
INTRODUCTION
Triple-negative breast cancer (TNBC) is characterized by a lack of expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) and represents up to 20% of all breast cancers. This subtype is a heterogeneous tumor that encompasses other breast cancer molecular subtypes. In general, TNBC is a high-grade, aggressive disease with a high rate of distant metastasis, and is associated with a poorer outcome than other breast cancer subtypes, despite a good response to standard chemotherapy regimens [1]. Therefore, further definition of these subclasses and novel therapeutic strategies are needed to predict prognosis and choose appropriate treatments for patients with TNBC.
Tumor-infiltrating lymphocytes (TILs) have been shown to have prognostic and predictive value in both adjuvant [2–4] and neoadjuvant settings [5–7] in breast cancer, especially in TN and HER2 breast cancers. TILs (both stromal and intratumoral) are associated with high histologic grade, hormone receptor negativity and high Ki-67 expression [2], possibly as a result of the load of somatic mutation. In TNBC in particular, a high number of stromal TILs is predictive of a more favorable outcome, and the prognostic value of stromal TILs can be considered strong evidence. However, according to the International TILs Working Group, TILs should not yet be used as a biomarker for withholding chemotherapy [8].
The programmed cell death protein 1 (PD-1, also known as CD279) pathway plays a crucial role in regulating immune responses. Programmed cell death ligand-1 (PD-L1, ligand for PD-1; also known as B7-H1 or CD274) on tumor cells is upregulated by constitutive oncogenic signaling (innate resistance) or by inflammatory signals in the tumor microenvironment (adaptive resistance), such as interferon-γ (INF-γ) produced by some activated T cells and natural killer cells [9]. Although some results remain controversial [10], PD-L1 expression reportedly correlates with a poor clinical outcome in several types of malignancy, and may be a predictive marker of PD-1/PD-L1 pathway inhibition [11–13]. In TNBC, the value of PD-L1 expression as a biomarker has so far been controversial [14–18] and the underlying molecular mechanisms remain unclear. Therefore, further studies are needed to identify immune biomarkers for the selection of patients who would most likely benefit from novel immunotherapies.
In the present study, we retrospectively analyzed PD-L1 expression and stromal TILs in 248 TNBCs. We also explored the correlation between immunologic features on tumors and immune cells and the clinicopathological characteristics of the tumors, their response to chemotherapy and clinical outcome.
RESULTS
Clinicopathological features, PD-L1 expression, and TILs
We evaluated 248 TN tumors with respect to the clinicopathological data (Table 1), PD-L1 expression on tumor cells (Supplementary Table 1 and Supplementary Figure 1) and stromal TILs (Supplementary Figure 2). Among the 248 TN tumors, PD-L1 expression was classified as strong-positive in 38 (15.3%), weak-positive in 65 (26.2%), and negative in 145 (58.5%) (Supplementary Table 1). Stromal TILs were present at a high level in 118 (47.6%) of the tumors (Supplementary Table 2). The breakdown of these results is as follows: high levels of TILs were present in 35 (92.1%) PD-L1 strong-positive tumors, 52 (80.0%) PD-L1 weak-positive tumors, and 31 (21.4%) PD-L1-negative tumors (Figure 1). Positive PD-L1 expression was significantly correlated with high levels of TILs (P < 0.0001, Figure 1). Patients with PD-L1-positive tumors were younger than those with PD-L1-negative tumors (P = 0.007). The nuclear grade and Ki-67 index were higher in PD-L1-positive tumors than in PD-L1-negative tumors (P = 0.0015 and P < 0.0001, respectively), although there was no significant difference between the two groups with respect to tumor size, nodal status and pathological stage (Table 1). We also evaluated PD-L1 expression on tumor-infiltrating immune cells (PD-L1IC expression). PD-L1IC-positive tumors were observed in 129 (52.0%) of the TN tumors (Supplementary Table 1 and Supplementary Figure 3). Positive PD-L1 expression on tumor cells was significantly correlated with positive PD-L1IC expression (Table 1).
