
INTRODUCTION
Gastric cancer (GC) is one of the most frequently diagnosed cancer worldwide [1]. Although a decline in GC incidence has been observed due to the primary prevention strategies including increased consumption of fresh fruits and vegetables, decreased intake of salt-preserved foods, and reduction in Helicobacter pylori (H. pylori) infection and smoking, GC has a unsatisfying prognosis and still remains the third leading cause of cancer deaths [1, 2]. Thus, more effective prevention strategies for GC are still urgently needed.
Evidences have revealed that gastric carcinogenesis develops from a complex multi-factorial and multi-stage process [3]. And studies report that inflammation is a participant in the neoplastic process [4]. The expression of cyclooxygenase (COX)-2 is increase in GC, suggesting that COX-2 may promote early gastric carcinogenesis [5, 6]. Non-steroidal anti-inflammatory drugs (NSAIDs), including nonselective NSAIDs (i.e., aspirin) and selective NSAIDs (i.e., celecoxib) can inhibit inflammation status through suppressing COX-2. Therefore, NSAIDs as a potential cost-effective chemoprevention pathway against GC gains the most recent interest. However, several epidemiological and clinical studies evaluating the association between NSAIDs and GC risk obtain inconsistent results [7–10]. Several meta-analyses have been performed to assess the association [11–13]. However, no meta-analyses conduct a dose–response analysis to evaluate the relationship between duration and frequency of NSAIDs use and GC risk, and furthermore these published meta-analyses could not conclude that whether the chemopreventive effect is different according to different tumor sites (cardia and non-cardia GC) because cardia and non-cardia GC have different risk factors, tumor characteristics, and biological behavior [14–16]. Besides, there is a lack of reasonable and in-depth subgroup analyses based on different types of NSAIDs use. Indeed, meta-analyses by Tian et al., Abnet et al. and Bosetti et al do not evaluate the duration and frequency of NSAIDs use [11–13], and meta-analysis by Bosetti et al. only assessed aspirin use and do not analyzed the effects of different tumor site [13].
Thus, the aims of this study are to assess the dose–response association between NSAIDs and GC risk and whether the chemopreventive effect of NSAIDs differed according to tumor site (cardia and non-cardia GC), medication type (aspirin and non-aspirin NSAIDs), and duration and frequency of NSAIDs use.
RESULTS
Study selection and study characteristics
3482 studies were initially identified in the literature search. 3319 studies were excluded after reviewing titles and abstracts. After full-text review of the remaining 164 studies, 140 studies were excluded due to irrelevant data of interest and duplicated studies. Finally, 24 full-text studies were included (Supplementary Figure S1) [7–10, 12, 17–35].
The 24 studies were published between 1993 and 2014, and were conducted in the USA, Korea, China, the UK, Italy, Sweden, Denmark, and Russia. Of the eligible studies, fourteen studies assess the chemoprevention of NSAIDs that was not limited to aspirin [9, 12, 22–27, 29–34], and ten studies assess the chemoprevention of aspirin only [7, 8, 10, 17–21, 28, 35]. Moreover, the site of GC was not otherwise specified (GC NOS) in sixteen studies [7–10, 17–21, 27–30, 32, 33, 35], seven studies provided results for cardia and non-cardia GC separately [12, 22–26, 31], one studies provided results for GC NOS and non-cardia GC [34]. The detailed characteristics are showed in Table 1 , Supplementary Table S2, and Supplementary Table S3.
Table 1: Baseline characteristics and design variables of the included studies
Article |
Year |
Country |
Study type |
Sample |
Drug type |
Definition of use |
GC type |
Adjusted variables |
Study quality |
Findings |
|---|---|---|---|---|---|---|---|---|---|---|
Kim |
2015 |
Korea |
PBS cohort |
11715 |
Aspirin |
100mg for ≥6 months |
GC NOS |
NR |
7 |
Longer duration of aspirin use reduced GC NOS risk |
Wang |
2015 |
China |
HBS CCS |
525 |
Aspirin |
≥1/week for ≥1 year |
GC NOS |
Gender, marriage, education, resident district, history of diabetes, BMI, cigarette smoking, alcohol drinking, and helicobacter pylori |
7 |
Aspirin use reduced GC NOS risk |
Gong |
2014 |
Korea |
HBS CCS |
654 |
Aspirin |
NR |
GC NOS |
NR |
6 |
Aspirin use reduced GC NOS risk |
Cook |
2013 |
USA |
PBS random trial |
39876 |
Aspirin |
100 mg of alternate-day |
GC NOS |
NR |
7 |
Aspirin use could not reduce GC NOS risk |
Jacobs |
2012 |
USA |
PBS cohort |
100139 |
Aspirin |
Daily |
GC NOS |
Age, sex, race, education, smoking, BMI, physical activity, history of heart disease, stroke, diabetes, hypertension, cholesterol-lowering drug use, aspirin use, NSAIDs use, and history of colorectal endoscopy |
