
INTRODUCTION
Extra-nodal natural-killer (NK)/T-cell lymphoma is a subtype of the mature T- and NK-cell neoplasm in the World Health Organization (WHO) classification [1]. It is common in Asia compared with Western countries: 3-9% of lymphoma versus 1% in Western countries [2-4]. NK/T-cell lymphoma is an aggressive lymphoma with 5-year survival <50 percent [5-8].
Several prognostic models have been studied for NK/T-cell lymphoma including the International Prognostic Index [IPI], the Korean Prognostic Index [KPI], the Prognostic Index for T-cell lymphoma, a new model combining the KPI, total protein and fasting blood glucose [8, 9] and a model using data from PET/CT parameters including the maximum standardized uptake value [SUVmax], whole-body metabolic tumour volume [WBMTV] and whole body total lesion glycolysis [WBTLG]) [10-12]. Recently, Kim et al. reported combining post-treatment Deauville score on PET/CT with data on Epstein-Barr virus (EBV) DNA predicts treatment-failure in subjects with nasal NK/T-cell lymphoma [13]. Most of these models were tested in persons with early and/or nasal NK/T-cell lymphoma.
Predictive value of SUVmax [10-12] is controversial probably because it measures maximum metabolic rate of some but not all lymphoma sites. In a small study, Kim et al. [10] suggested WBMTV and WBTLG might be better survival predictors than SUVmax but these data need confirmation. The SUVmax considers only one voxel. We hypothesized the sum of the SUVmax of all the nodal and extra-nodal tumours measured by 18F-FDG PET/CT would better represent lymphoma activity in a person with NK/T-cell lymphoma. To test this hypothesis, we designed three new models on the basis of the whole-body SUVmax of 11 nodal lesions (Waldeyer ring, neck, infra-clavicular, axillary and pectoral, mediastinal, hilar, spleen, para-aortic, mesenteric, lilac, inguinal and femoral) and 10 extra-nodal lesions (upper aero-digestive tract, skin/subcutaneous tissues, central nervous system [CNS] and spinal canal, lung, myocardium, bone and bone marrow, bowel, renal and adrenal, liver and testis). We tested these models in receiver-operator characteristic (ROC) curve analyses to determine which best predicted progression-free survival (PFS) and overall survival (OS) in training (N= 54) and validation (N=15) cohorts.
RESULTS
Clinical variables
Clinical variables are outlined in Table 1. Thirty-seven subjects were male. Median age was 46 years (range, 14-85 years). Twenty-seven were Ann Arbor stage-I/II and 20 of whom had extra-nasal cavity type lymphoma. Twenty-six subjects had an elevated serum lactate dehydrogenase (LDH) level and 23 had B-symptoms. Nine subjects had an ECOG score ≥2 and 31 had an IPI score ≥2.
Table 1: Subject variables (N=54)
Clinical characteristics |
N (%) |
|---|---|
Male |
37 (69%) |
Age ≤60 years |
42 (78%) |
LDH ≤ULN |
26 (48%) |
Ann Arbor stage I/II |
27 (50%) |
Presence of B symptom |
23 (43%) |
ECOG 2-4 |
9 (17%) |
Extra-nodal sites ≤1 |
32 (59%) |
IPI score 0-1 |
23 (43%) |
Values of SUVmax, WB1SUVmax, WB2SUVmax and WB3SUVmax in different groups
Upper aero-digestive tract involvement was present in 41 subjects with median SUVmax of 12.9 (range, 4.5-25.9). Bone and bone marrow involvement were present in 14 subjects with the median SUVmax of 8.0 (range, 2.7-13.5). SUVmax of the other 7 extra-nodal sites were all <20 percent (Table 2).