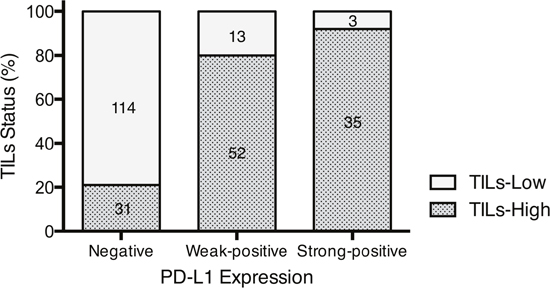
Figure 1: Relationship between PD-L1 expression and TILs status. Figures within this bar graph depict absolute numbers of cases. The result of Cochran-Armitage test for trend was P < 0.0001.
Table 1: Patients and tumor characteristics in TNBC
PD-L1-Positive |
PD-L1-Negative |
P |
|||
|---|---|---|---|---|---|
N = 103 (41.5%) |
N = 145 (58.5%) |
||||
Age at diagnosis |
|||||
Mean (range) |
57.4 |
(32–84) |
61.8 |
(30–89) |
0.007a) |
Tumor size |
|||||
T1a/b (≤ 1 cm) |
6 |
(5.8%) |
14 |
(9.7%) |
0.71b) |
T1c (> 1 cm, ≤ 2 cm) |
55 |
(53.4%) |
71 |
(49.0%) |
|
T2 (> 2 cm, ≤ 5 cm) |
39 |
(37.9%) |
55 |
(37.9%) |
|
T3 (> 5 cm) |
3 |
(2.9%) |
5 |
(3.4%) |
|
Nodal status |
|||||
N0 |
67 |
(65.0%) |
100 |
(69.0%) |
0.84b) |
N1 (1−3) |
25 |
(24.3%) |
33 |
(22.8%) |
|
N2 (4−9) |
7 |
(6.8%) |
7 |
(4.8%) |
|
N3 (≥10) |
4 |
(3.9%) |
4 |
(2.7%) |
|
Unknown |
1 |
(0.7%) |
|||
Pathological stage |
|||||
I |
43 |
(41.7%) |
63 |
(43.4%) |
0.71b) |
II |
49 |
(47.6%) |
71 |
(49.0%) |
|
III |
11 |
(10.7%) |
11 |
(7.6%) |
|
Nuclear grade |
|||||
1+2 |
19 |
(18.4%) |
54 |
(37.2%) |
0.0015b) |
3 |
80 |
(77.7%) |
88 |
(60.7%) |
|
Unknown |
4 |
(3.9%) |
3 |
(2.1%) |
|
Ki-67 |
|||||
≤ 30% |
6 |
(5.8%) |
42 |
(29.0%) |
< 0.0001b) |
> 30% |
83 |
(80.6%) |
84 |
(57.9%) |
|
Unknown |
14 |
(13.6%) |
19 |
(13.1%) |
|
PD-L1 on immune cells |
|||||
Negative |
17 |
(16.5%) |
102 |
(70.3%) |
< 0.0001b) |
Positive |
86 |
(83.5%) |
43 |
(29.7%) |
|
TILs |
|||||
Low |
16 |
(15.5%) |
114 |
(78.6%) |
< 0.0001b) |
High |
87 |
(84.5%) |
31 |
(21.4%) |
|
a) Logistic regression, b) Pearson's χ2 test.
Patient survival
The median follow-up in this cohort was 68 months (range 2–150 months). There was no significant difference in recurrence-free survival (RFS) and overall survival (OS) between patients with PD-L1-positive tumors and those with PD-L1-negative tumors (Figure 2A, 2B), and also there was no difference between patients with PD-L1IC-positive tumors and those with PD-L1IC-negative tumors (Supplementary Figure 4). Although there was no significant difference in RFS between patients with TILs-high and TILs-low tumors (Figure 2C), patients with TILs-high tumors had significantly better OS than those with TILs-low tumors (P = 0.016, Figure 2D).
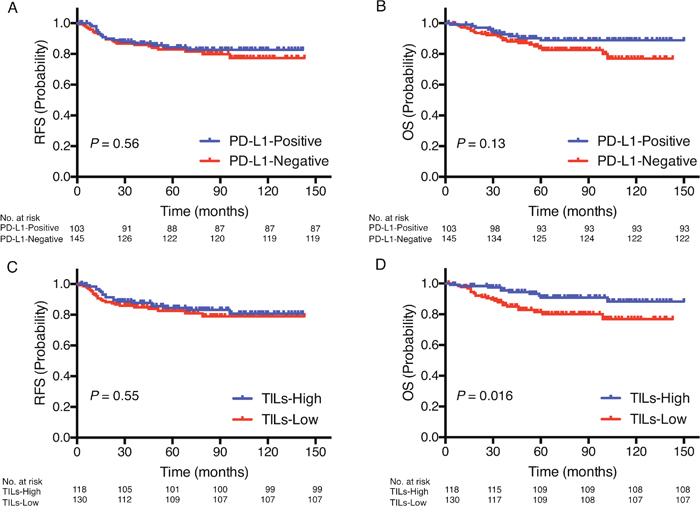
Figure 2: Prognostic value of PD-L1 expression and TILs status. Kaplan-Meier curves showing estimated RFS A. and OS B. for PD-L1 expression as well as RFS C. and OS D. for TILs status. P values are for comparison of two groups.
