
INTRODUCTION
Periodontal disease, a multifactorial disease, is mainly composed of chronic periodontitis (CP) and aggressive periodontitis (AgP) [1–3]. Periodontal disease, which is a risk factor of systemic diseases, such as head and neck cancer [4], diabetes [5], cardiovascular disease [6–7], erectile dysfunction [8], preterm birth, and low birthweight [9] has become a major public health problem. Therefore, it is of great significant to detect periodontal disease activity and to predict treatment efficacy genetically. A variety of publications have reported the potential association between interleukin (IL) polymorphisms and periodontal disease. IL-1β (beta) is highly polymorphic, and three polymorphisms that lead to transitions between C and T at positions -31(T→C, rs1143627), -511(C→T, rs16944), and +3954/3953(C→T, rs1143634) base pairs (bp) from the transcriptional site have been widely researched [1, 10–11]. Meta-analyses have proven that IL-1β rs1143634 polymorphism is significantly connected with the increased risk of CP [12–13], especially for white adults [14]; whereas, no significant association was discovered between IL-1β rs16944 polymorphism and CP susceptibility [15]. In addition, IL-1β rs1143634 polymorphism is correlated with CP [12–14] but has nothing to do with AgP [1].
An increasing number of studies have examined the association between IL-1β rs1143627 polymorphism and periodontal disease, but as far as we know, no meta-analyses have been carried out about this issue yet. Therefore, the questions of whether IL-1β rs1143627 polymorphism is related to periodontal disease or not, and whether there is a difference of such relationship between CP and AgP still remain uncertain. As a consequence, we conducted this meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [16] in order to answer those questions.
RESULTS
Study identification and characteristics
The initial search identified 350 publications and 6 eligible publications involving 8 case-control studies [17–22] were finally included. The literature search and selection process are shown in Figure 1.
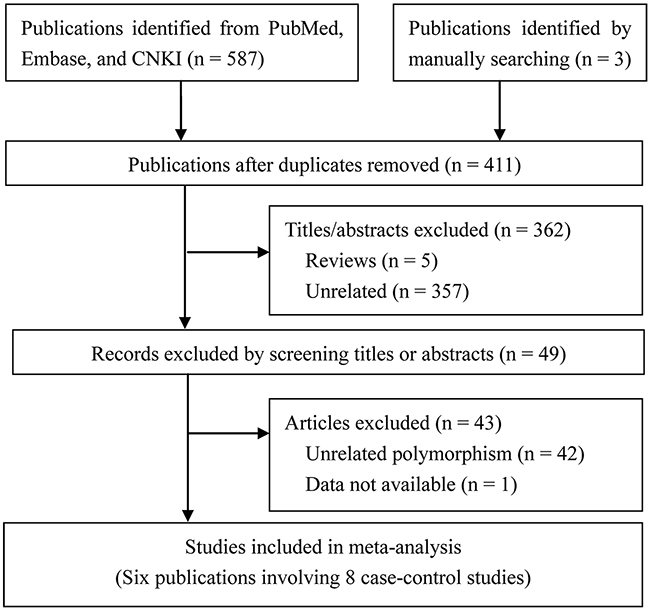
Figure 1: Study selection flow diagram.
The characteristics and relevant data of all included studies are shown in Table 1. All studies were case-control studies, totally containing 229 AgP patients, 382 CP patients, and 555 healthy controls. Two studies included both AgP and CP [19–20], which were treated as 4 independently case-control studies; while 3 case-control studies [17–18, 22] focused on CP patients and only 1 [19] focused on AgP patients. Among these studies, 5 were carried out in Asians, and 2 were performed in Jordanian, while only 1 was conducted in Italians and. All the studies conformed to HWE (p > 0.05).
