wang C, Zhang X, Han L, Cheng H, Gao W, Liu J, Lei G. The -938A/A genotype of BCL2 gene is associated with esophageal cancer. Med Oncol. 2012; 29: 2677-83.
34. Chen K, Hu Z, Wang LE, Sturgis EM, El-Naggar AK, Zhang W, Wei Q. Single-nucleotide polymorphisms at the TP53-binding or responsive promoter regions of BAX and BCL2 genes and risk of squamous cell carcinoma of the head and neck. Carcinogenesis. 2007; 28: 2008-12.
35. Fingas CD, Katsounas A, Kahraman A, Siffert W, Jochum C, Gerken G, Nuckel H, Canbay A. Prognostic assessment of three single-nucleotide polymorphisms (GNB3 825C>T, BCL2-938C>A, MCL1-386C>G) in extrahepatic cholangiocarcinoma. Cancer Invest. 2010; 28: 472-8.
36. Eun YG, Hong IK, Kim SK, Park HK, Kwon S, Chung DH, Kwon KH. A Polymorphism (rs1801018, Thr7Thr) of BCL2 is Associated with Papillary Thyroid Cancer in Korean Population. Clin Exp Otorhinolaryngol. 2011; 4: 149-54.
37. Lehnerdt GF, Franz P, Bankfalvi A, Grehl S, Kelava A, Nuckel H, Lang S, Schmid KW, Siffert W, Bachmann HS. The regulatory BCL2 promoter polymorphism (-938C>A) is associated with relapse and survival of patients with oropharyngeal squamous cell carcinoma. Ann Oncol. 2009; 20: 1094-9.
38. El Hindy N, Bachmann HS, Lambertz N, Adamzik M, Nuckel H, Worm K, Zhu Y, Sure U, Siffert W, Sandalcioglu IE. Association of the CC genotype of the regulatory BCL2 promoter polymorphism (-938C>A) with better 2-year survival in patients with glioblastoma multiforme. J Neurosurg. 2011; 114: 1631-9.
39. Bachmann HS, Heukamp LC, Schmitz KJ, Hilburn CF, Kahl P, Buettner R, Nuckel H, Eisenhardt A, Rubben H, Schmid KW, Siffert W, Eggert A, Schramm A, et al. Regulatory BCL2 promoter polymorphism (-938C>A) is associated with adverse outcome in patients with prostate carcinoma. Int J Cancer. 2011; 129: 2390-9.
40. Bachmann HS, Otterbach F, Callies R, Nuckel H, Bau M, Schmid KW, Siffert W, Kimmig R. The AA genotype of the regulatory BCL2 promoter polymorphism (938C>A) is associated with a favorable outcome in lymph node negative invasive breast cancer patients. Clin Cancer Res. 2007; 13: 5790-7.
41. Heubner M, Wimberger P, Otterbach F, Kasimir-Bauer S, Siffert W, Kimmig R, Nuckel H. Association of the AA genotype of the BCL2 (-938C>A) promoter polymorphism with better survival in ovarian cancer. Int J Biol Markers. 2009; 24: 223-9.
42. Knoefel LF, Werle-Schneider G, Dally H, Muller PJ, Edler L, Bartsch H, Tuengerthal S, Heussel CP, Reinmuth N, Thomas M, Risch A. Polymorphisms in the apoptotic pathway gene BCL-2 and survival in small cell lung cancer. J Thorac Oncol. 2011; 6: 183-9.
43. Kunkele A, Grosse-Lordemann A, Schramm A, Eggert A, Schulte JH, Bachmann HS. The BCL2-938 C > A promoter polymorphism is associated with risk group classification in children with acute lymphoblastic leukemia. BMC Cancer. 2013; 13: 452.
44. Masago K, Togashi Y, Fujita S, Nagai H, Sakamori Y, Okuda C, Kim YH, Mishima M. Effect of the BCL2 gene polymorphism on survival in advanced-stage non-small cell lung cancer patients who received chemotherapy. Oncology. 2013; 84: 214-8.
45. Moon JH, Sohn SK, Lee MH, Jang JH, Kim K, Jung CW, Kim DH. BCL2 gene polymorphism could predict the treatment outcomes in acute myeloid leukemia patients. Leuk Res. 2010; 34: 166-72.
46. Nuckel H, Frey UH, Bau M, Sellmann L, Stanelle J, Durig J, Jockel KH, Duhrsen U, Siffert W. Association of a novel regulatory polymorphism (-938C>A) in the BCL2 gene promoter with disease progression and survival in chronic lymphocytic leukemia. Blood. 2007; 109: 290-7.
47. Jain M, Kumar S, Lal P, Tiwari A, Ghoshal UC, Mittal B. Role of BCL2 (ala43thr), CCND1 (G870A) and FAS (A-670G) polymorphisms in modulating the risk of developing esophageal cancer. Cancer Detect Prev. 2007; 31: 225-32.
48. Ola MS, Nawaz M, Ahsan H. Role of Bcl-2 family proteins and caspases in the regulation of apoptosis. Mol Cell Biochem. 2011; 351: 41-58.