The Cox proportional hazards model showed a significant interaction between PD-L1 and TILs (P = 0.0018 for RFS; P = 0.015 for OS, Table 2); that is, PD-L1 expression and TILs were not independent prognostic factors. The patients were therefore divided into four subgroups: PD-L1-positive/TILs-high, PD-L1-positive/TILs-low, PD-L1-negative/TILs-high and PD-L1-negative/TILs-low. Kaplan-Meier graphical analysis demonstrated that both RFS (P = 0.0045, Figure 3A) and OS (P = 0.0036, Figure 3B) differed significantly among the four subgroups. The treatment background of these four subgroups did not significantly differ (Supplementary Table 3).
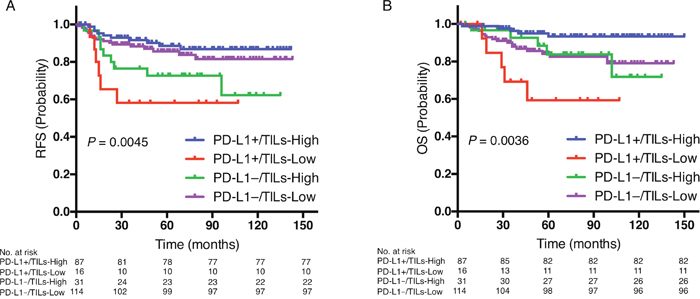
Figure 3: Prognostic value of the combination of PD-L1 expression and TILs status. Kaplan-Meier curves showing estimated RFS A. and OS B. for PD-L1-positive/TILs-high, PD-L1-positive/TILs-low, PD-L1-negative/TILs-high, and PD-L1-negative/TILs-low. P values are for comparison of four groups.
Table 2: Interaction between PD-L1 and TILs in a Cox proportional hazards model
Recurrence-free survival |
Overall survival |
||||
|---|---|---|---|---|---|
Likelihood ratio χ2 |
P |
Likelihood ratio χ2 |
P |
||
PD-L1 |
(Positive vs. Negative) |
0.07 |
0.79 |
0.04 |
0.85 |
TILs |
(High vs. Low) |
1.71 |
0.19 |
7.03 |
0.008 |
PD-L1*TILs |
9.72 |
0.0018 |
6.00 |
0.015 |
|
* Interaction.
Univariate and multivariate survival analysis
Univariate analysis of the clinicopathological characteristics revealed that tumor size (> 2 cm) and lymph node involvement were significantly related to poorer RFS and OS, while TILs-high tumors were significantly related to better OS (Table 3A). In addition, when we compared the PD-L1-positive/TILs-high subgroup, which had the longest RFS and OS, with other three subgroups, the PD-L1-positive/TILs-low subgroup had significant greater recurrence and death risks (for RFS: hazard ratio [HR] = 4.7, 95% confidence interval [CI] 1.6–12.7, P = 0.0067; for OS: HR = 8.4, 95% CI 2.3–30.3, P = 0.019, Table 3A).