Table 2: Distribution of extra-nodal site involvement
N |
SUVmax (range) |
|
|---|---|---|
Upper aero-digestive tract |
41 (76%) |
12.9 (4.5-25.9) |
Skin/subcutaneous tissues |
7 (13%) |
8.5 (2.7-17.1) |
Central nervous system and spinal canal |
2 |
8.6 (7.3-10.2) |
Lung |
8 (15%) |
5.3 (1.6-9.3) |
Myocardium |
2 |
10.3 (2.4-18.1) |
Bone and bone marrow |
14 (26%) |
8.0 (2.7-13.5) |
Bowel |
7 (13%) |
9.7 (4.0-25.1) |
Renal and adrenal |
5 |
11.1 (7.1-15.8) |
Liver |
4 |
6.4 (2.1-9.0) |
Testis |
5 (9%) |
8.3 (5.3-15.9) |
Median value of WB1SUVmax, WB2SUVmax and WB3SUVmax at diagnosis in the disease progression cohort (N=29) were higher than those in the progression-free group (N=25; P<0.0001, P=0.002 and P<0.001). There were no significant difference in SUVmax (P=0.141). Similarly, median value of WB1SUVmax, WB2SUVmax and WB3SUVmax at diagnosis in living subjects (N=30) were significantly higher than values in dead subjects (N=24; P<0.001, P=0.001 and P<0.001). The difference in SUVmax was borderline (P=0.072; Table 3).
Table 3: Median values of SUVmax, WB1SUVmax, WB2SUVmax and WB3SUVmax in different sub-groups.
PD |
≥SD |
P |
Alive |
Dead |
P |
|
|---|---|---|---|---|---|---|
SUVmax |
14.0 (3.9-25.9) |
11.8 (4.5-23.6) |
0.141 |
14.6 (3.9-25.9) |
11.9 (4.5-23.6) |
0.072 |
WB1SUVmax |
38.8 (3.9-109.0) |
17.3 (4.5-54.7) |
<0.001 |
42.0 (3.9-109.0) |
19.7 (4.5-65.6) |
<0.001 |
WB2SUVmax |
33.6 (3.9-99.2) |
17.4 (4.5-58.0) |
0.002 |
36.1 (3.9-99.2) |
19.2 (4.5-65.6) |
0.001 |
WB3SUVmax |
34.5 (3.9-109.0) |
17.1 (4.5-54.7) |
<0.001 |
36.7 (3.9-109.0) |
19.4 (4.5-65.6) |
<0.001 |
Comparison of the models
We evaluated the predictive accuracy of these models in time-dependent ROC curves which showed optimal cut-off values for SUVmax, WB1SUVmax, WB2SUVmax and WB3SUVmax of 12.0 (sensitivity 71%; specificity 60%; AUC (areas under the curve) 0.653; P=0.05), 15.8 (sensitivity 92%; specificity 67%; AUC 0.811; P<0.001), 12.7 (sensitivity 96%; specificity 57%; AUC 0.785; P<0.001) and 15.8 (sensitivity 88%; specificity 70%; AUC 0.793; P<0.001; Figure 1). If we consider OS for the entire follow-up period, the AUCs of SUVmax, WB1SUVmax, WB2SUVmax and WB3SUVmax were 0.653 [0.511, 777], 0.811 [0.681, 0.905], 0.785 [0.653, 0.885] and 0.793 [0.661, 0.891]. Pair-wise comparisons of ROC curves in the models are shown in Supplementary Table S1. Significant improvement in discrimination for WB1SUVmax, WB2SUVmax and WB3SUVmax compared with SUVmax was observed. There were no significant differences between WB1SUVmax, WB2SUVmax and WB3SUVmax and we selected WB3SUVmax which is the simplest of the 3 models to compute for further analyses. Kaplan-Meier PFS and OS cures for the WB3SUVmax model using the optimal cut-off value are shown in Figure 2.
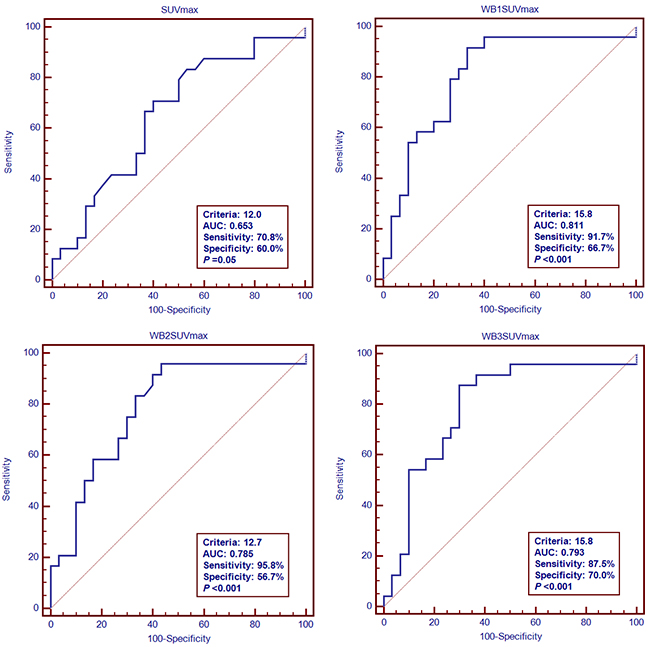
Figure 1: ROC curve analyses of OS.