8 |
Aspirin use reduced GC NOS risk |
Lee |
2012 |
Korea |
HBS CCS |
1966 |
Aspirin |
NR |
GC NOS |
NR |
6 |
Aspirin use reduced GC NOS risk |
Rothwell |
2011 |
UK |
PBS random trials |
10502 |
Aspirin |
Daily |
GC NOS |
NR |
6 |
Longer duration of aspirin use reduced GC NOS risk |
Bertuccio |
2010 |
Italy |
HBS CCS |
772 |
Aspirin |
≥1/week for ≥6 months |
GC NOS |
Period of interview, education, BMI, tobacco smoking, and family history of gastric cancer |
7 |
Aspirin use could not reduce GC NOS risk |
Wu |
2010 |
Taiwan |
PBS cohort |
52161 |
Any NSAIDs |
≥28/month for ≥6 months |
GC NOS |
NR |
7 |
Aspirin use reduced GC NOS risk |
Figueroa |
2009 |
USA |
PBS CCS |
1062 |
Any NSAIDs, aspirin |
≥1/week for ≥6 months |
Cardia GC |
Center, age, race, gender, cigarette smoking, GERD, proxy interview, and BMI |
7 |
Aspirin, non-aspirin, and NSAIDs use reduced non-cardia GC risk but not cardia GC risk |
Epplein |
2009 |
USA |
PBS cohort |
169292 |
Any NSAIDs, aspirin, non-aspirin |
≥2/week for ≥1 months |
Cardia, non-cardia |
Age, sex, ethnicity, smoking, BMI, and alcohol consumption |
7 |
Aspirin and NSAIDs use reduced non-cardia GC risk but not cardia GC risk |
Abnet |
2009 |
USA |
PBS cohort |
311115 |
Any NSAIDs, aspirin, non-aspirin |
≥1/month for ≥1 year |
Cardia, non-cardia |
Age, sex, cigarette smoking status, alcohol, education, fruit intake, vegetable intake, BMI, total energy intake, and physical activity |
7 |
Aspirin, non-aspirin, and NSAIDs use reduced non-cardia GC risk but not cardia GC risk |
Duan |
2008 |
USA |
PBS CCS |
2074 |
Any NSAIDs, aspirin, non-aspirin |
≥2/week for ≥1 month |
Cardia, non-cardia |
Age, sex, race, birthplace, education, smoking status, BMI, UGI history, and antacid use |
7 |
Longer duration of aspirin and NSAIDs use reduced non-cardia GC risk but not cardia GC risk |
Fortuny |
2007 |
USA |
PBS CCS |
2972 |
Any NSAIDs, aspirin, non-aspirin |
≥1 prescriptions |
Cardia, non-cardia |
Age, sex, HMO, years of enrollment in the HMO, race, and use of drug classes other than the studied one |
7 |
Aspirin and NSAIDs use reduced non-cardia GC risk but not cardia GC risk, non-aspirin NSAIDs could not reduce both cardia and non-cardia GC risk |
Trivers |
2005 |
USA |
PBS CCS |
615 |
Any NSAIDs |
≥1/week for 6 months |
Cardia, non-cardia |
NR |
6 |
NSAIDs use could not reduce both cardia and non-cardia GC risk |
Lindblad |
2005 |
Sweden |
PBS CCS |
11023 |
Aspirin, non-aspirin |
any use |
GC NOS |
Sex, age, smoking, alcohol consumption, BMI, calendar year, and UGI disorders |
7 |
Longer duration of non-aspirin NSAIDs use reduced GC NOS risk, aspirin use could not reduce GC NOS risk |
Ratnasinghe |
2004 |
USA |
PBS cohort |
22834 |
Aspirin |
any use |
GC NOS |
BMI, sex, race, poverty index, education and smoking |
6 |
Aspirin use could not reduce GC NOS risk |
Sorensen |
2003 |
Denmark |
PBS cohort |
172057 |
Any NSAIDs |
≥1 prescriptions |
GC NOS |
NR |
6 |
NSAIDs use could not reduce GC NOS risk |
Nomura |
2003 |
USA |
HBS CCS |
746 |
NSAIDs |
≥2/week for ≥3month |
GC NOS |
Sex, age, and ethnicity |
7 |
NSAIDs use reduced GC NOS risk |
Akre |
2001 |
Sweden |
PBS CCS |
1732 |
Aspirin, non-aspirin |
≥1/month |
GC NOS, cardia, non-cardia |
Age, gender and socioeconomic status |
7 |
Aspirin use could not reduce both cardia and non-cardia GC risk |
Langman |
2000 |
UK |
PBS CCS |
2450 |
Any NSAIDs |
≥1 prescriptions |
GC NOS |
Age and smoking status |
7 |
More NSAIDs prescriptions use reduced GC NOS risk |
Coogan |
2000 |
USA |
HBS CCS |
6083 |
NSAIDs, aspirin |
≥4/week for ≥ 3 months |
GC NOS |
Age, sex, interview year, center, race, religion, cigarettes, family history of digestive cancer, education, and alcohol consumption |
8 |
Aspirin use reduced GC NOS risk |
Zaridze |
1999 |
Russia |
HBS CCS |
1058 |
Any NSAIDs, aspirin |
≥2/week for 6 months |
GC NOS, non-cardia |
Age and education |
6 |
Aspirin and NSAIDs use reduced non-cardia GC risk but not cardia GC risk |
Thun |
1993 |
USA |
PBS cohort |
635031 |
Aspirin |
≥1/month |
GC NOS |
Age, race, sex, BMI, number of cigarette smoked, drinks of alcohol, total dietary fat, and fruit/vegetable/grain consumption, family history of the specific cancer, any tobacco use, and ever pipe or cigar |
8 |
Aspirin use reduced GC NOS risk |
Abbreviations, BMI: Body mass index; CCS: Case-control study; GC: Gastric cancer; GERD: Gastroesophageal reflux disease; HBS: Hospital-based study; HMO: Health maintenance organization; NOS: Not otherwise specified; NR: Not reported; NSAIDs: Non-steroidal anti-inflammatory drugs; PBS: Population-based study; UGI: Upper gastrointestinal; UK: the United Kingdom; USA: the United States of America.
