
INTRODUCTION
Endometriosis, a chronic gynecological disease, shares common characteristics with malignant cells [1]. Although endometriosis remains largely benign, malignant transformation may account for up to 1% of cases, most commonly from ovarian lesions [2, 3]. In addition to epidemiological evidence between endometriosis and ovarian cancer, the pathological findings confirmed endometriosis in close proximity to the tumor [4, 5]. Both ovarian clear cell and endometrioid carcinoma are associated with endometriosis [6].
The difference in prognosis between ovarian cancer patients with and without endometriosis remains elusive. Previous studies reported that ovarian cancer patients with endometriosis are associated with better prognosis compared with those without concomitant endometriosis [7-10]. However, other studies have not confirmed these findings after adjusting for potential confounding factors [11]. Resolving this issue is difficult because the criteria for the diagnosis of endometriosis associated ovarian cancer (EAOC) is heterogenous. Given these conflicting findings, we sought to characterize ovarian cancers arising from endometriosis based on pathological identification and to evaluate the prognostic impact of the endometriosis on ovarian cancer patients for risk stratification.
RESULTS
Patient characteristics and associations with endometriosis
A total of 196 patients met the inclusion criteria, of which 58 (30.0%) cases have been affected by tumors arising in endometriosis, while 138 (70.0%) had no concomitant endometriosis. Of the 58 specimens were histologically positive for ovarian cancer arising in endometriosis by H&E staining, reconfirmation of all samples by CD10 staining. CD10 IHC result was positive in each endometriosis specimens judged by H&E staining (Figure 1). CD10 staining was confined to endometrial stromal cells, and generally moderate to strong (Supplementary Table 1). Patients and tumor characteristics of the two groups are presented in Table 1. Forty-eight patients (82.76%) were clear cell histology type arising from endometriosis compared with 65.94% of clear cell ovarian cancer without endometriosis (P = 0.048). Fifty-one patients (87.93%) with endometriosis were diagnosed at the FIGO stage (I-II) compared with 66.67% of patients without endometriosis (P = 0.004). Intraperitoneal metastasis was detected in 41 patients (29.71%) in the endometriosis-free group, compared to 8 (13.79%) patients with endometriosis group (P = 0.03). Twenty-one patients (15.22%) without endometriosis tend to have more ascites compared to 1 case (1.42%) arising in endometriosis (P = 0.013). Eighty-three patients (60.14%) without endometriosis present high CA125 level, compared to 25 patients (43.1%) arising in endometriosis (P = 0.042). No association between endometriosis and other clinicopathologic characteristics was observed.
Table 1: Patient characteristics in ovarian cancer arising or not from endometriosis.
Characteristic |
Endometriosis |
P value |
|
No (n =138) |
Arising (n = 58) |
||
Age (years) |
51.08 (49.45-52.71) |
49.64(47.62-51.65) |
0.314 |
Histology Clear cell Endometrioid Mixed |
91 (65.94%) 37 (26.81%) 10 (7.25%) |
48 (82.76%) 9 (15.52%) 1 (1.72%) |
0.048 |
Ovarian involvement Monolateral Bilateral |
108 (78.26%) 30 (21.74%) |
52 (89.66%) 6 (10.34%) |
0.060 |
ECOG performance status 0-1 2-3 |
128 (92.75%) 10 (7.25%) |
55 (94.83%) 3 (5.17%) |
0.827 |
FIGO stage I II III IV |
75 (54.35%) 17 (12.32%) 40 (28.99%) 6 (4.35%) |
46 (79.31%) 5 (8.62%) 7 (12.07%) 0 (0.00%) |
< 0.001 |
FIGO stage Early stage (I/II) Late stage (III/IV) |
92 (66.67%) 46 (33.33%) |
51 (87.93%) 7 (12.07%) |
0.004 |
Lymph node metastasis negative positive |
121 (87.68%) 17 (12.32%) |
54 (93.10%) 4 (6.90%) |
0.386 |
Intraperitoneal metastasis negative positive |
97 (70.29%) 41 (29.71%) |
50 (86.21%) 8 (13.79%) |
0.030 |
Residual tumor (cm) ≤ 1 > 1 |
121 (87.68%) 17 (12.32%) |
54 (93.10%) 4 (6.90%) |
0.386 |
Preoperative ascites (ml) < 500 ≥ 500 |
117 (84.78%) 21 (15.22%) |
57 (98.28%) 1 (1.42%) |
0.013 |
Preoperative CA125 level (U/ml) < 35 ≥ 35 |
55 (39.86%) 83 (60.14%) |
33 (56.90%) 25 (43.10%) |
0.042 |
Abbreviations: ECOG, Eastern Cooperative Oncology Group; FIGO, International federation of gynecology and obstetrics; CA125, cancer antigen 125. All data presented as median (95% CI) or number. Bold values indicate P < 0.05.