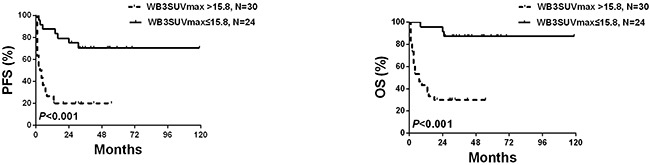
Figure 2: PFS and OS according to WB3SUVmax.
Parameters (sex, age, Ann Arbor stage, LDH level, B-symptom, extra-nodal involvement sites, ECOG score, IPI score and WB3SUVmax) significantly associated with PFS and OS were entered into multivariate analyses. WB3SUVmax >15.8 was significantly associated with PFS (HR 3.67 [1.19, 11.29]; P=0.023) and OS (HR 4.51 [1.02-19.91]; P=0.047; Table 4).
Table 4: Uni- and multivariate Cox regression analyses for PFS and OS
Univariate (PFS) |
Multivariate (PFS) |
Univariate (OS) |
Multivariate (OS) |
|||||
|---|---|---|---|---|---|---|---|---|
Characteristic |
HR (95%CI) |
P |
HR (95%CI) |
P |
HR (95%CI) |
P |
HR (95%CI) |
P |
WB3SUVmax>15.8 |
5.23 (2.20-12.40) |
<0.001 |
3.67 (1.19-11.29) |
0.023 |
9.66 (2.85-32.76) |
<0.001 |
4.51 (1.02-19.91) |
0.047 |
IPI≥2 |
7.37 (2.78-19.51) |
<0.001 |
-- |
-- |
13.81 (3.22-59.21) |
<0.001 |
-- |
-- |
Age>60 years |
0.786 (0.32-1.92) |
0.596 |
-- |
-- |
0.79 (0.30-2.13) |
0.650 |
-- |
-- |
ECOG PS>1 |
2.07 (0.92-4.65) |
0.078 |
-- |
-- |
2.23 (0.88-5.64) |
0.091 |
-- |
-- |
LDH>ULN |
5.50 (2.33-12.98) |
<0.001 |
-- |
-- |
7.24 (2.46-21.38) |
<0.001 |
-- |
-- |
Stage III or IV |
4.17 (1.89-9.21) |
<0.001 |
-- |
-- |
5.62 (2.08-15.17) |
0.001 |
-- |
-- |
Extra-nodal sites>1 |
3.05 (1.48-6.32) |
0.003 |
-- |
-- |
5.63 (2.31-13.74) |
<0.001 |
-- |
-- |
Gender (male) |
0.69 (0.33-1.42) |
0.314 |
-- |
-- |
0.71 (0.31-1.63) |
0.422 |
-- |
-- |
B symptoms |
2.92 (1.30-6.56) |
0.010 |
-- |
-- |
3.74 (1.39-10.05) |
0.009 |
-- |
-- |
Validation cohort for WB3SUVmax
Data from the validation cohort confirmed the predictive value of WB3SUVmax for PFS and OS (Figure 3).
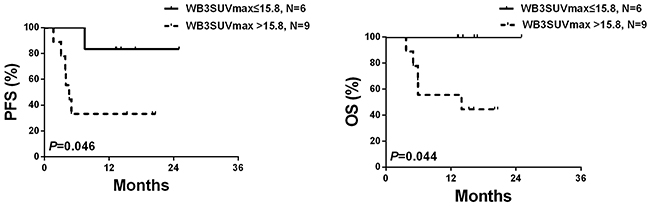
Figure 3: PFS and OS of the validation cohort (N=15) according to WB3SUVmax.