NSAIDs use and GC NOS
Our results indicated that any NSAIDs use was inversely associated with GC risk (RR=0.78, 96%CI=0.72-0.85, Figure 1). Both aspirin use and non-aspirin NSAIDs use had a chemopreventive effect for GC (aspirin: RR=0.70, 95%CI=0.62-0.80; non-aspirin NSAIDs: RR= 0.86, 95%CI=0.80-0.94) (Supplementary Figure S2). As was shown by subgroup analysis on the study design, sample size, and country, the chemopreventive effect of NSAIDs on GC was confirmed in any NSAIDs group, aspirin subgroup, and non-aspirin NSAIDs subgroup (Table 2).
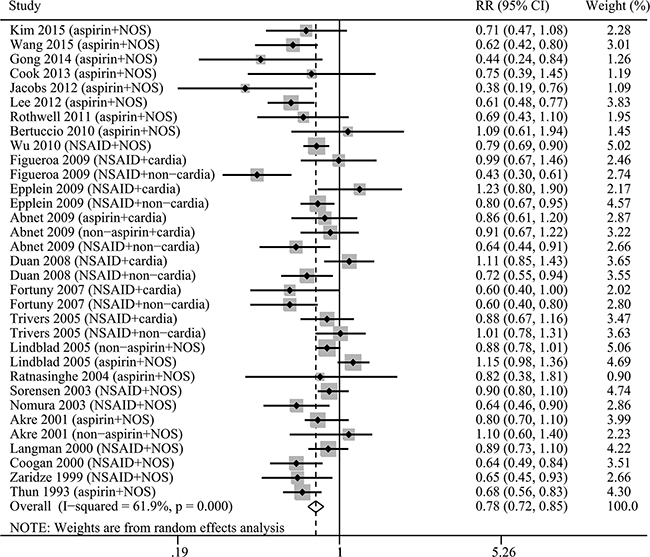
Figure 1: The relative risk (RR) was summarized for the relationship between any NSAIDs use and gastric cancer risk.
Table 2: The results of subgroup analyses for the relationship between NSAIDs and gastric cancer risk
GC NOS |
Non-cardia GC |
Cardia GC |
||||
|---|---|---|---|---|---|---|
RR |
I2 (%) |
RR |
I2 (%) |
RR |
I2 (%) |
|
Any NSAIDs |
||||||
Total |
0.78[0.72-0.85] |
61.9% |
0.70[0.59-0.84] |
69.6% |
0.93[0.82-1.05] |
16.2% |
Study type |
||||||
Cohort |
0.80[0.74-0.86] |
24.5% |
0.77[0.66-0.90] |
15.0% |
0.95[0.78-1.16] |
0.0% |
Case-control |
0.78[0.69-0.88] |
71.9% |
0.68[0.53-0.88] |
76.9% |
0.91[0.79-1.07] |
38.3% |
Study quality |
||||||
≥7 |
0.78[0.70-0.86] |
66.1% |
0.65[0.51-0.83] |
69.5% |
0.91[0.79-1.05] |
23.4% |
<7 |
0.80[0.70-0.92] |
52.9% |
0.78[0.58-1.05] |
71.6% |
0.97[0.77-1.22] |
39.1% |
PBS/HBS |
||||||
PBS |
0.82[0.76-0.90] |
60.0% |
0.73[0.60-0.87] |
69.9% |
0.93[0.82-1.05] |
16.2% |
HBS |
0.64[0.56-0.72] |
0.0% |
/ |
/ |
/ |
/ |
Duration of use |
||||||
≥5 years |
0.65[0.56-0.74] |
49.3% |
0.56[0.46-0.68] |
35.9% |
0.87[0.67-1.12] |
40.3% |
<5 years |
0.78[0.67-0.90] |
54.0% |
0.68[0.51-0.90] |
67.6% |
0.84[0.66-1.08] |
11.2% |
Frequency of use |
||||||
≥7/week |
0.77[0.70-0.85] |
42.6% |
0.64[0.52-0.80] |
0.0% |
1.02[0.82-1.27] |
0.0% |
<7/week |
0.74[0.67-0.83] |
0.0% |
0.66[0.53-0.81] |
0.0% |
0.86[0.69-1.05] |
0.0% |
Sample size |
||||||
<2000 |
0.74[0.65-0.85] |
64.7% |
0.68[0.53-0.88] |
76.9% |
0.91[0.79-1.07] |
38.3% |
≥2000 |
0.82[0.75-0.90] |
56.3% |
0.77[0.66-0.90] |
15.0% |
0.95[0.78-1.16] |
0.0% |
Country |
||||||
Europe & America |
0.81[0.74-0.88] |
61.5% |
0.70[0.59-0.84] |
69.6% |
0.93[0.82-1.05] |
16.2% |
Asia |
0.72[0.65-0.80] |
41.2% |
/ |
/ |
/ |
/ |
H. pylori status |
||||||
H. pylori+ |
0.52[0.42-0.65] |
0.0% |
/ |
/ |
/ |
/ |
H. pylori- |
0.81[0.71-0.91] |
0.0% |
/ |
/ |
/ |
/ |
Aspirin |
||||||
Total |
0.70[0.62-0.80] |
71.7% |
0.64[0.53-0.78] |
68.8% |
0.82[0.61-1.11] |
71.4% |
Study type |
||||||
Cohort |
0.72[0.65-0.80] |
0.0% |
0.70[0.60-0.83] |
0.0% |
0.91[0.70-1.19] |
0.0% |
Case-control |
0.68[0.56-0.84] |
82.1% |
0.61[0.45-0.83] |
78.3% |
0.76[0.47-1.23] |
82.2% |
Study quality |
||||||
≥7 |
0.70[0.59-0.84] |
77.7% |
0.64[0.51-0.80] |
70.7% |
0.79[0.55-1.12] |
76.3% |
<7 |
0.69[0.60-0.79] |
12.8% |
0.63[0.43-0.92] |
60.3% |
/ |
/ |
PBS/HBS |
||||||
PBS |
0.73[0.63-0.85] |
74.7% |
0.66[0.54-0.81] |
70.7% |
0.82[0.61-1.11] |
71.4% |
HBS |
0.61[0.52-0.71] |
20.1% |
/ |
/ |
/ |
/ |
Duration of use |
||||||
≥5 years |
0.73[0.63-0.84] |
21.6% |
0.61[0.49-0.76] |
0.0% |
1.01[0.78-1.31] |
0.0% |
<5 years |
0.92[0.83-1.03] |
43.0% |
0.78[0.65-0.93] |
17.0% |
1.06[0.82-1.37] |
0.0% |
Frequency of use |
||||||
≥7/week |
0.71[0.56-0.89] |
53.5% |
0.65[0.51-0.83] |
0.0% |
1.06[0.82-1.37] |
0.0% |
<7/week |