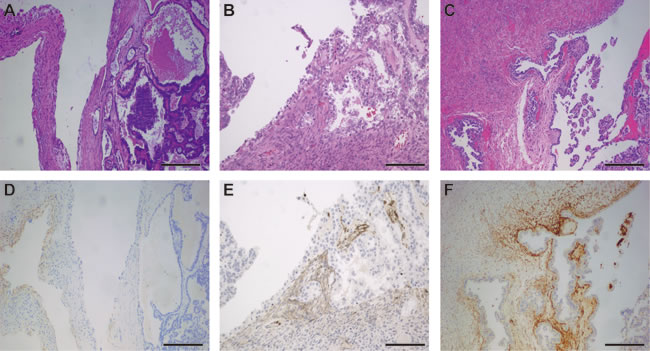
Figure 1: Representative photographs of ovarian clear cell carcinoma arising in endometriosis. A.-C. H&E staining of ovarian clear cell carcinoma arising in endometriosis. D.-F. Weak, moderate and strong immunohistochemical staining with CD10 of stroma in ovarian clear cell carcinoma specimen. Bar = 100μm.
Endometriosis is associated with PFS and OS in ovarian cancer patients
To further estimate the relationship between endometriosis and clinical outcomes of ovarian cancer patients, we applied Kaplan-Meier survival analysis and log-rank test to compare PFS and OS between two groups. As shown in Figure 2, patients with endometriosis were significantly associated with late recurrence (P < 0.001) and better OS (P < 0.001). We further performed a subgroup analysis by FIGO stage (Figure 3). The prognostic value of endometriosis is more prominent in patients with early stage (FIGO I-II) (P < 0.001 for both PFS and OS).
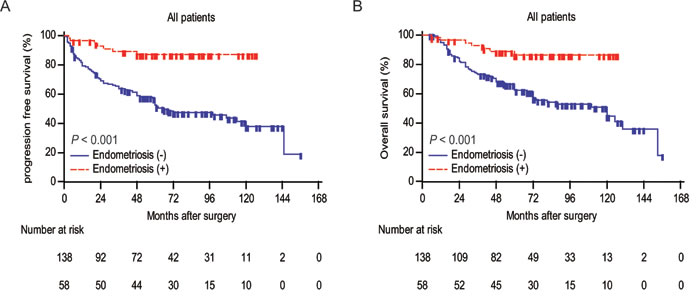
Figure 2: Analyses of progression-free survival and overall survival according to endometriosis in all patients. A.Kaplan-Meier curves for PFS of ovarian cancer patients categorized by endometriosis. Patients who were lost to follow-up or who showed no progression at the time of the last follow-up were censored (+). B. Kaplan-Meier curves for OS of ovarian cancer patients categorized by endometriosis. Patients who were lost to follow-up or who were still alive at the time of the last follow-up were censored (+). P values were calculated by log-rank test.