Table 1: Characteristics of included studies in meta-analysis
Study |
Country (Ethinicity) |
Type |
Case/Control |
Genotyping method |
HWE |
Smoking status |
||||
|---|---|---|---|---|---|---|---|---|---|---|
Sample |
Mean age |
Male:Female |
C allele |
T allele |
||||||
Komatsu 2008 |
Japan (Asian) |
CP |
113/108 |
57.4±0.9/47.4±1.7 |
43:70/47:61 |
107/108 |
119/108 |
NA |
Yes |
None |
Scapoli 2010 |
Italy (unrelated Caucasian Italians) |
AgP |
95/121 |
43.4 ±7.7/30.1 ±4.7 |
29:66/60:61 |
1.002 (0.645-1.558)* |
MassARRAY |
Yes |
NA |
|
Kobayashi 2009 |
Japan (Asian) |
CP |
117/108 |
51.9±0.9/51.2±1.2 |
86:31/75:35 |
120/104 |
114/112 |
TaqMan |
Yes |
Mixed |
Shete 2010 |
India (Asian) |
CP |
43/107 |
35.21/NA |
7:36/NA |
61/147 |
25/67 |
PCR-RFLP |
Yes |
None |
Shete 2010 |
India (Asian) |
AgP |
54/107 |
25.9/NA |
20:34/NA |
76/107 |
32/67 |
PCR-RFLP |
Yes |
None |
Karasneh 2011 |
Jordan (Jordanian) |
CP |
100/80 |
40.43±11.25/22.28±5.43 |
56:44/48:32 |
117/80 |
83/104 |
PCR-RFLP |
Yes |
Mixed |
Karasneh 2011 |
Jordan (Jordanian) |
AgP |
80/80 |
29.15±7.92/22.28±5.43 |
22:58/48:32 |
100/80 |
60/104 |
PCR-RFLP |
Yes |
Mixed |
Amirisetty 2014 |
India (Asian) |
CP |
29/31 |
41.3/41.8 |
23:6/23:8 |
36/31 |
36/22 |
PCR-RFLP |
Yes |
None |
Notes: CP, chronic periodontitis; AgP, aggressive periodontitis; NA, not available; HWE, Hardy-Weinberg equilibrium; None, non-smokers; Mixed, with both ever smokers and non-smokers; *, odds ratio with its 95% confidence interval.
Meta-analysis
Table 2 shows the results of heterogeneity test, subgroup analyses, and overall estimates.
Table 2: Overall and subgroup analyses of meta-analysis
Genetic comparison |
Overall and subgroup analysis |
No. of studies |
Heterogeneity |
Model |
Meta-analysis |
||
|---|---|---|---|---|---|---|---|
p |
I2(%) |
OR(95%CI) |
p |
||||
T vs. C |
Overall |
8 |
0.78 |
0.00 |
Fixed |
0.92(0.81-1.12) |
0.57 |
AgP |
3 |
0.52 |
0.00 |
Fixed |
0.92(0.71-1.20) |
0.55 |
|
CP |
5 |
0.63 |
0.00 |
Fixed |
0.97(0.80-1.19) |
0.79 |
|
Asian |
5 |
0.68 |
0.00 |
Fixed |
0.97(0.80-1.16) |
0.71 |
|
Jordanian |
2 |
0.31 |
3.82 |
Fixed |
0.85(0.59-1.23) |
0.40 |
|
Italian |
1 |
1.00 |
0.00 |
Fixed |
1.11(0.64-1.92) |
0.70 |
|
Mixed |
3 |
0.34 |
8.52 |
Fixed |
0.98(0.76-1.28) |
0.90 |
|
None |
4 |
0.72 |
0.00 |
Fixed |
0.91(0.74-1.13) |
0.42 |
|
TT vs. CC |
Overall |
6 |
0.33 |
13.32 |
Fixed |
1.22(0.80-1.87) |
0.36 |
AgP |
2 |
0.50 |