0.73[0.64-0.82] |
0.0% |
0.67[0.50-0.90] |
0.0% |
0.76[0.56-1.05] |
0.0% |
Sample size |
||||||
<2000 |
0.67[0.55-0.80] |
72.3% |
0.61[0.45-0.83] |
78.3% |
0.76[0.47-1.23] |
82.2% |
≥2000 |
0.75[0.64-0.89] |
67.6% |
0.70[0.60-0.80] |
0.0% |
0.91[0.70-1.19] |
0.0% |
Country |
||||||
Europe & America |
0.72[0.62-0.84] |
74.1% |
0.64[0.53-0.78] |
68.8% |
0.82[0.61-1.11] |
71.4% |
Asia |
0.61[0.52-0.73] |
0.0% |
/ |
/ |
/ |
/ |
H. pylori status |
||||||
H. pylori+ |
0.53[0.36-0.77] |
1.9% |
/ |
/ |
/ |
/ |
H. pylori- |
0.81[0.52-1.26] |
0.0% |
/ |
/ |
/ |
/ |
Non-aspirin |
||||||
Total |
0.86[0.80-0.94] |
31.0% |
0.74[0.60-0.93] |
58.7% |
0.92[0.78-1.09] |
0.0% |
Study type |
||||||
Cohort |
0.91[0.73-1.13] |
51.2% |
0.84[0.57-1.22] |
76.8% |
0.99[0.77-1.28] |
16.1% |
Case-control |
0.84[0.77-0.93] |
22.4% |
0.68[0.55-0.85] |
8.0% |
0.87[0.70-1.10] |
0.0% |
Study quality |
||||||
≥7 |
0.83[0.76-0.91] |
19.9% |
0.68[0.57-0.81] |
0.0% |
0.89[0.74-1.06] |
0.0% |
<7 |
1.04[0.85-1.26] |
0.0% |
/ |
/ |
/ |
/ |
Duration of use |
||||||
≥5 years |
0.84[0.62-1.12] |
0.0% |
0.75[0.51-1.10] |
35.9% |
0.97[0.62-1.51] |
0.0% |
<5 years |
0.85[0.75-0.96] |
33.0% |
0.81[0.66-0.98] |
14.5% |
0.89[0.53-1.48] |
62.3% |
Frequency of use |
||||||
≥7/week |
0.72[0.57-0.90] |
10.2% |
0.63[0.45-0.87] |
50.0% |
1.06[0.82-1.37] |
0.0% |
<7/week |
0.79[0.64-0.97] |
44.8% |
0.64[0.47-0.87] |
16.5% |
0.76[0.56-1.05] |
0.0% |
PBS/HBS |
||||||
PBS |
0.86[0.80-0.94] |
31.0% |
0.74[060-0.93] |
58.7% |
0.93[0.78-1.09] |
0.0% |
HBS |
/ |
/ |
/ |
/ |
/ |
/ |
Sample size |
||||||
<2000 |
0.80[0.69-0.93] |
26.0% |
0.68[0.55-0.85] |
8.0% |
0.87[0.70-1.10] |
0.0% |
≥2000 |
0.89[0.81-0.98] |
36.3% |
0.84[0.58-1.22] |
76.8% |
0.99[0.77-1.28] |
16.1% |
Country |
||||||
Europe & America |
0.86[0.80-0.94] |
31.0% |
0.74[0.60-0.93] |
58.7% |
0.93[0.78-1.09] |
0.0% |
Asia |
/ |
/ |
/ |
/ |
/ |
|
Abbreviations, GC: Gastric cancer; HBS: Hospital-based study; NOS: Not otherwise specified; PBS: Population-based study; RR: Risk ratio; “/” symbol: No results due to insufficient studies
I2 shows the degree of heterogeneity among studies.
We observed a lower GC risk in studies with longer duration of NSAIDs use compared with studies with shorter duration (RR=0.65 for ≥ 5 years VS RR=0.78 for < 5 years, Table 2 ). The results of dose–response analysis indicated that there were insignificant non-linear relationships between duration of any NSAIDs use and aspirin use and GC risk (any NSAIDs: P for non-linearity=0.12, Figure 2; aspirin: P for non-linearity= 0.27), so linear regression models were fitted (any NSAIDs: P for linear trend<0.01; aspirin: P for linear trend=0.01). And every 2 years increment for any NSAIDs use was inversely associated with GC risk (RR=0.89, 95 % CI=0.83-0.96), and aspirin use tended toward a potentially chemopreventive effect (RR=0.95, 95%CI=0.88-1.02), suggesting that similar trends were observed with linear model and subgroup analysis based on duration of NSAIDs use. A non-linear relationship existed in non-aspirin NSAIDs (P for non-linearity=0.02) and there was a maximal chemopreventive effect at duration of 5 years, with a monotonically decreasing trend for duration of less than 5 years and a increasing trend for duration of more than 5 years. Besides, a separate analysis with a linear model showed a decreased trend of GC risk for 2 years increment (RR=0.96, 95%CI=0.93-0.99).