DISCUSSION
The predictive values of PET/CT parameters such as SUVmax, WBMTV and WBTLG in extra-nodal NK/T-cell lymphomas are controversial [10-12, 16-22]. One problem with using SUVmax is that the value represents only the highest metabolic rate in one lymphoma site which may not be representative of metabolic rate in several or all lymphoma sites. As such WBMTV and WBTLG may better represent the sum of lymphoma sites and metabolic activity [10, 20]. Nevertheless, the prognostic value of WBMTV and WBTLG in aggressive lymphomas is controversial [10, 20-22].
Limitations of predictive models for extra-nodal NK/T-cell lymphoma, especially the non-nasal type [2, 10-12, 15-22] led us to study three new prognostic models, WB1SUVmax, WB2SUVmax, WB3SUVmax. The models differ in how they sum SUVmax lymphoma sites but had mostly concordant values. In 40 subjects, WB1SUVmax, WB2SUVmax, WB3SUVmax were similar and in 10 others values were >15.8. We selected WB3SUVmax, because it was the simplest to compute. Although the WB3SUVmax does not represent the total volume and metabolic activity of lymphoma sites, it indicates the sum of the highest metabolic rates of all nodal and extra-nodal lesions. In conclusion, we show WB3SUVmax is a strong predictor of PFS and OS in persons with extra-nodal NK/T-cell lymphoma. Because our validation cohort was small, our conclusion should be tested in other datasets.
SUBJECTS AND METHODS
Subjects
The study was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University and done according to guidelines of Nanjing Medical University. Subjects provided informed consent in accordance with requirements of the Declaration of Helsinki. Between June, 2006 and May, 2014, 54 consecutive subjects with newly diagnosed NK/T-cell lymphoma had a 18F-FDG PET/CT scan for staging at our centre. Diagnosis was based on the World Health Organization lymphoma classification [23]. Baseline clinical variables included age, sex, Ann Arbor stage (I-IV), LDH, B-symptoms, extra-nodal disease sites and ECOG performance score. Therapy was with L/P-EMD (L/Peg-asparaginase, etoposide, methotrexate and dexamethasone; Supplementary Table S2). Subjects received a median cycle of 4 (range, 3-6). Thirty subjects also received radiation therapy to residual disease sites. Median follow-up is 45 months (range, 20-120 months).
18F-FDG PET/CT image acquisition
PET/CT studies were obtained on the following PET/CT devices: Gemini TF64 (Philips), Gemini GXL (Philips), Gemini TF16 (Philips), Discovery LS (GE Healthcare), and Biograph TP16 (Siemens). Subjects with fasting serum glucose <7.0 mmol/L >6 h received IV 18F-fluorodeoxyglucose (18F-FDG) 3.70−5.55 MBq/Kg. After 60 min whole-body PET/CT imaging was performed with a whole-body CT scan (120 KV and 140 mA) and a whole-body PET (in 3-dimensional mode, 120s/bed position). Acquisition of CT, PET and PET/CT fusion images including cross-section, sagittal-section and coronal-section used CT-based attenuation correction in reconstruction image by an iterative method.
Image analysis models
The body was divided into 11 nodal regions (Waldeyer ring, neck, infra-clavicular, axillary and pectoral, mediastinal, hilar, spleen, paraaortic, mesenteric, lilac, inguinal and femoral) and 10 extra-nodal regions (upper aero-digestive tract, skin/subcutaneous tissues, central nervous system [CNS] and spinal canal, lung, myocardium, bone and bone marrow, bowel, renal and adrenal, liver and testis) for analyses [2, 15] (Supplementary Table S3). SUVmaxs were evaluated for all subjects. Four models (SUVmax, WB1SUVmax, WB2SUVmax and WB3SUVmax) were used to calculate the whole body SUVmax of the nodal and extra-nodal regions (Table 5).
Table 5: Three different models to calculate the whole body SUVmaxs for nodal and extra-nodal regions to predict PFS and survival
Models |
Nodal and extra-nodal regions for calculation |
|---|---|
SUVmax |
Maximum standard uptake value of primary lesion |
WB1SUVmax |
Whole body SUVmax of 11 nodal and 10 extra-nodal regions |
WB2SUVmax |
Whole body SUVmax of 4 nodal* (neck, axillary, inguinal and spleen) and 10 extra-nodal regions |
WB3SUVamx |
Whole body SUVmax of 3 nodal regions (superior diaphragm, inferior diaphragm and spleen) and 10 extra-nodal regions |
*Four different nodal regions refer to chronic lymphocytic leukemia (CLL)
Validation cohort
15 subjects receiving PEMD for a median of 4 cycles (range, 2-6) constituted the validation cohort. Median follow-up from diagnosis was 16 mo (range 13- 25 mo).