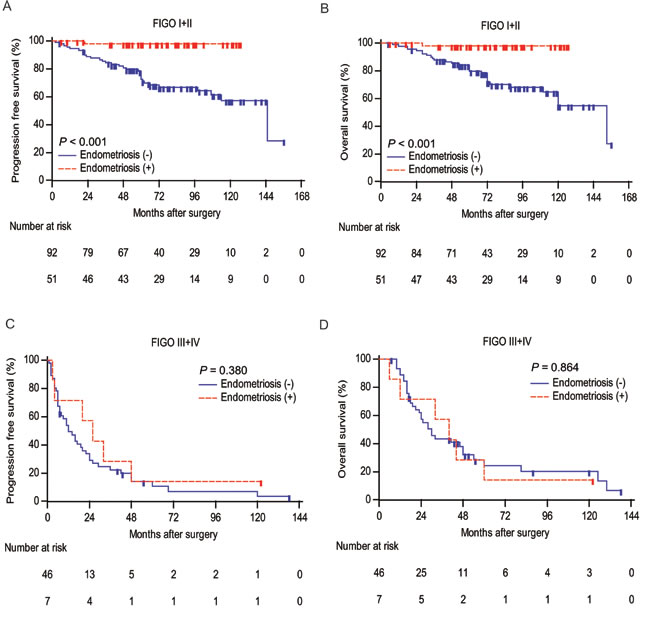
Figure 3: Analyses of progression-free survival and overall survival according to endometriosis in different FIGO stage groups. A., C. Kaplan-Meier curves for PFS of ovarian cancer patients categorized by endometriosis in FIGO stage I+II and III+IV, respectively. Patients who were lost to follow-up or who showed no progression at the time of the last follow-up were censored (+). B., D. Kaplan-Meier curves for OS of ovarian cancer patients categorized by endometriosis in FIGO stage I+II and III+IV, respectively. Patients who were lost to follow-up or who were still alive at the time of the last follow-up were censored (+). P values were calculated by log-rank test.
Endometriosis is an independent predictor of PFS and OS
To determine the prognostic significance of clinicopathologic variables of PFS and OS, we performed univariate Cox analysis. As present in Table 2, endometriosis was identified as a protective factor that might affect PFS (hazard ratio (HR) 0.187, P < 0.001) and OS (HR 0.238, P < 0.001) of ovarian cancer patients. In addition, FIGO stage, lymph node metastasis, intraperitoneal metastasis, residual tumor, ascites, and CA125 were identified as unfavorable factor for PFS and OS. On multivariate analysis, endometriosis is an independent prognostic factor for PFS (HR 0.284, P = 0.002) and OS (HR 0.349, P = 0.009).
Table 2: Univariate and multivariate Cox regression analysis for progression-free survival (PFS) and overall survival (OS) of ovarian cancer patients according to various clinic-pathologic factors (n = 196).
Clinical variables |
PFS |
OS |
||
HR (95%CI) |
P value |
HR (95%CI) |
P value |
|
Univariate analysis |
||||
Age |
0.999 (0.975-1.023) |
0.915 |
1.003 (0.977-1.030) |
0.814 |
Histology clear cell Endometrioid Mixed |
Reference 0.967 (0.585-1.671) 1.896 (0.903-3.982) |
0.286 |
Reference 0.910 (0.514-1.611) 1.845 (0.867-3.926) |
0.282 |
ECOG performance 0-1 2-3 |
Reference 1.895 (0.913-3.932) |
0.088 |
Reference 1.567 (0.678-3.621) |
0.296 |
FIGO stage Early stage (I-II) Late stage (III-IV) |
Reference 10.367 (6.460-16.638) |
<0.001 |
Reference 7.413 (4.526-12.139) |
<0.001 |
Lymph node metastasis negative positive |
Reference 4.707 (2.786-7.952) |
<0.001 |
Reference 3.048 (1.684-5.517) |
<0.001 |
Intraperitoneal metastasis negative positive |
Reference 6.182 (3.908-9.778) |
<0.001 |
Reference 5.194 (3.213-8.398) |
<0.001 |
Residual tumor (cm) ≤ 1 > 1 |
Reference 5.639 (3.375-9.423) |
<0.001 |
Reference 4.556 (2.651-7.831) |
<0.001 |
Preoperative ascites (ml) < 500 ≥ 500 |
Reference 2.914 (1.682-5.047) |
<0.001 |
Reference 2.653 (1.473-4.779) |
0.001 |
Preoperative CA125 (U/ml) < 35 ≥ 35 |
Reference 2.524 (1.561-4.079) |
<0.001 |
Reference 2.570 (1.536-4.301) |
<0.001 |
Endometriosis negative positive |
Reference 0.187 (0.086-0.405) |
<0.001 |
Reference 0.238 (0.109-0.518) |
<0.001 |
Multivariate analysis |
||||
FIGO stage Early stage (I-II) Late stage (III-IV) |
Reference 8.642 (5.339-13.988) |
<0.001 |
Reference 6.158(3.732-10.163) |
<0.001 |
Preoperative CA125 (U/ml) < 35 ≥ 35 |
Reference 2.033 (1.249-3.309) |
0.003 |
Reference 2.150 (1.275-3.626) |
0.010 |
Endometriosis negative positive |
Reference 0.284 (0.130-0.623) |
0.002 |
Reference 0.349 (0.159-0.765) |
0.009 |
Abbreviations: ECOG, Eastern Cooperative Oncology Group; FIGO, International federation of gynecology and obstetrics; CA125, cancer antigen 125; HR, hazard ratio; 95% CI, 95% confidence interval.