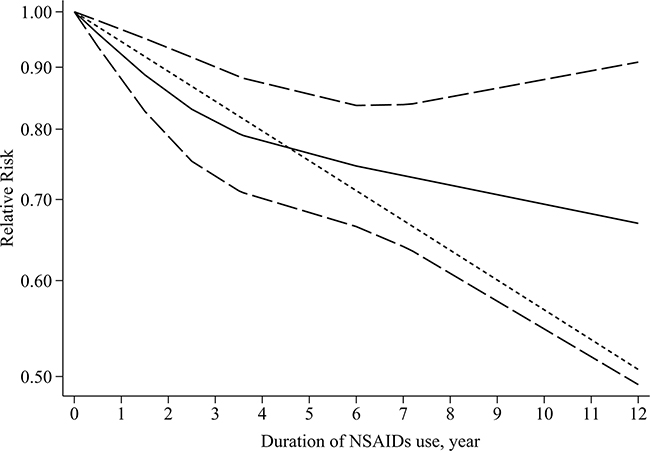
Figure 2: Dose–response relationship between duration of any NSAIDs use and gastric cancer risk. Relative risk (RR; –––) and the corresponding 95% confidence intervals (CI; – – –) were summarized for the dose–response relationship between duration of any NSAIDs use (year) and gastric cancer risk. Data were modeled with restricted cubic spline models, where - - - - represents the linear trend.
We observed a similar GC risk in studies with more frequency of NSAIDs use compared with studies with less frequency (RR=0.77 for ≥7/week VS RR=0.74 for < 5 years, Table 2 ). There were non-linear relationships between frequency of any NSAIDs use and aspirin use and GC risk (any NSAIDs: P for non-linearity<0.01, Figure 3; aspirin: P for non-linearity<0.01) and a linear relationship in frequency of non-aspirin NSAIDs (P for non-linearity=0.38, P for linear trend<0.01). The chemopreventive effect of any NSAIDs and aspirin use for GC risk may be maximal at 5/week. A monotonically decreasing trend was observed for frequency of less than 5/week, but the inverse relationship was attenuated gradually for frequency of more than 5/week. In addition, we also evaluated the potential relationships in a separate analysis with a linear model and the results showed a decreased trend of GC risk as per 2/week increase in frequency of any NSAIDs (RR=0.90, 95%CI=0.85-0.96) and aspirin (RR=0.90, 95%CI=0.85-0.97).
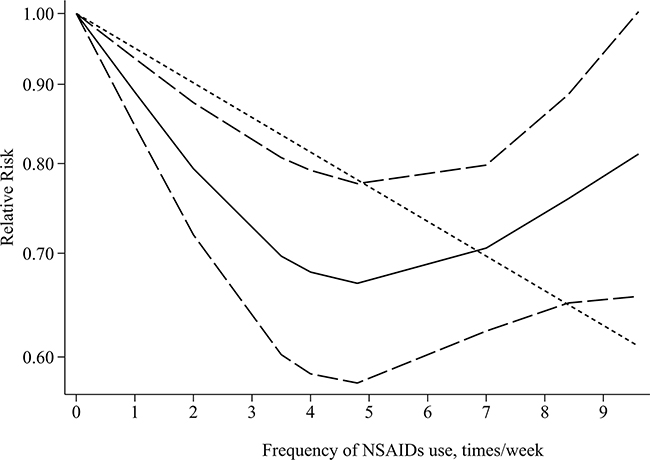
Figure 3: Dose–response relationship between frequency of any NSAIDs use and gastric cancer risk. Relative risk (RR; –––) and the corresponding 95% confidence intervals (CI; – – –) were summarized for the dose–response relationship between frequency of any NSAIDs use (year) and gastric cancer risk. Data were modeled with restricted cubic spline models, where - - - - represents the linear trend.
NSAIDs use and non-cardia GC
Any NSAIDs use had a chemopreventive effect for non-cardia GC risk (RR=0.70, 96%CI=0.59-0.84, Figure 4). In the term of medication type, aspirin use and non-aspirin NSAIDs use were associated with non-cardia GC (aspirin: RR=0.64, 95%CI=0.53-0.78; non-aspirin NSAIDs: RR= 0.74, 95%CI=0.60-0.93, Figure 4). Subgroup analysis based on the study design, sample size, and country could obtain similar trend, confirming the stability of our results (Table 2).
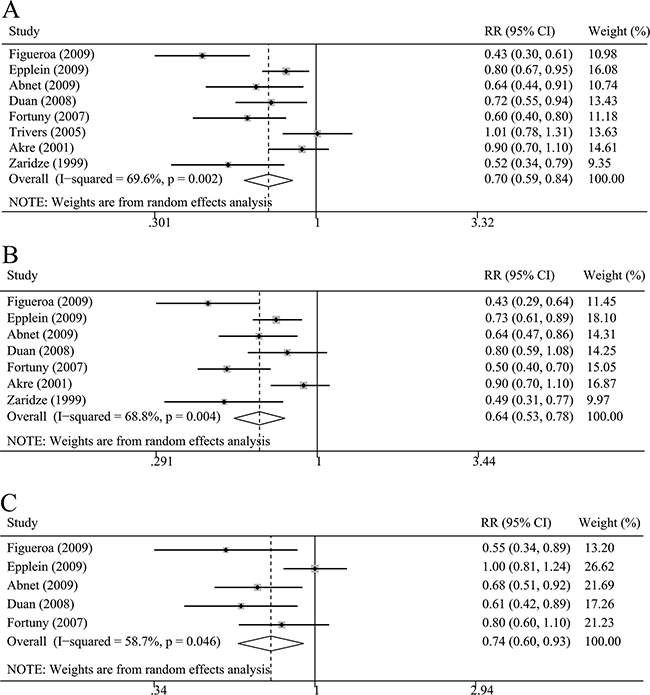
Figure 4: The relative risk (RR) was summarized for the relationship between NSAIDs use and non-cardia gastric cancer risk. A. Any NSAIDs use and non-cardia gastric cancer. B. Aspirin use and non-cardia gastric cancer. (C): Non-aspirin NSAIDs use and non-cardia gastric cancer.