0.00 |
Fixed |
1.74(0.88-3.45) |
0.11 |
|
CP |
4 |
0.31 |
17.10 |
Fixed |
0.98(0.57-1.68) |
0.93 |
|
Asian |
4 |
0.72 |
0.00 |
Fixed |
0.84(0.48-1.45) |
0.52 |
|
Jordanian |
2 |
0.95 |
0.00 |
Fixed |
2.10(1.09-4.07) |
0.03 |
|
Mixed |
3 |
0.15 |
47.51 |
Fixed |
1.39(0.83-2.31) |
0.21 |
|
None |
3 |
0.55 |
0.00 |
Fixed |
0.92(0.43-1.97) |
0.84 |
|
CT vs. CC |
Overall |
6 |
0.80 |
0.00 |
Fixed |
0.92(0.69-1.23) |
0.58 |
AgP |
2 |
0.33 |
0.00 |
Fixed |
0.74(0.46-1.20) |
0.22 |
|
CP |
4 |
0.98 |
0.00 |
Fixed |
1.05(0.72-1.52) |
0.80 |
|
Asian |
4 |
0.56 |
0.00 |
Fixed |
0.87(0.60-1.28) |
0.49 |
|
Jordanian |
2 |
0.72 |
0.00 |
Fixed |
0.99(0.63-1.55) |
0.96 |
|
Mixed |
3 |
0.93 |
0.00 |
Fixed |
1.00(0.69-1.45) |
1.00 |
|
None |
3 |
0.43 |
0.00 |
Fixed |
0.81(0.50-1.29) |
0.37 |
|
TT vs. (CC+CT) |
Overall |
6 |
0.15 |
38.91 |
Fixed |
1.19(0.81-1.74) |
0.37 |
AgP |
2 |
0.67 |
0.00 |
Fixed |
1.98(1.04-3.80) |
0.04 |
|
CP |
4 |
0.22 |
32.14 |
Fixed |
0.92(0.57-1.46) |
0.71 |
|
Asian |
4 |
0.41 |
0.00 |
Fixed |
0.84(0.52-1.36) |
0.49 |
|
Jordanian |
2 |
0.84 |
0.00 |
Fixed |
2.11(1.14-3.91) |
0.02 |
|
Mixed |
3 |
0.06 |
63.53 |
Random |
1.40(0.66-2.99) |
0.38 |
|
None |
3 |
0.29 |
18.41 |
Fixed |
1.02(0.49-2.10) |
0.96 |
|
(TT+CT) vs. CC |
Overall |
6 |
0.04 |
57.80 |
Random |
0.66(0.44-1.01) |
0.06 |
AgP |
2 |
0.27 |
18.76 |
Fixed |
0.45(0.30-0.68) |
<0.01 |
|
CP |
4 |
0.16 |
41.19 |
Fixed |
0.86(0.60-1.22) |
0.39 |
|
Asian |
4 |
0.09 |
54.35 |
Random |
0.59(0.34-1.01) |
0.05 |
|
Jordanian |
2 |
0.05 |
72.43 |
Random |
0.82(0.37-1.81) |
0.62 |
|
Mixed |
3 |
0.14 |
49.45 |
Fixed |
0.83(0.59-1.18) |
0.30 |
|
None |
3 |
0.21 |
35.43 |
Fixed |
0.45(0.29-0.69) |
<0.01 |
|
Notes: AgP, aggressive periodontitis; CP, chronic periodontitis; OR, odds ratio; CI, confidence interval; Mixed, with both non-smokers and ever smokers; None, non-smokers.
In total analysis, non-significant correlation was observed between IL-1β rs1143627 polymorphism and periodontal disease susceptibility under all 5 genetic models [T vs. C: odds ratio (OR) = 0.92, 95% confidence interval (CI) = 0.81-1.12, I2= 0% (Figure 2); TT vs. CC: OR = 1.22, 95% CI = 0.80-1.87, I2= 13.32%; CT vs. CC: OR = 0.92, 95% CI = 0.69-1.23, I2= 0%; CT+TT vs. CC: OR = 0.66, 95% CI = 0.44-1.01, I2= 57.8%; TT vs. CT + CC: OR = 1.19, 95% CI = 0.81-1.74, I2= 38.91%]. Sensitivity analyses of each genetic model all revealed robust results (Figure 3).