Table 3: Cox proportional hazards model for recurrence-free and overall survival
A. Univariate analysis
Variables |
Recurrence-free survival |
Overall survival |
|||||
|---|---|---|---|---|---|---|---|
HR |
95% CI |
P |
HR |
95% CI |
P |
||
Age |
(> 50 vs. ≤ 50) |
1.1 |
0.5−2.3 |
0.85 |
1.2 |
0.6−3.1 |
0.62 |
Tumor size |
(> 2 cm vs. ≤ 2 cm) |
2.7 |
1.5−5.1 |
0.0015 |
2.6 |
1.3−5.3 |
0.0075 |
Nodal status |
(Positive vs. Negative) |
2.8 |
1.5−5.1 |
0.0011 |
2.1 |
1.1−4.3 |
0.032 |
Nuclear grade |
(3 vs. 1 and 2) |
1.0 |
0.5−2.1 |
0.99 |
0.7 |
0.4−1.6 |
0.44 |
Ki-67 |
(> 30% vs. ≤ 30%) |
1.8 |
0.8−5.2 |
0.21 |
1.2 |
0.5−3.2 |
0.72 |
PD-L1 |
(Positive vs. Negative) |
0.8 |
0.4−1.5 |
0.56 |
0.6 |
0.3−1.2 |
0.13 |
PD-L1IC |
(Positive vs. Negative) |
0.6 |
0.3−1.1 |
0.09 |
0.7 |
0.4-1.4 |
0.35 |
TILs |
(High vs. Low) |
0.8 |
0.4−1.5 |
0.55 |
0.4 |
0.2−0.8 |
0.015 |
PD-L1*TILs |
(PD-L1+/TILs-Low vs. PD-L1+/TILs-High) |
4.7 |
1.6−12.7 |
0.0067 |
8.4 |
2.3−30.3 |
0.0019 |
(PD-L1–/TILs-High vs. PD-L1+/TILs-High) |
2.8 |
1.1−6.9 |
0.031 |
3.1 |
0.9−11.1 |
0.083 |
|
(PD-L1–/TILs-Low vs. PD-L1+/TILs-High) |
1.4 |
0.7−3.2 |
0.38 |
3.2 |
1.3−9.7 |
0.013 |
|
B. Multivariate analysis
Variables |
Recurrence-free survival |
Overall survival |
|||||
|---|---|---|---|---|---|---|---|
HR |
95% CI |
P |
HR |
95% CI |
P |
||
Tumor size |
(> 2 cm vs. ≤ 2 cm) |
2.4 |
1.3−4.5 |
0.007 |
2.1 |
1.1−4.5 |
0.034 |
Nodal status |
(Positive vs. Negative) |
2.3 |
1.2−4.2 |
0.011 |
1.9 |
0.9−3.8 |
0.083 |
PD-L1*TILs |
(PD-L1+/TILs-Low vs. PD-L1+/TILs-High) |
4.1 |
1.4−11.1 |
0.014 |
7.2 |
2.0−26.2 |
0.0038 |
(PD-L1–/TILs-High vs. PD-L1+/TILs-High) |
2.6 |
1.0−6.5 |
0.043 |
2.9 |
0.8−10.4 |
0.11 |
|
(PD-L1–/TILs-Low vs. PD-L1+/TILs-High) |
1.5 |
0.7−3.3 |
0.34 |
3.2 |
1.3−9.9 |
0.011 |
|
* Interaction; HR, hazard ratio; CI, confidence interval; +, positive; –, negative.
As individual factors, PD-L1 and TILs status were excluded from the multivariate analysis, because they were included in the four subgroups defined by combining the PD-L1 and TILs status. Age at diagnosis, nuclear grade, Ki-67 index and PD-L1IC were also excluded from the multivariate analysis through the back elimination method. The multivariate analysis revealed that a tumor size (> 2 cm) and the PD-L1-positive/TILs-low subgroup were independent and negative prognostic factors for both RFS and OS (Table 3B).
DISCUSSION
PD-L1 positivity in TNBC ranged from 19% to 58% in two previous studies [14, 19]. Differences in the cut-off value and primary antibody are likely reasons for the discrepancy in the percentages of PD-L1 expression between the two studies. Although studies have been conducted to analyze the relationship between PD-L1 and breast cancer, including all subtypes, the prognosis of patients with PD-L1-positive tumors remains controversial: PD-L1 was related to a poor prognosis [19–21], whereas PD-L1 expression was a good prognostic factor for breast cancer [16, 22], especially for basal-like tumors [17]. These controversial results might reflect the presence of multiple breast cancer subtypes, biological heterogeneity, or non-uniform methods for assessing PD-L1 status.
The International TILs Working Group recently issued recommendations for improving the consistency in scoring TILs, including detailed guidelines for annotating the prevalence of lymphocyte infiltration that may improve inter-observer reproducibility [23, 24]. We evaluated TILs according to these guidelines, and our data showed that patients with TILs-high tumors had significantly better OS than those with TILs-low tumors. This finding was consistent with the previous results of Pruneri et al. [8], who showed that each 10% increase in TILs strongly predicted better survival.
In the present study, PD-L1 expression was significantly correlated with higher levels of TILs. There few reports on the relationship between PD-L1 and TILs, and their results are controversial: higher CD8+ lymphocyte infiltration was related to lower PD-L1 expression in early-stage breast cancer [25], whereas PD-L1 expression showed a positive correlation with levels of infiltrating intratumoral CD8+ and FOXP3+ lymphocytes in breast cancer [18].
Our univariate analysis showed that PD-L1 expression on tumor cells was not a prognostic factor for RFS or OS. In combination, however, PD-L1 and TILs had a pronounced influence on patient prognosis, owing to interaction between PD-L1 and TILs. In addition, our multivariate analysis showed that the PD-L1-positive/TILs-low subgroup had the poorest prognosis, while the PD-L1-positive/TILs-high subgroup had the best prognosis among the four subgroups. Modulation of PD-L1 levels occurs via two major pathways, the intracellular (innate) signaling pathway mediated by PI3K/AKT/mTOR activation and/or the extracellular induced (adaptive) pathway mediated by IFNγ production by TILs and subsequent IFNGRs/JAK/STAT signaling in tumor cells [26]. When TILs levels are decreased in PD-L1-positive tumors, there may be aberrant activation of PI3K/AKT/mTOR signaling. Conversely, when levels of TILs are increased in PD-L1-positive tumors, there may be activation of IFNGRs/JAK/STAT signaling mediated by IFNγ production by TILs. Webb et al. showed that the PD-L1-positive/CD8+ tumors are associated with a better prognosis than PD-L1-negative/CD8+ or PD-L1-negative/CD8– tumors in high-grade serous ovarian cancer [27]. Teng et al. reported that four types of tumor microenvironment exist on the basis of their PD-L1 status and presence or absence of TILs [28]. Microenvirionments that are PD-L1-positive with TILs driving adaptive immune resistance are associated with the best prognosis.
This is the first report of an interaction between PD-L1 and TILs in breast cancer. The combination of PD-L1 and TILs may be the most robust factor predictive of prognosis in TNBC. Although PD-L1 expression is generally considered to indicate a poor prognosis [11–13], the prognosis of patients with PD-L1-positive/TILs-high tumors was improved. We therefore expect a positive effect of novel anti-PD-1/PD-L1 monoclonal antibody therapies in patients with PD-L1-positive/TILs-low tumors, for whom prognosis is currently poor. In fact, in a phase Ib trial for PD-L1-positive TNBCs (KEYNOTE-012), it was unclear whether PD-L1 expression was predictive of a clinical benefit with the PD-1 antibody pembrolizumab [29].
This study had several limitations. First, it included only retrospectively collected cases. Second, although we assessed the interactive effect PD-L1 and TILs, the causal relationship is not clear. Finally, these factors were not predictive of the response to treatments, including anthracycline- or taxane-based regimens (data not shown).
In conclusion, we report that PD-L1 expression on tumor cells is related to high TILs levels, and the combination of PD-L1-positive and TILs-low is associated with a poor prognosis in TNBC. Although additional research into the underlying mechanisms is necessary, these biomarkers may be useful for stratification for TNBC patients and for predicting their prognosis. Our findings support a rationale for the development of novel immune-targeted therapies, such as PD-1/PD-L1 inhibitors, for patients with TNBC.
MATERIALS AND METHODS
Patients
This study included 248 patients with primary TNBC who underwent resection without neoadjuvant chemotherapy at Kyushu University Hospital (Fukuoka, Japan), Hamanomachi Hospital (Fukuoka, Japan) or Kumamoto City Hospital (Kumamoto, Japan) between January 2004 and December 2014. About 20% of patients diagnosed with TNBC received neoadjuvant chemotherapy in our institutions and were excluded from this study. The patients received adjuvant treatment according to the National Comprehensive Cancer Network Guidelines for treatment of breast cancer (http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#breast), the Clinical Practice Guideline of Breast Cancer by the Japanese Breast Cancer Society (http://jbcs.xsrv.jp/guidline/, in Japanese), and the recommendations of the St. Gallen International Breast Cancer Conference [30–33]. The treatment characteristics for the patients are shown in Supplementary Table 3. The study conformed to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Kyushu University Hospital (No. 27-102).