Longer duration of NSAIDs use had a lower non-cardia GC risk compared with studies with shorter duration (≥ 5 years VS < 5 years, Table 2 ). There were insignificant nonlinear and significant linear relationships between duration of any NSAIDs use and aspirin use and non-cardia GC risk with a decreased trend of non-cardia GC risk as per 2 year increase in duration (any NSAIDs: P for non-linearity=0.07, P for linear trend<0.01, RR=0.83, 95%CI=0.72-0.96; aspirin: P for non-linearity=0.50, P for linear trend<0.01, RR=0.87, 95%CI=0.81-0.93).
NSAIDs use and cardia GC
Our results indicated that NSAIDs was not associated with cardia GC risk (any NSAIDs: RR= 0.93, 95%CI=0.82-1.05; aspirin: RR= 0.82, 95%CI=0.61-1.11; non-aspirin NSAIDs: RR=0.92, 95%CI=0.78-1.09) (Supplementary Figure S3). Subgroup analysis in any NSAIDs group, aspirin subgroup and non-aspirin NSAIDs subgroup based on study design, sample size and country showed that NSAIDs use did not reduce the risk of cardia GC risk (Table 2). The results of dose-response analysis also showed that increase in duration and frequency of NSAIDs use was not associated with cardia GC risk.
Assessment of publication bias
The results of Begg’s and Egger’s tests showed no evidence of publication bias, except in the relationship between non-aspirin NSAIDs and non-cardia GC (PBegg's = 0.09, PEgger's = 0.02) (Supplementary Table S4, Supplementary Figure S4). And the trim-and-fill analysis indicated that publication bias could not substantially impact on the results for the relationship between non-aspirin NSAIDs and non-cardia GC (RR=0.86, 95%CI=0.76-0.97).
DISCUSSION
Gastric cancer (GC) is a global health problem with unfavorable prognosis [1]. Thus, effective prevention strategies for GC were important for public health. Recently, body of evidence has reported that NSAIDs have protective effects on numerous solid cancer risks [36–38]. However, there are no general agreements about the chemopreventive effect of NSAIDs in GC. Moreover, it remains unclear that whether the chemopreventive effect is different according to differences of tumor site, medication type, and duration and frequency of NSAIDs use.
Our results of both overall and subgroup analysis indicated that any NSAIDs, aspirin, and non-aspirin NSAIDs use could reduce GC risk, especially for non-cardia GC risk. In addition, dose-response analysis indicated decreased trend of GC risk as per 2 years increase in duration of any NSAIDs use and aspirin use, with insignificant nonlinear dose-response relationships. There were nonlinear relationships between frequency of any NSAIDs use and aspirin use and GC risk, and a monotonically decreasing trend was observed only for frequency of less than 5/week, thus the chemopreventive effect of any NSAIDs and aspirin use may be maximal at 5/week.
There were several possible mechanisms responsible for the chemopreventive effect of NSAIDs. The main anti-cancer mechanism was attributed to the blockade of COX-2 pathway because expression of COX-2 was associated with gastric carcinogenesis through promotion of cell proliferation, inhibition of apoptosis, and induction of angiogenesis [6, 39]. Indeed, Sawaoka et al. demonstrated that NSAIDs exerted anti-proliferative activity against GC that overexpressed COX-2 [40]. Nam et al. also reported that NSAIDs could prevent gastric carcinogenesis in mouse models [41]. In addition, some NSAIDs could induce cell death and inhibit proliferation in cells without expression of COX, thus several studies suggested that COX was not the sole target of NSAIDs and other targets may also promote apoptosis [42, 43]. Kopp et al. and Yamamoto et al. demonstrated that NSAIDs could promote apoptosis by inhibiting the activation of nuclear factor κb [44, 45]. Several studies also reported that NSAIDs could prevent carcinogenesis via B-catenin, wnt signalling, tumour necrosis factor, polyamine metabolism and the DNA mismatch repair system[46, 47]. Moreover, NSAIDs could inhibit replication and proliferation of H. pylori and potentially increase H. pylori clearance [48, 49]. Thus, future studies are needed to elucidate mechanisms of NSAIDs involving in carcinogenesis and investigate whether NSAIDs could be used for the treatment of gastric precancerosis and combination treatment of GC.
Our overall, subgroup, and dose-response analyses consistently showed that NSAIDs use was associated with low risk of non-cardia GC but not of cardia GC. Several clinical studies also found that NSAIDs or aspirin use was associated with only non-cardia GC but not with cardia GC [12, 22, 23, 50]. The potential reason for the different chemopreventive effect of NSAIDs between different anatomic sites was that the risk factors and biological behavior of cardia GC differed greatly from that of non-cardia GC [14–16]. As a definite carcinogen, H. pylori infection, which could cause chronic inflammation in stomach and then lead to COX-2 expression and prostaglandin synthesis, was a strong risk factor for non-cardia GC but was not associated with the risk of cardia GC [23, 51]. Indeed, a meta-analysis by Cavaleiro-Pinto et al. reported a no relationship between H. pylori and cardia GC with summary RR of 1.08 (95% CI 0.83–1.40)[52]. The incidence of COX-2 overexpression in cardia GC was lower compared with non-cardia GC [53]. Thus, NSAIDs may not markedly reduce the cardia GC risk via inhibiting COX-2. Future studies are needed to investigate the differences of carcinogenesis mechanisms between cardia and non-cardia GC, contributing to primary prevention strategies.
Although NSAIDs use could reduce GC risk, it is still confusing that which type of NSAIDs has a stronger chemopreventive effect for GC. Aspirin was one of the most widely used NSAIDs worldwide. Thus, we conducted subgroup analysis based aspirin and non-aspirin NSAIDs (including many selective NSAIDs that inhibit COX-2 only), and the results indicated that a greater chemopreventive effect of aspirin than that of non-aspirin NSAIDs. Aspirin was non-selective NSAIDs that inhibit COX-1 and COX-2, and experimental study reported that both COX-1 and COX-2 could substantially overexpress in tumor tissues [54]. Therefore, COX-1-dependent effect of NSAIDs might promote chemoprevention for GC besides COX-2-dependent effect. Indeed, Tsuji et al. have demonstrated that COX-1 expressed in tumor could participate in tumor angiogenesis and non-selective NSAIDs had an obviously anti-cancer effect by inhibition of COX-1 [55]. Thus, future studies are needed to explore which NSAIDs type should be used for chemoprevention of GC, considering COX-1-dependent and COX-2-dependent effect simultaneously.
The frequency, duration and dose of NSAIDs use was one of the most important questions, considering efficacy and adverse effects simultaneously. However, the definitions of NSAIDs use in included studies were different. Thus, it was important to evaluate how different definitions of NSAIDs use may impact the results, and we conducted both subgroup analysis and dose-response analysis based on frequency and duration of NSAIDs use. For the frequency of NSAIDs use, subgroup analysis indicated that there was no obviously decreasing trend with increasing frequency of NSAIDs use. Indeed, a nonlinear relationship showed the existence of a threshold effect (5/week) between frequency of NSAIDs use and GC risk, with a monotonically decreasing trend for ≤ 5/week and increasing trend for > 5/week. A similar nonlinear relationship with a threshold effect was also reported in esophageal adenocarcinoma and colorectal cancer [56, 57]. The reasons for the nonlinear relationship were unclear. The chemoprevention of NSAIDs through COX-2-dependent pathway required a much shorter dosing interval because nucleated cells could rapidly resynthesize the COX-2, however, high frequency of NSAIDs use may attenuate their chemopreventive effect due to serious gastric mucosal injury caused by NSAIDs [58, 59]. Moreover, another meaningful and important result was the inversely linear relationship between duration of NSAIDs and GC risk. The risk of non-cardia GC decreased by 17% and 13% for 2 years increment of any NSAIDs and aspirin use, respectively. However, most of included studies did not clearly define the dose of NSAIDs use, and thus the present study could not analyze whether the dose of NSAIDs use would impact the chemopreventive effect. Future studies should assess the risk-benefit profile of NSAIDs use, and explore the optimal duration, frequency and dose of NSAIDs use for chemoprevention for GC.
There were several limitations in this study. First, although the association between duration and frequency of NSAIDs use and GC risk were analyzed, it was still unclear that whether the dose of NSAIDs would impact the chemopreventive effect of NSAIDs. Second, detailed individual information was not available from each published studies. Thus, we could not perfectly adjust all important confounding factors, and confounding factors may underestimate chemopreventive effect of NSAIDs on GC. Third, we could not evaluate the side effects of NSAIDs use, such as gastrointestinal bleeding and ulcer perforation owing to limited data. Thus, whether the chemopreventive benefit of NSAIDs outweighed their side effects was unclear. Moreover, a considerable degree of heterogeneity was observed among the studies and could not be explained completely.
In conclusion, our results indicate that NSAIDs use, including aspirin and non-aspirin NSAIDs, is inversely associated with GC risk, especially for non-cardia GC risk. NSAIDs use may become a feasible approach to prevent non-cardia GC.
MATERIALS AND METHODS
Literature search
A literature search was performed for relevant studies using the PubMed and Embase database (up to March 2016). The reference lists of relevant studies and reviews were manually checked for potential studies. The main search terms were as follows: “non-steroidal anti-inflammatory drugs,” “NSAIDs”, “cyclooxygenase-2 inhibitors”, “COX-2 inhibitors”, “aspirin”, “salicylate”, “acetaminophen”, “gastric cancer”, and “stomach cancer”.
Eligibility criteria
Studies were included if met all the following inclusion criteria: (1) the exposure of interest was any type of NSAIDs, (2) the outcome of interest was GC, including cardia and non-cardia GC, (3) the effect estimates [hazard ratios (HRs), risk ratios (RRs), or odds ratios (ORs)] and corresponding 95% confidence intervals (CIs) could be extracted or calculated from published data, (4) the full text could be obtained. Only the most informative study was included if several duplicated studies were based on the same population. To retain maximum information, some data that only reported in excluded duplicated studies were extracted and added it into the included duplicated study.
Data extraction and quality assessment
Two reviewers independently extracted following data: first author, publication country and year, study name, study design, definition of NSAIDs use, medication type, tumor site, sample size, duration and frequency of NSAIDs use, effect measures with corresponding 95% CIs, and adjusted variables. The study quality was assessed by Newcastle-Ottawa Scale criteria [60]. Any disagreements on the data extraction were resolved by comprehensive discussion of three authors.
Statistical analysis
The association between NSAIDs and GC risk was summarized by RRs with 95% CIs. The ORs provided by case-control studies were used as RRs in the pooled process because GC incidence was sufficiently low and the ORs were close to the RRs [61]. If there were various RRs for different population databases in one study, each population database was considered as one independent study. Overall analysis was performed by including all the relevant studies. Subgroup analysis was performed on basis of NSAIDs type, tumor site, duration and frequency of NSAIDs use, study design, quality of study, publication country, and sample size.
A dose–response analysis was used to evaluate the relationship between duration and frequency of NSAIDs use and GC risk (Supplementary File S1) [62, 63]. This analysis required the distribution of cases and non-cases, assigned values of duration and frequency of NSAIDs use, and risk estimates in each category for each study. For intervals, the midpoint of the interval was chosen, and the assigned value of the lowest category was designated as a reference level. For the open-ended upper interval, the value assigned was 20% higher than the low end of the interval [64]. We used restricted cubic splines with three knots at the 25%, 50%, and 75% percentiles of the distribution to examine a potential non-linear dose–response relationship between GC risk and duration and frequency of NSAIDs use [65, 66]. A P-value for non-linearity was calculated by testing the null hypothesis that the regression coefficient of the second spline was equal to zero [65]. A linear dose-response relationship was examined by generalized least-squares regression [63].
The Cochran Q test and the I2 statistic were used to measure heterogeneity [67]. If there was substantial heterogeneity, a random effect model was used; otherwise, a fixed effect model was used. Publication bias was evaluated utilizing Egger’s and Begg’s tests, and trim-and-fill analysis was conducted if there was publication bias [68–70].
All statistical analyses were performed with Stata software (Version 12.0; Stata Corporation, College Station, Texas, USA, 2011). A two-sided P-value <0.05 was considered statistical significance.
Abbreviations
CI: Confidence Intervals; COX: Cyclooxygenase; GC: Gastric Cancer; H. pylori: Helicobacter pylori; HR: Hazard Ratio; NSAIDs: Non-steroidal Anti-inflammatory Drugs; OR: Odds Ratio; RR: Risk Ratio
.ACKNOWLEDGMENTS
We thank the department of Chemotherapy and Radiotherapy of Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University for technical assistance. The corresponding author had full access to all the data and analyses.
CONFLICTS OF INTEREST
All authors declare that they have no competing interests.
GRANT SUPPORT
None
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J and Jemal A. Global cancer statistics, 2012. CA. 2015; 65:87-108.
2. Bertuccio P, Chatenoud L, Levi F, Praud D, Ferlay J, Negri E, Malvezzi M and La Vecchia C. Recent patterns in gastric cancer: a global overview. International journal of cancer. 2009; 125:666-673.
3. Clapp RW, Jacobs MM and Loechler EL. Environmental and occupational causes of cancer: new evidence 2005-2007. Reviews on environmental health. 2008; 23:1-37.
4. Coussens LM and Werb Z. Inflammation and cancer. Nature. 2002; 420:860-867.
5. Lim HY, Joo HJ, Choi JH, Yi JW, Yang MS, Cho DY, Kim HS, Nam DK, Lee KB and Kim HC. Increased expression of cyclooxygenase-2 protein in human gastric carcinoma. Clinical cancer research. 2000; 6:519-525.
6. Wang Z, Chen JQ and Liu JL. COX-2 Inhibitors and Gastric Cancer. Gastroenterology research and practice. 2014; 2014:132320.
7. Bertuccio P, Bravi F, Bosetti C, Negri E and La Vecchia C. Aspirin and gastric cancer risk. European journal of cancer prevention. 2010; 19:426-427.
8. Cook NR, Lee IM, Zhang SM, Moorthy MV and Buring JE. Alternate-day, low-dose aspirin and cancer risk: long-term observational follow-up of a randomized trial. Annals of internal medicine. 2013; 159:77-85.
9. Wu CY, Wu MS, Kuo KN, Wang CB, Chen YJ and Lin JT. Effective reduction of gastric cancer risk with regular use of nonsteroidal anti-inflammatory drugs in Helicobacter pylori-infected patients. Journal of clinical oncology. 2010; 28:2952-2957.
10. Wang Y, Shen C, Ge J and Duan H. Regular aspirin use and stomach cancer risk in China. European journal of surgical oncology. 2015; 41:801-804.
11. Tian W, Zhao Y, Liu S and Li X. Meta-analysis on the relationship between nonsteroidal anti-inflammatory drug use and gastric cancer. European journal of cancer prevention. 2010; 19:288-298.
12. Abnet CC, Freedman ND, Kamangar F, Leitzmann MF, Hollenbeck AR and Schatzkin A. Non-steroidal anti-inflammatory drugs and risk of gastric and oesophageal adenocarcinomas: results from a cohort study and a meta-analysis. British journal of cancer. 2009; 100:551-557.
13. Bosetti C, Rosato V, Gallus S, Cuzick J and La Vecchia C. Aspirin and cancer risk: a quantitative review to 2011. Annals of oncology. 2012; 23:1403-1415.
14. Ichikura T, Ogawa T, Kawabata T, Chochi K, Sugasawa H and Mochizuki H. Is adenocarcinoma of the gastric cardia a distinct entity independent of subcardial carcinoma? World journal of surgery. 2003; 27:334-338.
15. Cho Y, Lee DH, Oh HS, Seo JY, Lee DH, Kim N, Jeong SH, Kim JW, Hwang JH, Park YS, Lee SH, Shin CM, Jo HJ, Jung HC, Yoon YB and Song IS. Higher prevalence of obesity in gastric cardia adenocarcinoma compared to gastric non-cardia adenocarcinoma. Digestive diseases and sciences. 2012; 57:2687-2692.
16. Xue L, Zhang X, Li Y, Yang H, Li X, