
Introduction
Lung cancer is one of the most common malignancies and the most frequent cause of cancer-related mortality worldwide [1]. Despite the significant improvement in chemotherapy regimen for the treatment of advanced non-small-cell lung cancer (NSCLC), the 5-year survival for these patients remains relative poor [2, 3]. Thus, novel agents are urgently needed to improve the prognosis of these patients.
The epidermal growth factor receptor (EGFR) is a member of the HER family of receptor tyrosine kinases which plays a critical role in regulating the development and progression of many solid tumors including NSCLC [4-6]. Thus, EGFR and its related signal pathway have been regarded as attractive therapeutic targets in the treatment of NSCLC [7, 8]. Currently, three anti-EGFR agents, gefitinib, erlotinib and afatinib have been approved for use in EGFR mutation-positive NSCLC patients [9, 10]. Although EGFR-TKIs are generally well tolerated, a pattern of adverse events such as skin rash, diarrhea, thromboembolic events and interstitial lung disease have been reported [11-15], which is different from traditional cytotoxic agents. Infections have been reported with anti-EGFR agents. In 2014, Qi et al. performed a meta-analysis and found a significantly increased risk of severe infectious events associated with the use of anti-EGFR mono-clonal antibodies cetuximab and panitumumab in cancer patients (RR 1.34, p = 0.003) [16] . However, whether EGFR-TKIs increase the risk of infections in NSCLC remains unknown. We thus perform this meta-analysis and systematic review of available randomized controlled trials to determine the overall incidence and risk of infections in NSCLC patients treated with these drugs.
Results
Search results
We identified a total of 362 related studies through the database search, and retrieved 52 full-text studies for evaluation. The reasons for study exclusion were illustrated in Figure 1. As a result, 25 RCTs with 13,436 patients were included for the present study [17-41]. The baseline characteristics of each trial were presented in Table 1. For the indications of the included studies, there were eight trials in first-line settings, two trials in adjuvant settings, and fifteen trials in the subsequent lines of treatment (maintenance or second line, Table 1). An open assessment of the included trials was carried out by using Jadad scale, and fourteen trials were placebo-controlled, double-blinded randomized trials with Jadad score of 5, and eleven trials had Jadad scores of 3.
Table 1: baseline characteristics of 25 trials Included in the Meta-analysis (n=17,420)
Studies |
Treatment strategy |
Enrolled patients (n) |
Treatment arms |
Median age (years) |
Median EGFR-TKIs duration (months) |
Median PFS/TTP (months) |
Median OS (months) |
Patients for analysis |
Severe infections |
Reported infectious events |
Herbst R.S. et al 2004 (INTACT-2) |
First-line |
1037 |
Gefitinib 500mg/d plus PC |
62 |
99 days |
4.6 |
8.7 |
342 |
NR |
Pneumonia, sepsis |
Gefitinib 250mg/d plus PC |
61 |
129 days |
5.3 |
9.8 |
342 |
NR |
||||
Placebo plus PC |
63 |
138 days |
5.0 |
9.9 |
341 |
NR |
||||
Giaccone G. et al 2004 (INTACT-1) |
First-line |
1093 |
Gefitinib 500mg/d plus GD |
61 |
97d |
5.5 |
9.9 |
358 |
NR |
Pneumonia |
Gefitinib 250mg/d plus GD |
59 |
150d |
5.8 |
9.9 |
362 |
NR |
||||
Placebo plus GD |
61 |
159d |
6.0 |
10.9 |
355 |
NR |
||||
Herbst R.S. et al 2005 (TRIBUTE) |
First-line |
1059 |
Erlotinib 150mg/d plus PC |
62.7 |
4.6m |
5.1 |
10.6 |
526 |
15 |
Febrile neutropenia, Pneumonias, sepsis, septic shock |
Placebo plus PC |
62.6 |
5.3m |
4.9 |
10.5 |
533 |
7 |
||||
Shepherd F.A. et al 2005 |
Salvage treatment |
731 |
Erlotinib 150mg/d |
62 |
NR |
2.2 |
6.7 |
485 |
2 |
Infection, pneumonitis |
Placebo |
59 |
NR |
1.8 |
4.7 |
242 |
5 |
||||
Thatcher N. et al 2007 |
Salvage treatment |
1692 |
Gefitinib 250mg plus BSC |
62 |
2.9 |
3.0 |
5.6 |
1126 |
30 |
Pneumonia |
Placebo 250mg plus BSC |
61 |
2.7 |
2.6 |
5.1 |
562 |
15 |
||||
Galzemeier U. et al 2007 |
First-line |
1172 |
Erlotinib 150mg/d plus GD |
60.0 |
NR |
23.7 weeks |
43 weeks |
579 |
NR |
Neutropenia/febrile neutropenia/neutropenic sepsis |
Placebo plus GD |
59.1 |
NR |
24.6 weeks |
44.1 weeks |
580 |
NR |
||||
Kelly K. et al 2008 (SWOG S0023) |
Maintenance |
243 |
Gefitinib 250mg/d |
62 |
NR |
8.3 |
23 |
118 |
3 |
Pneumonitis |
Placebo |
61 |
NR |
11.7 |
35 |
125 |
0 |
||||
Kim E.S. et al 2008 (INTEREST) |
Second-line |
1433 |
Gefitinib 250mg/d |
61 |
4.4 |
2.2 |
7.6 |
729 |
23 |
Lung infections |
Docetaxel |
60 |
3.0 |
2.7 |
8.0 |
715 |
25 |
||||
Cappuzzo F.et al/2010 (SATURN:BO18192) |
Maintenance |
1949 |
Erlotinib 150mg qd po |
60 |
NR |
12.3weeks |
12 |
433 |
4 |
Infections |
Placebo |
60 |
NR |
11.1weeks |
11 |
445 |
0 |
||||
Lee D.H. et al 2010 (ISTANA) |
Second-line |
161 |
Gefitinib 250 mg/d |
57 |
NR |
3.3 |
NR |
81 |
NR |
Pneumonia, septic shock |
Docetaxel |
58 |
NR |
3.4 |
NR |
76 |
NR |
||||
Maemondo M. et al 2010 |
First-line |
230 |
Gefitinib 250mg/d |
63.9 |
308 days |
10.8 |
30.5 |
114 |
3 |
Pneumonia |
PC |
62.6 |
84 days |
5.4 |
23.6 |
114 |
0 |
||||
Gaafar R.M. et al/2011 (EORTC 08021) |
Maintenance |
173 |
Gefitinib 250mg/d |
61 |
115d |
4.1 |
10.9 |
85 |
1 |
Infections |
Placebo |
62 |
85d |
2.3 |
9.4 |
86 |
1 |
||||
Natale R.B. et al 2011 |
Second-line |
1240 |
Erlotinib 150 mg/d |
61 |
8.6 weeks |
2.0 |
7.8 |
614 |
NR |
Pneumonia, respiratory tract infection |
Vandetanib 300mg/d |
61 |
9.1 weeks |
2.6 |
6.9 |
623 |
NR |
||||
Zhou C. et al 2011 (OPTIMAL) |
First-line |
165 |
Erlotinib 150mg/d |
57 |
55.5 weeks |
13.1 |
NR |
83 |
1 |
Infection |
Gemcitabine plus carboplatin |
59 |
10.4 weeks |
4.6 |
NR |
72 |
0 |
||||
Ciuleanu T. et al 2012 (TITAN) |
Second-line |
424 |
Erlotinib 150mg/d |
59 |
NR |
6.3 weeks |
5.3 |
196 |
1 |
Infections |
Chemotherapy |
59 |
NR |
8.6 weeks |
5.5 |
213 |
1 |
||||
Lee S.M. et al 2012 (TOPICAL) |
First-line |
670 |
Erlotinib 150mg/d |
77 |
NR |
2.8 |
3.7 |
334 |
5 |
Pneumonia |
Placebo |
77 |
NR |
2.6 |
3.6 |
313 |
1 |
||||
Perol M. et al. 2012 |
Maintenance therapy |
464 |
Observation |
59.8 |
10.9 weeks |
1.9 |
10.8 |
155 |
0 |
Infections |
Gemcitabine |
57.9 |
12 weeks |
3.8 |
15.2 |
154 |
2 |
||||
Erlotinib 150mg/d |
56.4 |
12.1 weeks |
2.9 |
11.4 |
155 |
4 |
||||
Rosell R. et al 2012 (EURTAC) |
First-line |
174 |
Erlotinib 150mg/d |
65 |
8.2 |
9.7 |
19.3 |
84 |
1 |
Pneumonitis |
Chemotherapy |
65 |
2.8 |
5.2 |
19.5 |
82 |
1 |
||||
Sun J.M. et al 2012 (KCSG-LU08-01) |
Second-line |
Gefitinib 250mg/d |
58 |
NR |
9.0 |
22.2 |
68 |
1 |
Infections |
|
Pemetrexed |
64 |
NR |
3.0 |
18.9 |
67 |
2 |
||||
Goss G.D. et al/2013 (NCIC CTG BR 19) |
Adjuvant |
503 |
Gefitinib 150mg/d |
66 |
NR |
4.2y |
5.1y |
251 |
7 |
Infection, pneumonitis |
Placebo |
67 |
NR |
NR |
NR |
252 |
3 |
||||
Johson B.E. et al 2013 (ATLAS) |
Maintenance |
1145 |
Erlotinib 150mg/d+ bevacizumab |
64 |
72d |
4.76 |
14.39 |
368 |
17 |
Infection |
Placebo +bevacizumab |
64 |
64d |
3.71 |
13.31 |
367 |
18 |
||||
Kawaguchi T. et al 2014 (DELTA) |
Second-line |
301 |
Erlotinib |
68 |
NR |
2.0 |
14.8 |
150 |
2 |
Pneumonitis |
Docetaxel |
67 |
NR |
3.2 |
12.2 |
150 |
3 |
||||
Li N. et al 2014 |
Second-line |
123 |
Erlotinib 150mg/d |
54.3 |
NR |
4.1 |
11.7 |
61 |
0 |
Infection |
Pemetrexed |
55.1 |
NR |
3.9 |
13.4 |
62 |
0 |
||||
Kelly. K. et al 2015 (RADIANT) |
Adjuvant |
973 |
Erlotinib 150mg/d |
62 |
NR |
46.4 |
NR |
611 |
8 |
Pneumonia |
Placebo |
61 |
NR |
28.5 |
NR |
343 |
2 |
||||
Soria J.C. et al 2015 (IMPRESS) |
Second-line |
265 |
Gefitinib 150mg/d+ Pemetrexed +cisplatin |
60 |
152.5d |
5.4 |
14.8 |
133 |
NR |
Pneumonia |
Placebo+ Pemetrexed +cisplatin |
58 |
161.5d |
5.4 |
17.2 |
132 |
NR |
Abbreviation: TXT, docetaxel; NA, not reported; PC, paclitaxel plus carboplatin; GP, gemcitabine plus cisplatin; BSC, best support care; GD, gemcitabine plus cisplatin; NR, not reported;
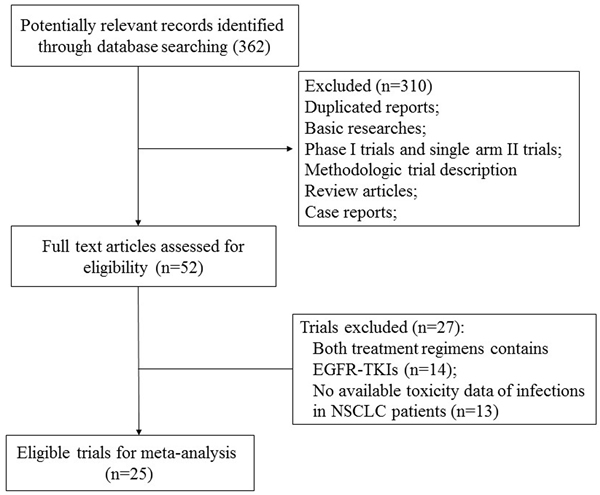
Figure 1: Studies eligible for inclusion in the meta-analysis
Overall incidence of infections
For the all-grade infectious incidence, a total of 6,593 patients were included for analysis. The pooled incidence was 7.0% (95%CI: 4.7-10.3%). For high-grade infections, a total of 5,977 patients were included for analysis yielding a pooled incidence 2.1% (95%CI: 1.7-2.8%). Additionally, 4,077 patients were included for fatal infections analysis. There was a total of 18 fatal infections reported yielding a pooled incidence of 0.7% (95%CI: 0.4% to 1.0%).
Peto Odds ratio of infections
In order to determine the specific contribution of EGFR-TKIs to the development of infections, a meta-analysis of the Peto OR of infections was performed. Our results showed that the Peto OR of all-grade infections was 1.48 (95%CI: 1.12-1.96, p = 0.006, Figure 2A), while the Peto OR of high-grade infections was 1.26 (95%CI: 0.96-1.67, p = 0.098, Figure 2B). Thus, the use of EGFR-TKIs in NSCLC patients had an increased risk of all-grade infections, but not for high-grade infections. Severe infections could be potentially life-threatening adverse events. There were 18 fatal infections events occurred in the EGFR-TKIs and 21 fatal infections events occurred in control arms, yielding a Peto OR 0.81 (95%CI: 0.43-1.53, p = 0.52, Figure 2C). No significant heterogeneity was found during the Peto OR analysis (Q = 6.64; P = 0.88; I2 = 0%). In addition, we conducted sub-group analysis based on treatment regimens, and demonstrated that the addition of EGFR-TKIs to chemotherapy had a tendency to increase the risk of infections in comparison with chemotherapy alone (Peto OR 1.24, 95%CI: 0.75-3.05, p = 0.39). Similarly, the use of EGFR-TKIs alone had a tendency to increase the risk of all-grade infections when compared to placebo (Peto OR 2.24, 95%CI: 0.27-18.53, p = 0.45) or chemotherapy alone (Peto OR 1.93, 95%CI: 0.88-4.26, p = 0.10). Finally, we carried out a meta-regression analysis to investigate the association between Peto OR of all-grade infections and the length of EGFR-TKIs treatment. The results showed that the longer EGFR-TKIs treatment, and the higher risk of infections with EGFR-TKIs, but this relationship was not statistically significant (P = 0.26, Figure 3).
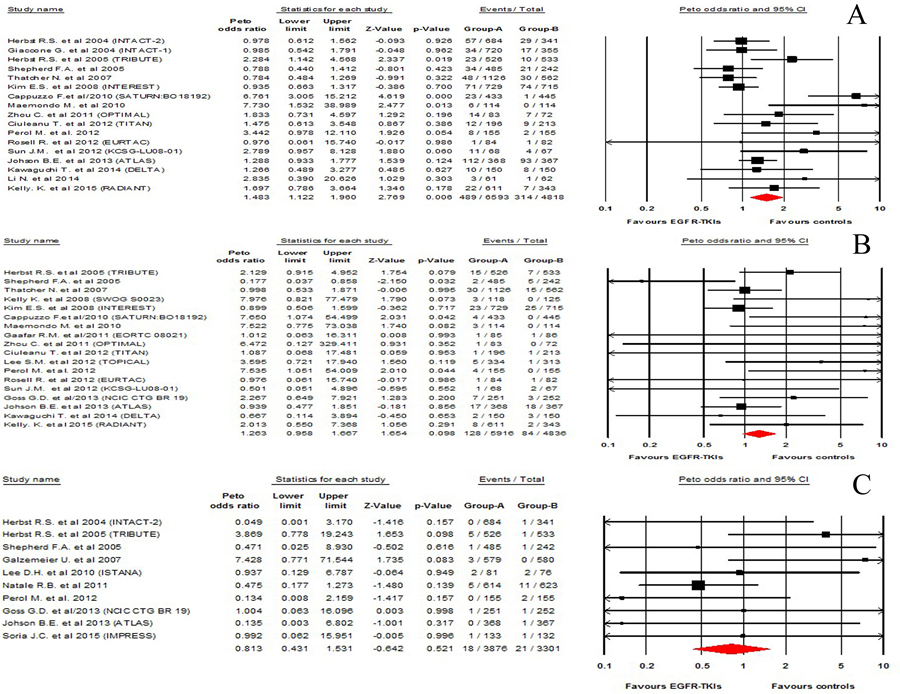
Figure 2: Risk of infections associated with EGFR-TKIs treatment compared with placebo treatment: A. all-grade infections, B. high-grade infections, C. fatal infections.
Risk of specific infections
We performed analysis to analyze the risk of all-grade infections based on specific type of infection. There was an increased risk of developing EGFR-TKIs-related infections (Peto OR 1.34, 95%CI: 1.08-1.66, p = 0.008) and febrile neutropenia (Peto OR 2.48, 95%CI: 1.31-4.69, p = 0.005), but not for pneumonia (Peto OR 0.97, 95%CI: 0.73-1.29, p = 0.82).
Publication bias
Egger’s test and Begg’s test was used to detect publication bias. There was no evidence of publication bias for the primary endpoint of this meta-analysis (Peto OR of all-grade infections; Begg’s test p = 0.12; Egger’s test p = 0.06).
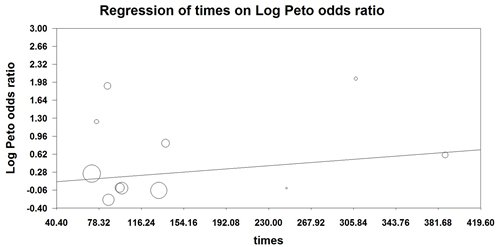
Figure 3: Meta-regression analysis of trends between treatment duration and relative risk of infections: symbols: each study is represented by a circle the diameter of which is proportional to its statistical weight.
Discussion
The introduction of novel targeted agents into the treatment of cancer has led to improve overall survival of many solid tumors. However, infection is an emerging complication with these drugs, and concerns have arisen regarding the potential risk of developing infections associated with targeted agents. Rafailidis et al [42] conducted the first systematic review in 2007 and demonstrated that there was an increased risk of developing monoclonal antibodies related severe infections but not for fatal adverse events. In consistent with previous results, two later meta-analyses also showed that EGFR-monoclonal antibodies significantly increased the risk of developing severe infections but not for fatal adverse events [16, 43]. Recently, Qi et al. performed another meta-analysis and showed that there was an increased risk of developing all-grade (RR 1.45, p < 0.001) and high-grade (RR 1.59, p < 0.001) infectious events in cancer patients treated with bevacizumab [44]. However, whether the use of EGFR-TKIs would increase the risk of infections in NSCLC remains undetermined.
A total of 17,420 NSCLC patients from 25 RCTs is included for analysis. As far as we known, our study is the first large meta-analysis to show a significantly increased risk of developing EGFR-TKIs related infection (Peto OR 1.48, p = 0.006) in NSCLC patients, but not for high-grade and fatal infectious events. Moreover, we perform a meta-regression analysis to assess the relationship between EGFR-TKIs treatment duration and risk of infections. The result shows that the peto OR of all-grade infections tends to be increased with EGFR-TKIs treatment duration, but it is not statistically significant (p = 0.26). As a result, clinicians should pay more attention to the risk of infections during the administration of EGFR-TKIs. Moreover, clinicians should treat NSCLC patients with any active infection before the initiation of EGFR-TKIs treatment.
Multiple mechanisms might involve in the development of infection. Basic research conducted by Lewkowicz et al [45] found TNF-α induced respiratory burst and phagocytic activity could be enhances by EGFR and its signal pathway. A recent study conducted by Li et al also demonstrated that EGFR play a critical role in the process of Tamm-Horsfall glycoprotein-enhanced neutrophil phagocytosis, and this effect could be suppressed by EGFR inhibitor [46]. However, more high-quality research are still recommended to determine the mechanisms of EGFR-TKIs associated infections.
Several limitations need to be mentioned in the present study. Firstly, as our study is a retrospective analysis of published studies, the baseline characteristics of each studies, such as dosage of EGFR-TKIs, periods of study conduct, and treatment regimens, might be potentially different, which might increase the heterogeneity among included studies. Second, we could not get individual patient data from each published studies, thus we could not perform a comprehensive analysis by adjusting baseline factors that existed between included trials.
Conclusions
In conclusion, our study has demonstrated that treatment with EGFR-TKIs in advanced NSCLC is associated with an increased risk of all-grade infections, but not for high-grade and fatal infections. Clinicians should be aware of these risks and provide regular follow-up for these toxicities.
materials and Methods
Data sources
We performed this systematic review adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements [47]. Our study was a meta-analysis of published data, and all of these included trials had been approved by the ethics committee, thus the ethical approval in our study was waved. To identify studies for inclusion in this study, we did a broad search of four databases, including Embase, Medline, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews, from the date of inception of every database to December 2015. Key words were “erlotinib”, “gefitinib”, “non-small-cell lung cancer”, “lung carcinoma”, “lung neoplasm”, “randomized controlled trial” and “infections”. The search was limited to prospective randomized clinical trials published in English. Each publication was reviewed and in cases of duplicate publications only the most complete, recent, and updated report of the clinical trial was included in the meta-analysis.
Study selection
To be included for analysis in our systematic review and meta-analysis, the trials had to meet all the following criteria: 1) patients with pathologically confirmed non-small-cell lung cancer; 2) trials comparing therapy with or without EGFR-TKIs (erlotinib and gefitinib); 3) the included study had sufficient data for extraction. We assessed the quality of reports of clinical trials by using the 5-item Jadad scale including randomization, double-blinding, and withdrawals as previously described [48, 49].
Data extraction and clinical end point
Two independent investigators reviewed the titles and abstracts of potentially relevant studies. We retrieved the full text of relevant studies for further review by the same two reviewers. A third senior investigator resolved any discrepancies between reviewers. If reviewers suspected an overlap of cohorts in a report, they contacted the corresponding author for clarification; we excluded studies with a clear overlap. We extracted the following data: first author’s name, year of publication, number of enrolled subjects, treatment regimens, number of patients in treatment and controlled groups, median age, median treatment duration, median progression-free survival, median overall survival and adverse outcomes of interest (infections). The following adverse outcomes were considered as infectious events and were included in the analyses: Infections (not specified), febrile neutropenia, sepsis, septic shock, lung infection, respiratory tract infection and pneumonia. Adverse events of severe infections (≥grade 3), as assessed and recorded according to the National Cancer Institute’s common terminology criteria (NCI-CTC, version 2 or 3; http://ctep.cancer.gov), were extracted for analysis, which has been widely used in cancer clinical trials.
Statistical analysis
Statistical analysis of the overall incidence and relative risk for all-grade, high-grade and fatal infections was calculated using comprehensive meta-analysis software version 2.0(Biostat, Englewood, NJ, USA). We used the Peto method to calculate ORs and 95% CIs because this method provided the best confidence interval coverage and was more powerful and relatively less biased than the fixed or random effects analysis when dealing with low event rates [50]. To calculate peto odds ratio (OR), patients assigned to EGFR-TKIs were compared only with those assigned to control treatment in the same trial. Additionally, to test whether effect sizes were moderated by differences in length of treatment, we carried out meta-regressions with difference in median length of experimental treatments (expressed in days) as predictor and relative risk as dependent variable. Between-study heterogeneity was estimated using the χ2-based Q statistic [51]. Heterogeneity was considered statistically significant when P heterogeneity < 0.1. If heterogeneity existed, data was analyzed using a random effects model according to the method of DerSimonian and Laird [52]. In the absence of heterogeneity, the pooled estimate calculated on the basis of the fixed-effects model was reported using an inverse variance method. A statistical test with a p-value less than 0.05 was considered significant. The presence of publication bias was evaluated by using the Begg and Egger tests [53].
Conflicts of interest
The authors report no conflicts of interest in this work.
References
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69–90.
2. Azzoli CG, Baker S Jr, Temin S, Pao W, Aliff T, Brahmer J, Johnson DH, Laskin JL, Masters G, Milton D, Nordquist L, Pfister DG, Piantadosi S, et al, and American Society of Clinical Oncology. American Society of Clinical Oncology Clinical Practice Guideline update on chemotherapy for stage IV non-small-cell lung cancer. J Clin Oncol. 2009; 27:6251–66.
3. Spiro SG, Silvestri GA. One hundred years of lung cancer. Am J Respir Crit Care Med. 2005; 172:523–29.
4. Goffin JR, Zbuk K. Epidermal growth factor receptor: pathway, therapies, and pipeline. Clin Ther. 2013; 35:1282–303.
5. Normanno N, De Luca A, Bianco C, Strizzi L, Mancino M, Maiello MR, Carotenuto A, De Feo G, Caponigro F, Salomon DS. Epidermal growth factor receptor (EGFR) signaling in cancer. Gene. 2006; 366:2–16.
6. Kari C, Chan TO, Rocha de Quadros M, Rodeck U. Targeting the epidermal growth factor receptor in cancer: apoptosis takes center stage. Cancer Res. 2003; 63:1–5.
7. Scaltriti M, Baselga J. The epidermal growth factor receptor pathway: a model for targeted therapy. Clin Cancer Res. 2006; 12:5268–72.
8. Lee CK, Brown C, Gralla RJ, Hirsh V, Thongprasert S, Tsai CM, Tan EH, Ho JC, Chu T, Zaatar A, Osorio Sanchez JA, Vu VV, Au JS, et al. Impact of EGFR inhibitor in non-small cell lung cancer on progression-free and overall survival: a meta-analysis. J Natl Cancer Inst. 2013; 105:595–605.
9. Ellis PM, Coakley N, Feld R, Kuruvilla S, Ung YC. Use of the epidermal growth factor receptor inhibitors gefitinib, erlotinib, afatinib, dacomitinib, and icotinib in the treatment of non-small-cell lung cancer: a systematic review. Curr Oncol. 2015; 22:e183–215.
10. Landi L, Cappuzzo F. Experience with erlotinib in the treatment of non-small cell lung cancer. Ther Adv Respir Dis. 2015; 9:146–63.
11. Petrelli F, Cabiddu M, Borgonovo K, Barni S. Risk of venous and arterial thromboembolic events associated with anti-EGFR agents: a meta-analysis of randomized clinical trials. Ann Oncol. 2012; 23:1672–79.
12. Jia Y, Lacouture ME, Su X, Wu S. Risk of skin rash associated with erlotinib in cancer patients: a meta-analysis. J Support Oncol. 2009; 7:211–17.
13. Abdel-Rahman O, Elhalawani H. Risk of fatal pulmonary events in patients with advanced non-small-cell lung cancer treated with EGF receptor tyrosine kinase inhibitors: a comparative meta-analysis. Future Oncol. 2015; 11:1109–22.
14. Qi WX, Sun YJ, Shen Z, Yao Y. Risk of interstitial lung disease associated with EGFR-TKIs in advanced non-small-cell lung cancer: a meta-analysis of 24 phase III clinical trials. J Chemother. 2015; 27:40–51.
15. Shi L, Tang J, Tong L, Liu Z. Risk of interstitial lung disease with gefitinib and erlotinib in advanced non-small cell lung cancer: a systematic review and meta-analysis of clinical trials. Lung Cancer. 2014; 83:231–39.
16. Qi WX, Fu S, Zhang Q, Guo XM. Incidence and risk of severe infections associated with anti-epidermal growth factor receptor monoclonal antibodies in cancer patients: a systematic review and meta-analysis. BMC Med. 2014; 12:203.
17. Soria JC, Wu YL, Nakagawa K, Kim SW, Yang JJ, Ahn MJ, Wang J, Yang JC, Lu Y, Atagi S, Ponce S, Lee DH, Liu Y, et al. Gefitinib plus chemotherapy versus placebo plus chemotherapy in EGFR-mutation-positive non-small-cell lung cancer after progression on first-line gefitinib (IMPRESS): a phase 3 randomised trial. Lancet Oncol. 2015; 16:990–98.
18. Kelly K, Altorki NK, Eberhardt WE, O’Brien ME, Spigel DR, Crinò L, Tsai CM, Kim JH, Cho EK, Hoffman PC, Orlov SV, Serwatowski P, Wang J, et al. Adjuvant Erlotinib Versus Placebo in Patients With Stage IB-IIIA Non-Small-Cell Lung Cancer (RADIANT): A Randomized, Double-Blind, Phase III Trial. J Clin Oncol. 2015; 33:4007–14.
19. Li N, Ou W, Yang H, Liu QW, Zhang SL, Wang BX, Wang SY. A randomized phase 2 trial of erlotinib versus pemetrexed as second-line therapy in the treatment of patients with advanced EGFR wild-type and EGFR FISH-positive lung adenocarcinoma. Cancer. 2014; 120:1379–86.
20. Kawaguchi T, Ando M, Asami K, Okano Y, Fukuda M, Nakagawa H, Ibata H, Kozuki T, Endo T, Tamura A, Kamimura M, Sakamoto K, Yoshimi M, et al. Randomized phase III trial of erlotinib versus docetaxel as second- or third-line therapy in patients with advanced non-small-cell lung cancer: Docetaxel and Erlotinib Lung Cancer Trial (DELTA). J Clin Oncol. 2014; 32:1902–08.
21. Johnson BE, Kabbinavar F, Fehrenbacher L, Hainsworth J, Kasubhai S, Kressel B, Lin CY, Marsland T, Patel T, Polikoff J, Rubin M, White L, Yang JC, et al. ATLAS: randomized, double-blind, placebo-controlled, phase IIIB trial comparing bevacizumab therapy with or without erlotinib, after completion of chemotherapy, with bevacizumab for first-line treatment of advanced non-small-cell lung cancer. J Clin Oncol. 2013; 31:3926–34.
22. Goss GD, O’Callaghan C, Lorimer I, Tsao MS, Masters GA, Jett J, Edelman MJ, Lilenbaum R, Choy H, Khuri F, Pisters K, Gandara D, Kernstine K, et al. Gefitinib versus placebo in completely resected non-small-cell lung cancer: results of the NCIC CTG BR19 study. J Clin Oncol. 2013; 31:3320–26.
23. Sun JM, Lee KH, Kim SW, Lee DH, Min YJ, Yun HJ, Kim HK, Song HS, Kim YH, Kim BS, Hwang IG, Lee K, Jo SJ, et al, and Korean Cancer Study Group. Gefitinib versus pemetrexed as second-line treatment in patients with nonsmall cell lung cancer previously treated with platinum-based chemotherapy (KCSG-LU08-01): an open-label, phase 3 trial. Cancer. 2012; 118:6234–42.
24. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, Porta R, Cobo M, Garrido P, et al, and Spanish Lung Cancer Group in collaboration with Groupe Français de Pneumo-Cancérologie and Associazione Italiana Oncologia Toracica. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012; 13:239–46.
25. Pérol M, Chouaid C, Pérol D, Barlési F, Gervais R, Westeel V, Crequit J, Léna H, Vergnenègre A, Zalcman G, Monnet I, Le Caer H, Fournel P, et al. Randomized, phase III study of gemcitabine or erlotinib maintenance therapy versus observation, with predefined second-line treatment, after cisplatin-gemcitabine induction chemotherapy in advanced non-small-cell lung cancer. J Clin Oncol. 2012; 30:3516–24.
26. Lee SM, Khan I, Upadhyay S, Lewanski C, Falk S, Skailes G, Marshall E, Woll PJ, Hatton M, Lal R, Jones R, Toy E, Chao D, et al. First-line erlotinib in patients with advanced non-small-cell lung cancer unsuitable for chemotherapy (TOPICAL): a double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2012; 13:1161–70.
27. Ciuleanu T, Stelmakh L, Cicenas S, Miliauskas S, Grigorescu AC, Hillenbach C, Johannsdottir HK, Klughammer B, Gonzalez EE. Efficacy and safety of erlotinib versus chemotherapy in second-line treatment of patients with advanced, non-small-cell lung cancer with poor prognosis (TITAN): a randomised multicentre, open-label, phase 3 study. Lancet Oncol. 2012; 13:300–08.
28. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, Zhang S, Wang J, Zhou S, Ren S, Lu S, Zhang L, Hu C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011; 12:735–42.
29. Natale RB, Thongprasert S, Greco FA, Thomas M, Tsai CM, Sunpaweravong P, Ferry D, Mulatero C, Whorf R, Thompson J, Barlesi F, Langmuir P, Gogov S, et al. Phase III trial of vandetanib compared with erlotinib in patients with previously treated advanced non-small-cell lung cancer. J Clin Oncol. 2011; 29:1059–66.
30. Gaafar RM, Surmont VF, Scagliotti GV, Van Klaveren RJ, Papamichael D, Welch JJ, Hasan B, Torri V, van Meerbeeck JP, EORTC Lung Cancer Group, The Italian Lung Cancer Project. A double-blind, randomised, placebo-controlled phase III intergroup study of gefitinib in patients with advanced NSCLC, non-progressing after first line platinum-based chemotherapy (EORTC 08021/ILCP 01/03). Eur J Cancer. 2011; 47:2331–40.
31. Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I, Fujita Y, Okinaga S, Hirano H, et al, and North-East Japan Study Group. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010; 362:2380–88.
32. Lee DH, Park K, Kim JH, Lee JS, Shin SW, Kang JH, Ahn MJ, Ahn JS, Suh C, Kim SW. Randomized Phase III trial of gefitinib versus docetaxel in non-small cell lung cancer patients who have previously received platinum-based chemotherapy. Clin Cancer Res. 2010; 16:1307–14.
33. Cappuzzo F, Ciuleanu T, Stelmakh L, Cicenas S, Szczésna A, Juhász E, Esteban E, Molinier O, Brugger W, Melezínek I, Klingelschmitt G, Klughammer B, Giaccone G, et al. Erlotinib as maintenance treatment in advanced non-small-cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2010; 11:521–29.
34. Kim ES, Hirsh V, Mok T, Socinski MA, Gervais R, Wu YL, Li LY, Watkins CL, Sellers MV, Lowe ES, Sun Y, Liao ML, Osterlind K, et al. Gefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised phase III trial. Lancet. 2008; 372:1809–18.
35. Kelly K, Chansky K, Gaspar LE, Albain KS, Jett J, Ung YC, Lau DH, Crowley JJ, Gandara DR. Phase III trial of maintenance gefitinib or placebo after concurrent chemoradiotherapy and docetaxel consolidation in inoperable stage III non-small-cell lung cancer: SWOG S0023. J Clin Oncol. 2008; 26:2450–56.
36. Gatzemeier U, Pluzanska A, Szczesna A, Kaukel E, Roubec J, De Rosa F, Milanowski J, Karnicka-Mlodkowski H, Pesek M, Serwatowski P, Ramlau R, Janaskova T, Vansteenkiste J, et al. Phase III study of erlotinib in combination with cisplatin and gemcitabine in advanced non-small-cell lung cancer: the Tarceva Lung Cancer Investigation Trial. J Clin Oncol. 2007; 25:1545–52.
37. Thatcher N, Chang A, Parikh P, Rodrigues Pereira J, Ciuleanu T, von Pawel J, Thongprasert S, Tan EH, Pemberton K, Archer V, Carroll K. Gefitinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet. 2005; 366:1527–37.
38. Shepherd FA, Rodrigues Pereira J, Ciuleanu T, Tan EH, Hirsh V, Thongprasert S, Campos D, Maoleekoonpiroj S, Smylie M, Martins R, van Kooten M, Dediu M, Findlay B, et al, and National Cancer Institute of Canada Clinical Trials Group. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005; 353:123–32.
39. Herbst RS, Prager D, Hermann R, Fehrenbacher L, Johnson BE, Sandler A, Kris MG, Tran HT, Klein P, Li X, Ramies D, Johnson DH, Miller VA, et al. TRIBUTE: a phase III trial of erlotinib hydrochloride (OSI-774) combined with carboplatin and paclitaxel chemotherapy in advanced non-small-cell lung cancer. J Clin Oncol. 2005; 23:5892–99.
40. Herbst RS, Giaccone G, Schiller JH, Natale RB, Miller V, Manegold C, Scagliotti G, Rosell R, Oliff I, Reeves JA, Wolf MK, Krebs AD, Averbuch SD, et al. Gefitinib in combination with paclitaxel and carboplatin in advanced non-small-cell lung cancer: a phase III trial—INTACT 2. J Clin Oncol. 2004; 22:785–94.
41. Giaccone G, Herbst RS, Manegold C, Scagliotti G, Rosell R, Miller V, Natale RB, Schiller JH, Von Pawel J, Pluzanska A, Gatzemeier U, Grous J, Ochs JS, et al. Gefitinib in combination with gemcitabine and cisplatin in advanced non-small-cell lung cancer: a phase III trial—INTACT 1. J Clin Oncol. 2004; 22:777–84.
42. Rafailidis PI, Kakisi OK, Vardakas K, Falagas ME. Infectious complications of monoclonal antibodies used in cancer therapy: a systematic review of the evidence from randomized controlled trials. Cancer. 2007; 109:2182–89.
43. Funakoshi T, Suzuki M, Tamura K. Infectious complications in cancer patients treated with anti-EGFR monoclonal antibodies cetuximab and panitumumab: a systematic review and meta-analysis. Cancer Treat Rev. 2014; 40:1221–29.
44. Qi WX, Fu S, Zhang Q, Guo XM. Bevacizumab increases the risk of infections in cancer patients: A systematic review and pooled analysis of 41 randomized controlled trials. Crit Rev Oncol Hematol. 2015; 94:323–36.
45. Lewkowicz P, Tchórzewski H, Dytnerska K, Banasik M, Lewkowicz N. Epidermal growth factor enhances TNF-alpha-induced priming of human neutrophils. Immunol Lett. 2005; 96:203–10.
46. Li KJ, Siao SC, Wu CH, Shen CY, Wu TH, Tsai CY, Hsieh SC, Yu CL. EGF receptor-dependent mechanism may be involved in the Tamm-Horsfall glycoprotein-enhanced PMN phagocytosis via activating Rho family and MAPK signaling pathway. Molecules. 2014; 19:1328–43.
47. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009; 62:1006–12.
48. Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, Tugwell P, Klassen TP. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet. 1998; 352:609–13.
49. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996; 17:1–12.
50. Sweeting MJ, Sutton AJ, Lambert PC. What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data. Stat Med. 2004; 23:1351–75.
51. Zintzaras E, Ioannidis JP. Heterogeneity testing in meta-analysis of genome searches. Genet Epidemiol. 2005; 28:123–37.
52. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986; 7:177–88.
53. Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000; 53:1119–29.