Immunohistochemistry (IHC)
Tumor subtypes were identified using IHC on surgically resected tissue. All resected specimens used for IHC were fixed (fixation was begun within 1 h) in 10% neutral buffered formalin for 6 to 72 h. ER-positive or PR-positive tissues were defined as ≥ 1% of tumor cells staining positive for ER or PR. Cancer specimens were defined as HER2-positive when HER2 IHC staining was scored as 3+ according to the standard criteria [34, 35], or when HER2 gene amplification was detected using fluorescence spectroscopy with in situ hybridization. The primary anti-PD-L1 antibody (monoclonal rabbit, E1L3N; Cell Signaling Technology, Beverly, MA) was used with a Ventana Discovery XT automated stainer (Ventana Medical Systems, Tucson, AZ) according to the manufacturer’s protocol and using proprietary reagents. Briefly, slides were deparaffinized on the automated system with EZ Prep solution. A heat-induced antigen retrieval method was used in standard Cell Conditioning 1 with an incubation temperature of 95°C. The primary antibody was used at a 1:200 dilution and was incubated for 32 min. The secondary antibody was SignalStain Boost IHC Detection Reagent (Cell Signaling Technology). Slides were counterstained with hematoxylin, and a bluing reagent was used for counterstaining. Using the clinical trial assay to identify levels of PD-L1 expression on tumor cells that maximally predict clinical response to pembrolizumab [29], PD-L1 weak-positive was defined as membranous PD-L1 expression in 1–49% of tumor cells, and PD-L1 strong-positive was defined as expression in ≥ 50% of tumor cell (Supplementary Table 1 and Supplementary Figure 1). In addition, PD-L1IC-positive was defined as expression in ≥ 5% of tumor-infiltrating immune cells [12] (Supplementary Figure 3).
Evaluation of tumor-infiltrating lymphocytes
TILs were assessed in hematoxylin and eosin-stained sections, carefully following the guidelines published by the International TILs Working Group to standardize TILs evaluation [23, 24] while blinded to the clinical information. These recommendations mainly propose a focus on stromal TILs. Cases were defined as TILs-high for ≥ 50% stromal TILs, which is also known as lymphocyte-predominant breast cancer, and as TILs-low for < 50% stromal TILs (Supplementary Figure 2).
Statistics
Logistic regression was used to compare continuous variables and χ2 tests were used to compare categorical variables between the PD-L1-positive and PD-L1-negative groups. The survival endpoints evaluated were RFS and OS. RFS was defined as the time from surgery to recurrence, including both local relapse and metastatic disease. OS was defined as the time from surgery until the date of death from any cause. Survival curves were generated using the Kaplan-Meier method and compared with the log-rank test. Hazard ratios were calculated using Cox proportional hazards regression. Values of P < 0.05 were considered statistically significant. Statistical analysis was carried out using JMP® 11 (SAS Institute Inc., Cary, NC).
ACKNOWLEDGMENTS
The authors thank Hisako Okuma, Shoko Sadatomi, Kaori Nomiyama, Miyuki Omori, Hiroshi Fujii, and Hiroyuki Minami for their technical assistance. The authors received a Best Platform Presentation Award supported by the 14th Asian Breast Diseases Association Meeting & Symposium, 2016.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING
This work was supported by the Japan Society for the Promotion of Science KAKENHI; Grant No. 20591550, MK (Makoto Kubo).
Author contributions
HM and MK (Makoto Kubo) have contributed equally to this work. MK (Makoto Kubo) designed the research; HM, RY, MK (Masaya Kai), MY performed the research; RN, TO, NA, YO (Yasuhiro Okumura), MO, YO (Yoshinao Oda) provided the clinical samples. HM and JK analyzed the data; HM and MK (Makoto Kubo) wrote the paper; and MN is the supervision.
REFERENCES
1. Foulkes WD, Smith IE, Reis-Filho JS. Triple-Negative Breast Cancer. The new england journal of medicine. 2010; 363: 1938-1948.
2. Loi S, Sirtaine N, Piette F, Salgado R, Viale G, Van Eenoo F, Rouas G, Francis P, Crown JP, Hitre E, de Azambuja E, Quinaux E, Di Leo A, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol. 2013; 31: 860-867.
3. Loi S, Michiels S, Salgado R, Sirtaine N, Jose V, Fumagalli D, Kellokumpu- Lehtinen PL, Bono P, Kataja V, Desmedt C, Piccart MJ, Loibl S, Denkert C, et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: results from the FinHER trial. Ann Oncol. 2014; 25: 1544-1550.
4. Adams S, Gray RJ, Demaria S, Goldstein L, Perez EA, Shulman LN, Martino S, Wang M, Jones VE, Saphner TJ, Wolff AC, Wood WC, Davidson NE, et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J Clin Oncol. 2014; 32: 2959-2966.
5. Ono M, Tsuda H, Shimizu C, Yamamoto S, Shibata T, Yamamoto H, Hirata T, Yonemori K, Ando M, Tamura K, Katsumata N, Kinoshita T, Takiguchi Y, et al. Tumor-infiltrating lymphocytes are correlated with response to neoadjuvant chemotherapy in triple-negative breast cancer. Breast Cancer Res Treat. 2012; 132: 793-805.
6. Yamaguchi R, Tanaka M, Yano A, Tse GM, Yamaguchi M, Koura K, Kanomata N, Kawaguchi A, Akiba J, Naito Y, Ohshima K, Yano H. Tumor-infiltrating lymphocytes are important pathologic predictors for neoadjuvant chemotherapy in patients with breast cancer. Hum Pathol. 2012; 43: 1688-1694.
7. Denkert C, von Minckwitz G, Brase JC, Sinn BV, Gade S, Kronenwett R, Pfitzner BM, Salat C, Loi S, Schmitt WD, Schem C, Fisch K, Darb-Esfahani S, et al. Tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2-positive and triple-negative primary breast cancers. J Clin Oncol. 2015; 33: 983-991.
8. Pruneri G, Vingiani A, Bagnardi V, Rotmensz N, De Rose A, Palazzo A, Colleoni AM, Goldhirsch A, Viale G. Clinical validity of tumor-infiltrating lymphocytes analysis in patients with triple-negative breast cancer. Ann Oncol. 2016; 27: 249-256.
9. Topalian SL, Drake CG and Pardoll DM. Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell. 2015; 27: 450-461.
10. Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, Tykodi SS, Sosman JA, Procopio G, Plimack ER, Castellano D, Choueiri TK, Gurney H, et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med. 2015; 373: 1803-1813.
11. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012; 366: 2443-2454.
12. Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, Cruz C, Bellmunt J, Burris HA, Petrylak DP, Teng SL, Shen X, Boyd Z, Hegde PS, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014; 515: 558-562.
13. Herbst RS, Soria JC, Kowanetz M, Fine GD, Hamid O, Gordon MS, Sosman JA, McDermott DF, Powderly JD, Gettinger SN, Kohrt HE, Horn L, Lawrence DP, et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature. 2014; 515: 563-567.
14. Mittendorf EA, Philips AV, Meric-Bernstam F, Qiao N, Wu Y, Harrington S, Su X, Wang Y, Gonzalez-Angulo AM, Akcakanat A, Chawla A, Curran M, Hwu P, et al. PD-L1 expression in triple-negative breast cancer. Cancer Immunol Res. 2014; 2: 361-370.
15. Wimberly H, Brown JR, Schalper K, Haack H, Silver MR, Nixon C, Bossuyt V, Pusztai L, Lannin DR, Rimm DL. PD-L1 Expression Correlates with Tumor-Infiltrating Lymphocytes and Response to Neoadjuvant Chemotherapy in Breast Cancer. Cancer Immunol Res. 2015; 3: 326-332.
16. Schalper KA, Velcheti V, Carvajal D, Wimberly H, Brown J, Pusztai L, Rimm DL.
17. Sabatier R, Finetti P, Mamessier E, Adelaide J, Chaffanet M, Ali HR, Viens P, Caldas C, Birnbaum D, Bertucci F. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget. 2014; 6: 5449-5464. doi: 10.18632/oncotarget.3216.
18. Ali HR, Glont SE, Blows FM, Provenzano E, Dawson SJ, Liu B, Hiller L, Dunn J, Poole CJ, Bowden S, Earl HM, Pharoah PD, Caldas C. PD-L1 protein expression in breast cancer is rare, enriched in basal-like tumours and associated with infiltrating lymphocytes. Ann Oncol. 2015; 26: 1488-1493.
19. Li Z, Dong P, Ren M, Song Y, Qian X, Yang Y, Li S, Zhang X, Liu F. PD-L1 Expression Is Associated with Tumor FOXP3(+) Regulatory T-Cell Infiltration of Breast Cancer and Poor Prognosis of Patient. J Cancer. 2016; 7: 784-793.
20. Qin T, Zeng YD, Qin G, Xu F, Lu JB, Fang WF, Xue C, Zhan JH, Zhang XK, Zheng QF, Peng RJ, Yuan ZY, Zhang L, et al. High PD-L1 expression was associated with poor prognosis in 870 Chinese patients with breast cancer. Oncotarget 2015;6:33972-33981. doi: 10.18632/oncotarget.5583.
21. Muenst S, Schaerli AR, Gao F, Daster S, Trella E, Droeser RA, Muraro MG, Zajac P, Zanetti R, Gillanders WE, Weber WP, Soysal SD. Expression of programmed death ligand 1 (PD-L1) is associated with poor prognosis in human breast cancer. Breast Cancer Res Treat. 2014; 146: 15-24.
22. Baptista MZ, Sarian LO, Derchain SF, Pinto GA, Vassallo J. Prognostic significance of PD-L1 and PD-L2 in breast cancer. Hum Pathol. 2016; 47: 78-84.
23. Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, Wienert S, Van den Eynden G, Baehner FL, Penault-Llorca F, Perez EA, Thompson EA, Symmans WF, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann Oncol. 2015; 26: 259-271.
24. Swisher SK, Wu Y, Castaneda CA, Lyons GR, Yang F, Tapia C, Wang X, Casavilca SA, Bassett R, Castillo M, Sahin A, Mittendorf EA. Interobserver Agreement Between Pathologists Assessing Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer Using Methodology Proposed by the International TILs Working Group. Ann Surg Oncol. 2016; 23: 2242-2248.
25. Park IH, Kong SY, Ro JY, Kwon Y, Kang JH, Mo HJ, Jung SY, Lee S, Lee KS, Kang HS, Lee E, Joo J, Ro J. Prognostic Implications of Tumor-Infiltrating Lymphocytes in Association With Programmed Death Ligand 1 Expression in Early-Stage Breast Cancer. Clin Breast Cancer. 2016; 16: 51-58.
26. Schalper KA. PD-L1 expression and tumor-infiltrating lymphocytes: Revisiting the antitumor immune response potential in breast cancer. Oncoimmunology. 2014; 3: e29288.
27. Webb JR, Milne K, Kroeger DR, Nelson BH. PD-L1 expression is associated with tumor-infiltrating T cells and favorable prognosis in high-grade serous ovarian cancer. Gynecologic Oncology. 2016; 141: 293-302.
28. Teng MWL, Ngiow SF, Ribas A, Smyth MJ. Classifying Cancers Based on T-cell Infiltration and PD-L1. Cancer Res. 2015; 75: 2139-2145.
29. Nanda R, Chow LQ, Dees EC, Berger R, Gupta S, Geva R, Pusztai L, Pathiraja K, Aktan G, Cheng JD, Karantza V, Buisseret L. Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study. J Clin Oncol. 2016; 34: 2460-2467.
30. Goldhirsch A, Glick JH, Gelber RD, Coates AS, Thurlimann B, Senn HJ, Panel Members. Meeting highlights: international expert consensus on the primary therapy of early breast cancer 2005. Ann Oncol. 2005; 16: 1569-1583.
31. Goldhirsch A, Wood WC, Gelber RD, Coates AS, Thurlimann B, Senn HJ, Panel Members. Progress and promise: highlights of the international expert consensus on the primary therapy of early breast cancer 2007. Ann Oncol. 2007; 18: 1133-1144.
32. Goldhirsch A, Ingle JN, Gelber RD, Coates AS, Thurlimann B, Senn HJ, Panel Members. Thresholds for therapies: highlights of the St Gallen International Expert Consensus on the primary therapy of early breast cancer 2009. Ann Oncol. 2009; 20: 1319-1329.
33. Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thurlimann B, Senn HJ and Panel Members. Strategies for subtypes--dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011; 22: 1736-1747.
34. Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M, Fitzgibbons P, Hanna W, Jenkins RB, Mangu PB, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013; 31: 3997-4013.
35. Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, Dowsett M, Fitzgibbons PL, Hanna WM, Langer A, McShane LM, Paik S, Pegram MD, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007; 25: 118-145.