Bold values indicate P < 0.05.
Association between endometriosis and clinical outcomes in early stage patients
To evaluate the clinical usefulness of endometriosis in early stage ovarian cancer, we performed subgroup analysis upon early stage patients. By univariate analysis, intraperitoneal metastasis (P < 0.001 for both PFS and OS) and residual tumor (P = 0.027, P = 0.021 for PFS and OS, respectively) were significantly associated with poor clinical outcomes, while endometriosis (P = 0.004, P = 0.007 for PFS and OS, respectively) was significantly associated with better prognosis (Table 3). Multivariate analysis showed that endometriosis remained as an independent indicator of PFS (HR 0.054, P = 0.004) and OS (HR 0.064, P = 0.007).
Table 3: Univariate and multivariate Cox regression analysis for progression-free survival (PFS) and overall survival (OS) of ovarian cancer patients with FIGO stage (I/II) according to various clinic-pathologic factors (n=143).
Clinical variables |
PFS |
OS |
||
HR (95%CI) |
P value |
HR (95%CI) |
P value |
|
Univariate analysis |
||||
Age |
1.009 (0.971-1.049) |
0.643 |
1.024 (0.982-1.067) |
0.273 |
Histology clear cell Endometrioid Mixed |
Reference 1.525 (0.701-3.317) 3.891 (1.315-11.511) |
0.085 0.290 0.015 |
Reference 1.252 (0.538-2.915) 3.577 (1.202-10.646) |
0.136 0.604 0.023 |
ECOG performance 0-1 2-3 |
Reference 2.370 (0.828-6.785) |
0.110 |
Reference 1.222 (0.290-5.154) |
0.786 |
Intraperitoneal metastasis negative positive |
Reference 4.938 (2.171-11.234) |
<0.001 |
Reference 4.710 (1.960-11.320) |
<0.001 |
Residual tumor (cm) ≤ 1 > 1 |
Reference 5.092 (1.215-21.341) |
0.027 |
Reference 5.494 (1.301-23.196) |
0.021 |
Preoperative ascites (ml) < 500 ≥ 500 |
Reference 1.942 (0.681-5.538) |
0.217 |
Reference 1.480 (0.448-4.895) |
0.522 |
Preoperative CA125 (U/ml) < 35 ≥ 35 |
Reference 1.813 (0.890-3.694) |
0.103 |
Reference 1.825 (0.864-3.853) |
0.117 |
Endometriosis negative positive |
Reference 0.054 (0.007-0.395) |
0.004 |
Reference 0.062 (0.009-0.455) |
0.007 |
Multivariate analysis |
||||
Intraperitoneal metastasis negative positive |
Reference 5.049 (2.213-11.517) |
<0.001 |
Reference 4.566 (1.899-10.976) |
<0.001 |
Endometriosis negative positive |
Reference 0.054 (0.007-0.391) |
0.004 |
Reference 0.064 (0.009-0.462) |
0.007 |
Abbreviations: ECOG, Eastern Cooperative Oncology Group; FIGO, International federation of gynecology and obstetrics; CA125, cancer antigen 125; HR, hazard ratio; 95% CI, 95% confidence interval.
Bold values indicate P < 0.05.
Construction and validation of prognostic nomogram for PFS and OS
Significant prognostic factors were concluded from multivariate Cox regression analysis of PFS and OS to establish nomogram (Figure 4). The nomogram illustrated FIGO stage as sharing the largest contribution to prognosis, followed by endometriosis and CA125. The calibration plot for the nomogram presented an optimal agreement between the predicted and actual observation for the PFS and OS at 5-year (Figure 5).
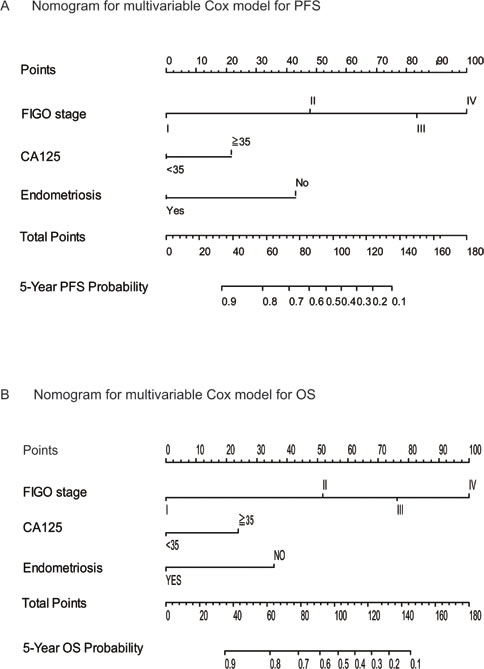
Figure 4: Survival nonograms. Nomograms were created from the multivariable Cox model. The presence or absence of each variable is scored (top row). The cumulative score from each variable is used to calculate 5-year PFS A. and OS B. probabilities. PFS = progression-free survival. OS = overall survival.
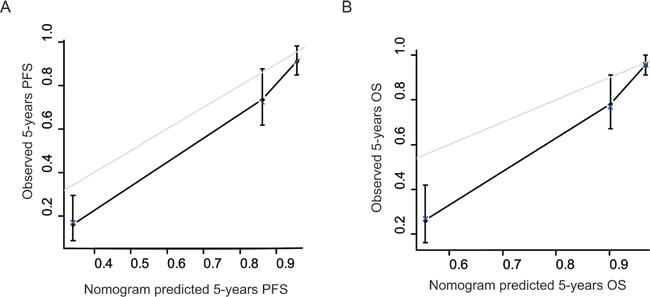
Figure 5: The calibration curves for predicting patient survival at each time point. Nomogram-predicted 5-year PFS A. and 5-year OS B. is plotted on the x-axis; actual PFS and OS is plotted on the y-axis. A plot along the 45-degree line would indicate a perfect calibration model in which the predicted probabilities are identical to the actual outcomes.
DISCUSSION
Our study reported endometriosis as an independent predictor for PFS and OS in patients with ovarian cancer. Moreover, endometriosis manifests a discriminative power in early stage ovarian cancer subgroups, which can help guiding management of patients with early FIGO stage. The nomogram integrating endometriosis, FIGO stage and CA125 predicts 5-year PFS and OS well for ovarian cancer patients.
Ryu et al. explored most of the patients had diagnosed at an early stage (stage I, 61.3%), and the overall 5-year survival rate was 57% [12]. Consistently, in our cohort, 121 (61.7%) out of all patients was diagnosed at FIGO stage I, and the overall 5-year survival rate was 69.5%. Moreover, we found that the overall 5-year survival rate was 91.5% in stage I, 56.3% in stage II, 26.4% in stage III, and 0% in stage IV (Supplementary Figure 1), which is quite consistent with data from the United states [13]. However, our study demonstrated that patients of ovarian cancer arising from endometriosis had a better prognosis, with 86.6% 5-year survival compared with 62.4% in patients of ovarian cancer without endometriosis, which was consistent with Shuang et al. [14].
The criteria for the definition of endometriosis associated ovarian cancer varied between different studies. Some authors considered the tumors as EAOC on the basis of malignant transformation in the endometriosis glands leading to carcinoma [10], whereas others included cases if either the transition point was identified or merely in the setting of any endometriosis was found within the surgical specimen coexisting with cancer [15]. We adopted the strictly histologic criteria for the diagnosis of ovarian cancer arising in endometriosis [16]. Additionally, the use of CD10 immunohistochemistry confirmed the diagnoses of ovarian cancer arising from endometriosis [17].
In our data, when FIGO stage was controlled, endometriosis remains significant on multivariate analysis between subjects and controls. This supports the hypothesis that EAOC as a distinct disease from non-EAOC with better prognosis [18]. ARID1A (AT-rich interactive domain 1A) mutations and consequent loss of BAF250a (BRG-associated factor 250a) protein expression were particularly identified in EAOC, and in the contiguous atypical endometriotic lesions, but not in distinct endometrioid lesions far from the carcinoma, suggesting such phenomenon as a possible early event in the malignant transformation of endometriosis [19, 20]. ARID1A mutations induce chromatin remodeling dysfunction and tend to coexist with activating PIK3CA mutations [21]. Moreover, atypical endometriosis and EAOC may share several molecular alterations such as ARID1A and PIK3CA mutations, PTEN loss, MET amplifications, and HNF1B overexpression, suggesting a common molecular mechanism for malignant development [22-24]. In an Apc- and Pten-defective mouse ovarian cancer model loss of ARID1A enhances epithelial differentiation and prolongs survival, which may account for the better prognosis of ovarian cancer arising in endometriosis [25]. The clinical significance of loss of ARID1A in EAOC has remained to be elucidated.
Our data are consistent with that of Shuang et al [14], who reported that 78.5% of clear cell cancer associated with endometriosis presented as stage I and II compared with 37.4% of clear cell ovarian cancers that are not associated with endometriosis. With regard to endometriosis as independent predictor for prognosis, there was a discrepancy between the study of Shuang et al [14] and our own. Resolving this issue only be these two studies is difficult because the number of patients in both studies was insufficient. Potential limitation of this analysis should be considered. This is a retrospective analysis, and data were obtained by clinical records; thus, only hard information, such as age and stage of the disease, were collected.
In conclusion, our study revealed that endometriosis is associated with better clinical outcomes in ovarian cancer patients. A prognostic model integrating endometriosis, FIGO stage and CA125 may improve the management of ovarian cancer patients in terms of risk stratification, individualizing postsurgical follow-up.
MATERIALS AND METHODS
Patients
After approval from institutional review board, we retrospectively identified 196 cases with a primary diagnosis of pure clear cell, endometrioid, or mixed ovarian cancer at our hospital between 1995 and 2010. Of the mixed tumors, 8 cases showed clear cell histology with endometrioid histology, whereas the remaining tumors showed heterogeneous histology consisting of endometrioid, clear cell, and serous differentiation. All patients underwent surgery according to Federation of Gynecology and Obstetrics (FIGO) guidelines for ovarian cancer. All patients received a platinum-based chemotherapy regimen, and the number of cycles ranged from six to nine after tailoring to different individuals. Microscopic slides were reviewed and confirmed by two experienced gynecologic pathologist (Dr. XT and JZ). Patients were divided into two groups according to the detection of cancer arising from ovarian endometriosis or not on the basis of the Sampson and Scott criteria: 1) the presence of both benign and neoplastic endometrial tissues in the tumor, 2) histological findings compatible with an endometrial origin, 3) the discovery of no other primary tumor sites, and 4) a morphologic demonstration of a continuum between benign and malignant epithelium [10]. Patients with the pathological findings confirmed endometriosis in close proximity to the tumor, but not histologically contiguous to the ovarian cancer tissue were excluded. The inclusion and exclusion criteria were summarized in Supplementary Figure 2. No statistically significant differences in tumor characteristics or survival outcomes were observed for included and excluded patients (Supplementary Table 2 and Supplementary Figure 3).
Immunohistochemistry
The primary formalin-fixed, paraffin-embedded ovarian cancer tissues arising from endometriosis were applied with CD10 immunohistochemical staining. Immunohistochemistry protocol was described previously [26]. The primary antibody against human CD10 (clone 56C6, DAKO; dilution: 1: 200) was applied in the procedure. Positive staining was subjectively classified as weak, moderate, or strong.
Statistical analysis
Correlations between endometriosis and clinicopathologic characteristics were analyzed with χ2 test. Clinical outcomes were assessed by progression free survival (PFS) and overall survival (OS). PFS was defined as the interval between the date of surgery and the date of diagnosis of any type of progression. OS was defined as the interval between surgery and death. Patients were censored if they were lost to follow-up or if they show not progression or were still alive at the time of last follow-up. Follow up was updated in Feb 2015. Kaplan-Meier method with log-rank test was applied to compare survival curves. Univariate and multivariate Cox regression models were fitted to evaluate the effect of prognostic factors on OS and PFS, and P > 0.10 was the removal criterion when performing backward stepwise variable deletions. Nomogram was constructed as the prognostic model whose accuracy was evaluated by the Calibration plot. Data were analyzed using MedCalc software (version 12.7.0.0; MedCalc, Mariakerke, Belgium), and R software, version 3.1.2 (The R Foundation for Statistical Computing, http://www.r-project.org). All statistical tests were two sided and performed at a significance level of 0.05.
CONFLICTS OF INTEREST
The authors declare no competing interests.
GRANT SUPPORT
This study was supported by grants from National Natural Science Foundation of China (31570803, 81272879, 81402151), Research Program of Shanghai Municipal Commission of Health and Family Planning (20154Y0049).
REFERENCES
1. Jayson GC, Kohn EC, Kitchener HC and Ledermann JA. Ovarian cancer. Lancet. 2014; 384(9951):1376-1388.
2. Giudice LC. Clinical practice. Endometriosis. The New England journal of medicine. 2010; 362(25):2389-2398.
3. Brown J and Farquhar C. Endometriosis: an overview of Cochrane Reviews. The Cochrane database of systematic reviews. 2014; 3:CD009590.
4. Stewart LM, Holman CD, Aboagye-Sarfo P, Finn JC, Preen DB and Hart R. In vitro fertilization, endometriosis, nulliparity and ovarian cancer risk. Gynecologic oncology. 2013; 128(2):260-264.
5. Buis CC, van Leeuwen FE, Mooij TM and Burger CW. Increased risk for ovarian cancer and borderline ovarian tumours in subfertile women with endometriosis. Hum Reprod. 2013; 28(12):3358-3369.
6. Pearce CL, Templeman C, Rossing MA, Lee A, Near AM, Webb PM, Nagle CM, Doherty JA, Cushing-Haugen KL, Wicklund KG, Chang-Claude J, Hein R, Lurie G, Wilkens LR, Carney ME, Goodman MT, et al. Association between endometriosis and risk of histological subtypes of ovarian cancer: a pooled analysis of case-control studies. The Lancet Oncology. 2012; 13(4):385-394.
7. Deligdisch L, Penault-Llorca F, Schlosshauer P, Altchek A, Peiretti M and Nezhat F. Stage I ovarian carcinoma: different clinical pathologic patterns. Fertility and sterility. 2007; 88(4):906-910.
8. Melin A, Lundholm C, Malki N, Swahn ML, Sparen P and Bergqvist A. Endometriosis as a prognostic factor for cancer survival. International journal of cancer. 2011; 129(4):948-955.
9. Wang S, Qiu L, Lang JH, Shen K, Huang HF, Pan LY, Wu M, Yang JX and Guo LN. Prognostic analysis of endometrioid epithelial ovarian cancer with or without endometriosis: a 12-year cohort study of Chinese patients. American journal of obstetrics and gynecology. 2013; 209(3):241 e241-249.
10. Kumar S, Munkarah A, Arabi H, Bandyopadhyay S, Semaan A, Hayek K, Garg G, Morris R and Ali-Fehmi R. Prognostic analysis of ovarian cancer associated with endometriosis. American journal of obstetrics and gynecology. 2011; 204(1):63 e61-67.
11. Davis M, Rauh-Hain JA, Andrade C, Boruta DM, 2nd, Schorge JO, Horowitz NS, May T and del Carmen MG. Comparison of clinical outcomes of patients with clear cell and endometrioid ovarian cancer associated with endometriosis to papillary serous carcinoma of the ovary. Gynecologic oncology. 2014; 132(3):760-766.
12. Ryu SY, Park SI, Nam BH, Kim I, Yoo CW, Nam JH, Lee KH, Cho CH, Kim JH, Park SY, Kim BG and Kang SB. Prognostic significance of histological grade in clear-cell carcinoma of the ovary: a retrospective study of Korean Gynecologic Oncology Group. Annals of oncology. 2009; 20(6):1032-1036.
13. Chan JK, Teoh D, Hu JM, Shin JY, Osann K and Kapp DS. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers. Gynecologic oncology. 2008; 109(3):370-376.
14. Ye S, Yang J, You Y, Cao D, Bai H, Lang J, Chen J and Shen K. Comparative study of ovarian clear cell carcinoma with and without endometriosis in People’s Republic of China. Fertility and sterility. 2014; 102(6):1656-1662.
15. Orezzoli JP, Russell AH, Oliva E, Del Carmen MG, Eichhorn J and Fuller AF. Prognostic implication of endometriosis in clear cell carcinoma of the ovary. Gynecologic oncology. 2008; 110(3):336-344.
16. Scarfone G, Bergamini A, Noli S, Villa A, Cipriani S, Taccagni G, Vigano P, Candiani M, Parazzini F and Mangili G. Characteristics of clear cell ovarian cancer arising from endometriosis: a two center cohort study. Gynecologic oncology. 2014; 133(3):480-484.
17. Agarwal N and Subramanian A. Endometriosis - morphology, clinical presentations and molecular pathology. Journal of laboratory physicians. 2010; 2(1):1-9.
18. Erzen M, Rakar S, Klancnik B and Syrjanen K. Endometriosis-associated ovarian carcinoma (EAOC): an entity distinct from other ovarian carcinomas as suggested by a nested case-control study. Gynecologic oncology. 2001; 83(1):100-108.
19. Wiegand KC, Shah SP, Al-Agha OM, Zhao Y, Tse K, Zeng T, Senz J, McConechy MK, Anglesio MS, Kalloger SE, Yang W, Heravi-Moussavi A, Giuliany R, Chow C, Fee J, Zayed A, et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. The New England journal of medicine. 2010; 363(16):1532-1543.
20. Maeda D, Mao TL, Fukayama M, Nakagawa S, Yano T, Taketani Y and Shih Ie M. Clinicopathological significance of loss of ARID1A immunoreactivity in ovarian clear cell carcinoma. International journal of molecular sciences. 2010; 11(12):5120-5128.
21. Jones S, Wang TL, Shih Ie M, Mao TL, Nakayama K, Roden R, Glas R, Slamon D, Diaz LA, Jr., Vogelstein B, Kinzler KW, Velculescu VE and Papadopoulos N. Frequent mutations of chromatin remodeling gene ARID1A in ovarian clear cell carcinoma. Science. 2010; 330(6001):228-231.
22. Sato N, Tsunoda H, Nishida M, Morishita Y, Takimoto Y, Kubo T and Noguchi M. Loss of heterozygosity on 10q23.3 and mutation of the tumor suppressor gene PTEN in benign endometrial cyst of the ovary: possible sequence progression from benign endometrial cyst to endometrioid carcinoma and clear cell carcinoma of the ovary. Cancer research. 2000; 60(24):7052-7056.
23. Gadducci A, Lanfredini N and Tana R. Novel insights on the malignant transformation of endometriosis into ovarian carcinoma. Gynecological endocrinology. 2014; 30(9):612-617.
24. Yamashita Y. Ovarian cancer: new developments in clear cell carcinoma and hopes for targeted therapy. Japanese journal of clinical oncology. 2015; 45(5):405-407.
25. Zhai Y, Kuick R, Tipton C, Wu R, Sessine M, Wang Z, Baker SJ, Fearon ER and Cho KR. Arid1a inactivation in an Apc- and Pten-defective mouse ovarian cancer model enhances epithelial differentiation and prolongs survival. The Journal of pathology. 2016; 238(1):21-30.
26. Potlog-Nahari C, Feldman AL, Stratton P, Koziol DE, Segars J, Merino MJ and Nieman LK. CD10 immunohistochemical staining enhances the histological detection of endometriosis. Fertility and sterility. 2004; 82(1):86-92.