Statistical analysis
We used the Epidata 3.10 to establish datasets and verify validity of data-entry twice. The discriminative ability of the model was determined using time-dependent ROC curves and the corresponding AUCs were calculated to assess the predictive accuracy of the models [24]. Differences in AUCs were tested as described [25]. Survival curves were constructed by the Kaplan-Meier method. Log-rank test was used to compare survival times of different groups categorized by the selected best predictive model. Prognostic significances of PET parameter (the best one) and clinical variables (sex, age, IPI score, Ann Arbor stage, LDH level, B-symptoms, ECOG performance and extra-nodal sites) were assessed by univariate analyses. Variables with significant associations were included in multivariate Cox proportional hazards regression analyses. All the statistical analyses used STATA statistical software (version 11.1; StataCorp, TX, USA) and R software (version 3.2.1; The R Foundation for Statistical Computing). Two-sided P≤0.05 was considered significant.
ACKNOWLEDGMENTS
Supported by National Natural Science Foundation of China (30971296, 81170485, 81170488, 81370657, 81470328, 81500125, 81522001, 81570141), Project of National Key Clinical Specialty, the National Science & Technology Pillar Program (2014BAI09B12), and a project funded by Jiangsu Provincial Special Program of Medical Science (BL2014086). RPG acknowledges support from the National Institute of Health Research (NIHR) Biomedical Research Centre funding scheme.
CONFLICT OF INTEREST
None.
REFERENCES
1. Jaffe ES. The 2008 WHO classification of lymphomas: implications for clinical practice and translational research. Hematology Am Soc Hematol Educ Program. 2009; 2009:523-531.
2. Au WY, Ma SY, Chim CS, Choy C, Loong F, Lie AK, Lam CC, Leung AY, Tse E, Yau CC, Liang R, Kwong YL. Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the World Health Organization classification scheme: a single center experience of 10 years. Ann Oncol. 2005;16:206-214.
3. Lymphoma Study Group of Japanese Pathologists. The World Health Organization classification of malignant lymphomas in Japan: incidence of recently recognized entities. Pathol Int. 2000;50:696-702.
4. Chen CY, Yao M, Tang JL, Tsay W, Wang CC, Chou WC, Su IJ, Lee FY, Liu MC, Tien HF. Chromosomal abnormalities of 200 Chinese patients with non-Hodgkin’s lymphoma in Taiwan: with special reference to T-cell lymphoma. Ann Oncol. 2004;15:1091-1096.
5. Lee J, Park YH, Kim WS, Lee SS, Ryoo BY, Yang SH, Park KW, Kang JH, Park JO, Lee SH, Kim K, Jung CW, Park YS, et al. Extranodal nasal type NK/T-cell lymphoma: Elucidating clinical prognostic factors for risk-based stratification of therapy. Eur J Cancer. 2005;41:1402-1408.
6. Chim CS, Ma SY, Au WY, Choy C, Lie AK, Liang R, Yau CC, Kwong YL. Primary nasal natural killer cell lymphoma: Long-term treatment outcome and relationship with the International Prognostic Index. Blood. 2004;103:216-221.
7. Cheung MM, Chan JK, Lau WH, Ngan RK, Foo WW. Early stage nasal NK/T-cell lymphoma: clinical outcome, prognostic factors, and the effect of treatment modality. Int J Radiat Oncol Biol Phy. 2002;54:182-190.
8. Lee J, Suh C, Park YH, Ko YH, Bang SM, Lee JH, Lee DH, Huh J, Oh SY, Kwon HC, Kim HJ, Lee SI, Kim JH, et al. Extranodal Natural Killer T-Cell Lymphoma, Nasal-Type: A Pronostic Model From a Retrospective Multicenter Study. J Clin Oncol. 2006;24:612-618.
9. Cai Q, Luo X, Zhang G, Huang H, Huang H, Lin T, Jiang W, Xia Z, Young KH. New prognostic model for extranodal natural killer/T-cell lymphoma, nasal type. Ann Hematol. 2014;93:1541-1549.
10. Kim CY, Hong CM, Kim DH, Son SH, Jeong SY, Lee SW, Lee J, Ahn BC. Prognostic value of whole-body metabolic tumour volume and total lesion glycolysis measured on 18F-FDG PET/CT in patients with extranodal NK/T-cell lymphoma. Eur J Nucl Med Mol Imaging. 2013;40:1321-1329.
11. Suh C, Kang YK, Roh JL, Kim MR, Kim JS, Huh J, Lee JH, Jang YJ, Lee BJ. Prognostic Value of Tumor 18F-FDG Uptake in Patients with Untreated Extranodal Natural Killer/T-Cell Lymphomas of the Head and Neck. J Nucl Med. 2008;49:1783-1789.
12. Jiang C, Zhang X, Jiang M, Zou L, Su M, Kosik RO, Tian R. Assessment of the prognostic capacity of pretreatment, interim, and post-therapy (18)F-FDG PET/CT in extranodal natural killer/T-cell lymphoma, nasal type. Ann Nucl Med. 2015;29:442-451.
13. Kim SJ, Choi JY, Hyun SH, Ki CS, Oh D, Ahn YC, Ko YH, Choi S, Jung SH, Khong PL, Tang T, Yan X, Lim ST, et al. Risk stratification on the basis of Deauville score on PET-CT and the presence of Epstein-Barr virus DNA after completion of primary treatment for extranodal natural killer/T-cell lymphoma, nasal type: a multicentre, retrospective analysis. Lancet Haematol. 2015;2:e66-74.
14. Suzuki R, Takeuchi K, Ohshima K, Nakamura S. Extranodal NK/T-cell lymphoma: diagnosis and treatment cues. Hematol Oncol. 2008;26:66-72.
15. Moon SH, Cho SK, Kim WS, Kim SJ, Chan Ahn Y, Choe YS, Lee KH, Kim BT, Choi JY. The role of 18F-FDG PET/CT for Initial Staging of Nasal Type Natural Killer/T-Cell Lymphoma: A Comparison with Conventional Staging Methods. J Nucl Med. 2013;54:1039-1044.
16. Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, Lister TA. Recommendations for initial evaluation, stageing, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32:3059-3068.
17. Cashen AF, Dehdashti F, Luo J, Homb A, Siegel BA, Bartlett NL. 18F-FDG PET/CT for early response assessment in diffuse large B-cell lymphoma: poor predictive value of international harmonization project interpretation. J Nucl Med. 2011;52:386-392.
18. Lin C, Itti E, Haioun C, Petegnief Y, Luciani A, Dupuis J, Paone G, Talbot JN, Rahmouni A, Meignan M. Early 18F-FDG PET for prediction of prognosis in patients with diffuse large B-cell lymphoma: SUV-based assessment versus visual analysis. J Nucl Med. 2007;48:1626-1632.
19. Zinzani PL, Rigacci L, Stefoni V, Broccoli A, Puccini B, Castagnoli A, Vaggelli L, Zanoni L, Argnani L, Baccarani M, Fanti S. Early interim 18F-FDG PET in Hodgkin’s lymphoma: evaluation on 304 patients. Eur J Nucl Med Mol Imaging. 2012;39:4-12.
20. Oh JR, Seo JH, Chong A, Min JJ, Song HC, Kim YC, Bom HS. Whole-body metabolic tumour volume of 18F-FDG PET/CT improves the prediction of prognosis in small cell lung cancer. Eur J Nucl Med Mol Imaging. 2012;39:925-935.
21. Adams HJ, de Klerk JM, Fijnheer R, Heggelman BG, Dubois SV, Nievelstein RA, Kwee TC. Prognostic superiority of the National Comprehensive Cancer Network International Prognostic Index over pretreatment whole-body volumetric-metabolic FDG-PET/CT metrics in diffuse large B-cell lymphoma. Eur J Haematol. 2015;94:532-539.
22. Watanabe S, Manabe O, Hirata K, Oyama-Manabe N, Hattori N, Kikuchi Y, Kobayashi K, Toyonaga T, Tamaki N. The usefulness of (18)F-FDG PET/CT for assessing methotrexate-associated lymphoproliferative disorder (MTX-LPD). BMC Cancer. 2016;16:635.
23. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue. International Agency for Research on Cancer. 2008.
24. The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N Engl J Med. 1993;329:987-994.
25. Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics; 56:337-344.