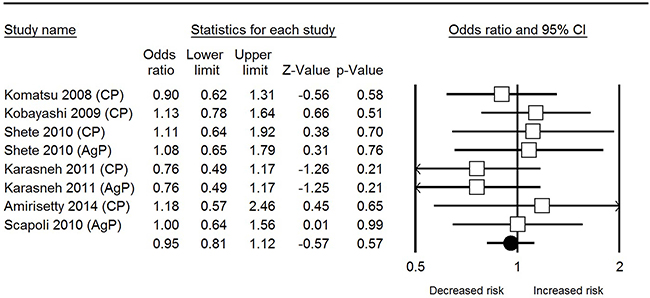
Figure 2: Forest plot of IL-1β rs1143627 polymorphism and periodontal disease in allele comparison.
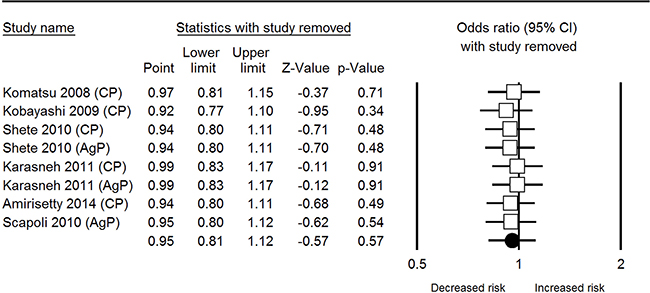
Figure 3: Sensitivity analysis plot of IL-1β rs1143627 polymorphism and periodontal disease in allele comparison.
Subgroup analysis based on smoking status also revealed non-significant association. However, after stratified analysis by ethnicity, TT vs. CC (OR = 2.10, 95%CI = 1.09-4.07) and TT vs. CT + CC (OR = 2.11, 95%CI = 1.14-3.91) stated that IL-1β rs1143627 polymorphism was associated with the increased risk of PD in Jordanian population; meanwhile, in stratified analysis by periodontal disease type, the TT vs. CT + CC (OR = 1.98, 95%CI = 1.04-3.80) showed that IL-1β rs1143627 polymorphism was connected with the increased risk of AgP while the CT+TT vs. CC (OR = 0.45, 95%CI = 0.30-0.68) revealed a decreased risk of AgP.
Publication bias
There was no obvious asymmetry in the funnel plot through visual inspection (Figure 4). The Egger’s test of all 5 genetic models also showed no evidence of significant publication bias (T vs. C: p = 0.46; TT vs. CC: p = 0.44; CT vs. CC: p = 0.76; (TT+CT) vs. CC: p = 0.70; TT vs. (CT + CC): p = 0.81).
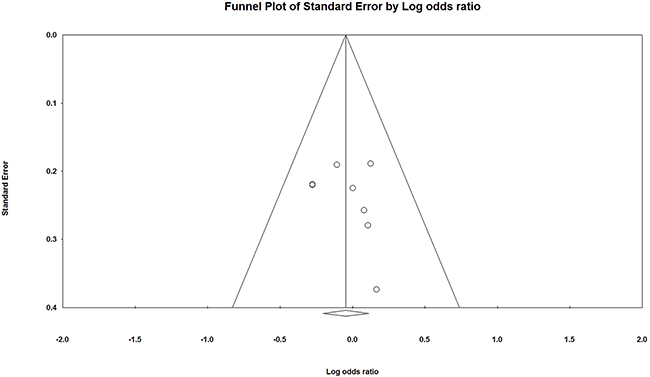
Figure 4: Funnel plot of IL-1β rs1143627 polymorphism and periodontal disease in allele comparison.
DISCUSSION
Our meta-analysis, based on 8 eligible case-control studies, demonstrated that there was no obvious association of IL-1β rs1143627 polymorphism with periodontal disease susceptibility in total analysis. The sensitivity analyses supported that the overall analyses were robust, and the majority of subgroup analyses concluded similar results in the overall populations. Smoking, which is a classical risk factor of periodontal disease [23] influences the prognosis of periodontal disease [24]. Hence, we performed a subgroup analysis according to the smoking status of participants. The results showed non-significant relation of periodontal disease risk with either non-smokers or mixed smokers (including ever smokers and non-smokers). Due to the lack of sufficient data, we could not detect whether IL-1β rs1143627 polymorphism is a co-factor of smoking in periodontal disease. Further studies should divide the populations into smokers and non-smokers, or only contain smokers to provide evidences for the collective effect of smoking with this polymorphism.
The current study was the first meta-analysis designed to investigate the correlation of IL-1β rs1143627 polymorphism with the risk of periodontal disease, and revealed a negative result, showing the lack of significant association. The results could be explained by some clues from published meta-analyses. First, the different polymorphisms in the same IL gene could show different results. For example, in 2009, Shao et al [25] conducted a systematic review and meta-analysis which indicated that only IL-6 C572G polymorphism was associated with periodontitis. Then a meta-analysis by Zhong et al [26] in 2012 illustrated that IL-10 C-819T and C-592A polymorphisms were in connection with CP while A-1082G polymorphism was not. Second, the association of the same gene polymorphism may be different in CP and AgP. For example, IL-1α C-899 (+4845)T polymorphism was related to the increased risk of CP [27] but not associated with AgP [28]. Since there were few studies included in our analysis, the current results should be treated with caution because the results may change along with alterations in studies populations, disease type or other relevant factors.
The major limitations of our meta-analysis were the small sample size and limited number of included studies. The results also changed as sample size increased. In 2008, Nikolopoulos et al [13] conducted a meta-analysis based on 10 case-control studies which informed no association of IL-1β rs1143634 polymorphism with CP in Caucasian populations. Yet, the later meta-analysis based on 16 studies by Deng et al [12] in 2013 put forward that IL-1β rs1143634 polymorphism was associated with increased risk of CP in Caucasian populations. In consequence, further studies are necessary to verify which conclusion is accurate. Moreover, we only enrolled studies published in English or Chinese language, suggesting that the publications in other languages were neglected. Furthermore, although the heterogeneity apart from contrast TT+CT vs. CC was acceptable in 4 genetic models, we still could not ignore the potential influences of heterogeneity. We failed to find an explanation for the heterogeneity of model TT+CT vs. CC being the largest. Meta-analysis was a secondary and observational study [29–30], thus it was limited by the quality of primary studies. Although we had conducted a more comprehensive search, the complete elimination of limitation still could not be guaranteed. The effects of gene - gene or gene - environment interactions were not analyzed owing to the lack of original data. In other words, our results were based on unadjusted data and these limitations might influence our final conclusions.
In summary, our meta-analysis suggests that IL-1β rs1143627 polymorphism is not associated with periodontal disease on the basis of current available evidence. However, we suggest that the results should be examined in further better-designed researches with larger sample size and multiple ethnic groups considering the above mentioned limitations, in order to measure the relationship of IL-1β rs1143627 polymorphism with periodontal disease development more comprehensively and precisely.
MATERIALS AND METHODS
Eligible criteria
Studies would be included if they met all the following criteria: (1) patients were clearly diagnosed with periodontal disease (either CP, AgP, or both) and the controls were periodontally healthy people without periodontitis; (2) studies explored the association between IL-1β rs1143627 polymorphism and periodontal disease susceptibility using a case-control or cohort study design; (3) full data on OR and 95% CI were reported in each group, or sufficient data were provided to calculate them; and (4) if two or more publications were from the same institute, we would compared their detailed basic information and then chose the more comprehensive one.
Search strategy
Two authors independently searched multiple online electronic databases known as PubMed, Embase, and Chinese National Knowledge Infrastructure (CNKI) up to October 26, 2016. The following key words were used in search strategy: “IL-1” or “interleukin-1”, “periodontal diseases” or “periodontitis”, and “polymorphism” or “mutation” or “variant” or “haplotype”. Moreover, all listed references of eligible studies and recently reviews were also screened for purpose of identifying the additional relevant publications. Only the studies published in Chinese or English were selected.
Data extraction
Two authors independently collected and recorded the main information from each included case-control studies. Any discrepancies were resolved through discussion to come to a consensus. The extracted data were listed as follows: surname of the first author, year of publication, study design, country and ethnicity of included population, demographics, smoking status, number of cases and controls, genotype distributions, source of controls, genotyping method, and Hardy-Weinberg equilibrium (HWE) for controls. If HWE was not reported, we calculated the data according to genotype distributions of controls.
Data analysis
Pooled OR and 95% CI were employed to estimate the association of IL-1β rs1143627 polymorphism with periodontal disease risk was evaluated under the allele comparison (T vs. C), homozygote comparison (TT vs. CC), heterozygote comparison (CT vs. CC), dominant model (TT+CT vs. CC), and recessive model (TT vs. CT + CC) [14–15, 31–35]. The between-study heterogeneity was assessed using the Cochrane Collaboration’s Q statistic and I2 statistic [16, 36]. The fixed-effect model was applied while p > 0.1 in Q statistic and I2 < 50% in I2 statistic which suggested an acceptable heterogeneity; otherwise, the random-effects model was used. The sensitivity analysis was also performed by omitting each included study in turn for investigating the robustness of overall results [15, 31]. Besides, we carry out subgroup analyses to further evaluate the specific correlation between periodontal disease risk and IL-1β rs1143627 variant according to ethnicity, HWE status, periodontal disease type, and smoking status if it was appropriate. Publication bias was assessed with the method of funnel plot and Egger’s test [37]. All the statistical analyses were carried out using the Comprehensive Meta-Analysis v2 software [15, 31, 38].
ACKNOWLEDGMENTS
The authors thank the local doctors and the patients who participated in our study.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
GRANT SUPPORT
None.
REFERENCES
1. Chen YJ, Han Y, Mao M, Tan YQ, Leng WD, Zeng XT. Interleukin-1β rs1143634 polymorphism and aggressive periodontitis susceptibility: a meta-analysis. Int J Clin Exp Med. 2015; 8: 2308-16.
2. Kebschull M, Guarnieri P, Demmer RT, Boulesteix AL, Pavlidis P, Papapanou PN. Molecular Differences between Chronic and Aggressive Periodontitis. J Dent Res. 2013; 92: 1081-8. doi: 10.1177/0022034513506011.
3. Wei XM, Chen YJ, Wu L, Cui LJ, Hu DW, Zeng XT. Tumor necrosis factor-alpha G-308A (rs1800629) polymorphism and aggressive periodontitis susceptibility: a meta-analysis of 16 case-control studies. Sci Rep. 2016; 6: 19099. doi: 10.1038/srep19099.
4. Zeng XT, Deng AP, Li C, Xia LY, Niu YM, Leng WD. Periodontal disease and risk of head and neck cancer: a meta-analysis of observational studies. PLoS One. 2013; 8: e79017. doi: 10.1371/journal.pone.0079017.
5. Mealey BL, Rose LF. Diabetes mellitus and inflammatory periodontal diseases. Compend Contin Educ Dent. 2008; 29: 402-8, 10, 12-3.
6. Leng WD, Zeng XT, Kwong JS, Hua XP. Periodontal disease and risk of coronary heart disease: An updated meta-analysis of prospective cohort studies. Int J Cardiol. 2015; 201: 469-72. doi: S0167-5273(15)30209-6.
7. Zeng XT, Leng WD, Lam YY, Yan BP, Wei XM, Weng H, Kwong JS. Periodontal disease and carotid atherosclerosis: A meta-analysis of 17,330 participants. Int J Cardiol. 2016; 203: 1044-51. doi: 10.1016/j.ijcard.2015.11.092.
8. Keller JJ, Chung SD, Lin HC. A nationwide population-based study on the association between chronic periodontitis and erectile dysfunction. J Clin Periodontol. 2012; 39: 507-12. doi: 10.1111/j.1600-051X.2012.01879.x.
9. Konopka T, Paradowska-Stolarz A. Periodontitis and risk of preterm birth and low birthweight--a meta-analysis. Ginekol Pol. 2012; 83: 446-53.
10. Bird S, Zou J, Wang T, Munday B, Cunningham C, Secombes CJ. Evolution of interleukin-1beta. Cytokine Growth Factor Rev. 2002; 13: 483-502. doi: S135961010200028X.
11. Xu J, Yin Z, Cao S, Gao W, Liu L, Yin Y, Liu P, Shu Y. Systematic review and meta-analysis on the association between IL-1B polymorphisms and cancer risk. PLoS One. 2013; 8: e63654. doi: 10.1371/journal.pone.0063654.
12. Deng JS, Qin P, Li XX, Du YH. Association between interleukin-1beta C (3953/4)T polymorphism and chronic periodontitis: evidence from a meta-analysis. Hum Immunol. 2013; 74: 371-8. doi: 10.1016/j.humimm.2012.11.018.
13. Nikolopoulos GK, Dimou NL, Hamodrakas SJ, Bagos PG. Cytokine gene polymorphisms in periodontal disease: a meta-analysis of 53 studies including 4178 cases and 4590 controls. J Clin Periodontol. 2008; 35: 754-67. doi: 10.1111/j.1600-051X.2008.01298.x.
14. Karimbux NY, Saraiya VM, Elangovan S, Allareddy V, Kinnunen T, Kornman KS, Duff GW. Interleukin-1 gene polymorphisms and chronic periodontitis in adult whites: a systematic review and meta-analysis. J Periodontol. 2012; 83: 1407-19. doi: 10.1902/jop.2012.110655.
15. Zeng XT, Liu DY, Kwong JS, Leng WD, Xia LY, Mao M. Meta-Analysis of Association Between Interleukin-1beta C-511T Polymorphism and Chronic Periodontitis Susceptibility. J Periodontol. 2015; 86: 812-9. doi: 10.1902/jop.2015.140698.
16. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009; 339: b2535. doi: 10.1136/bmj.b2535.
17. Komatsu Y, Galicia JC, Kobayashi T, Yamazaki K, Yoshie H. Association of interleukin-1 receptor antagonist +2018 gene polymorphism with Japanese chronic periodontitis patients using a novel genotyping method. Int J Immunogenet. 2008; 35: 165-70. doi: 10.1111/j.1744-313X.2008.00757.x.
18. Kobayashi T, Murasawa A, Ito S, Yamamoto K, Komatsu Y, Abe A, Sumida T, Yoshie H. Cytokine gene polymorphisms associated with rheumatoid arthritis and periodontitis in Japanese adults. J Periodontol. 2009; 80: 792-9. doi: 10.1902/jop.2009.080573.
19. Scapoli C, Borzani I, Guarnelli ME, Mamolini E, Annunziata M, Guida L, Trombelli L. IL-1 gene cluster is not linked to aggressive periodontitis. J Dent Res. 2010; 89: 457-61. doi: 10.1177/0022034510363232.
20. Shete AR, Joseph R, Vijayan NN, Srinivas L, Banerjee M. Association of single nucleotide gene polymorphism at interleukin-1beta +3954, -511, and -31 in chronic periodontitis and aggressive periodontitis in Dravidian ethnicity. J Periodontol. 2010; 81: 62-9. doi: 10.1902/jop.2009.090256.
21. Karasneh JA, Ababneh KT, Taha AH, Al-Abbadi MS, Ollier WE. Investigation of the interleukin-1 gene cluster polymorphisms in Jordanian patients with chronic and aggressive periodontitis. Arch Oral Biol. 2011; 56: 269-76. doi: 10.1016/j.archoralbio.2010.10.001.
22. Amirisetty R, Patel RP, Das S, Saraf J, Jyothy A, Munshi A. Interleukin 1beta (+3954, -511 and -31) polymorphism in chronic periodontitis patients from North India. Acta Odontol Scand. 2014: 1-5. doi: 10.3109/00016357.2014.961958.
23. Gelskey SC. Cigarette smoking and periodontitis: methodology to assess the strength of evidence in support of a causal association. Community Dent Oral Epidemiol. 1999; 27: 16-24.
24. Kotsakis GA, Javed F, Hinrichs JE, Karoussis IK, Romanos GE. Impact of cigarette smoking on clinical outcomes of periodontal flap surgical procedures: a systematic review and meta-analysis. J Periodontol. 2015; 86: 254-63. doi: 10.1902/jop.2014.140452.
25. Shao MY, Huang P, Cheng R, Hu T. Interleukin-6 polymorphisms modify the risk of periodontitis: a systematic review and meta-analysis. J Zhejiang Univ Sci B. 2009; 10: 920-7. doi: 10.1631/jzus.B0920279.
26. Zhong Q, Ding C, Wang M, Sun Y, Xu Y. Interleukin-10 gene polymorphisms and chronic/aggressive periodontitis susceptibility: a meta-analysis based on 14 case-control studies. Cytokine. 2012; 60: 47-54. doi: 10.1016/j.cyto.2012.05.014.
27. Mao M, Zeng XT, Ma T, He W, Zhang C, Zhou J. Interleukin-1alpha -899 (+4845) C-->T polymorphism increases the risk of chronic periodontitis: evidence from a meta-analysis of 23 case-control studies. Gene. 2013; 532: 114-9. doi: 10.1016/j.gene.2013.09.043.
28. Wang WF, Shi J, Chen SJ, Niu YM, Zeng XT. Interleukin-1alpha -899 (+4845) C-->T polymorphism is not associated with aggressive periodontitis susceptibility: A meta-analysis based on 19 case-control studies. Biomed Rep. 2014; 2: 378-83. doi: 10.3892/br.2014.240.
29. Zeng X, Zhang Y, Kwong JS, Zhang C, Li S, Sun F, Niu Y, Du L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. J Evid Based Med. 2015; 8: 2-10. doi: 10.1111/jebm.12141.
30. Zeng XT, Leng WD, Zhang C, Liu J, Cao SY, Huang W. Meta-analysis on the association between toothbrushing and head and neck cancer. Oral Oncol. 2015; 51: 446-51. doi: 10.1016/j.oraloncology.2015.02.095.
31. Yan Y, Weng H, Shen ZH, Wu L, Zeng XT. Association between interleukin-4 gene -590 c/t, -33 c/t, and 70-base-pair polymorphisms and periodontitis susceptibility: a meta-analysis. J Periodontol. 2014; 85: e354-62. doi: 10.1902/jop.2014.140317.
32. Jiang L, Weng H, Chen MY, Zhang C, Zeng XT. Association between cyclooxygenase-2 gene polymorphisms and risk of periodontitis: a meta-analysis involving 5653 individuals. Mol Biol Rep. 2014; 41: 4795-801. doi: 10.1007/s11033-014-3350-z.
33. Zeng XT, Luo W, Geng PL, Guo Y, Niu YM, Leng WD. Association between the TP53 codon 72 polymorphism and risk of oral squamous cell carcinoma in Asians: a meta-analysis. BMC Cancer. 2014; 14: 469. doi: 10.1186/1471-2407-14-469.
34. Ding C, Chen X, Zhang PT, Huang JP, Xu Y, Chen N, Zhong LJ. Matrix Metalloproteinase-3 -1171 5A/6A Polymorphism (rs35068180) is Associated with Risk of Periodontitis. Sci Rep. 2015; 5: 11667. doi: 10.1038/srep11667.
35. Weng H, Yan Y, Jin YH, Meng XY, Mo YY, Zeng XT. Matrix metalloproteinase gene polymorphisms and periodontitis susceptibility: a meta-analysis involving 6,162 individuals. Sci Rep. 2016; 6: 24812. doi: srep24812.
36. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327: 557-60. doi: 10.1136/bmj.327.7414.557.
37. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315: 629-34.
38. Zeng XT, Luo W, Huang W, Wang Q, Guo Y, Leng WD. Tooth loss and head and neck cancer: a meta-analysis of observational studies. PLoS One. 2013; 8: e79074. doi: 10.1371/journal.pone.0079074.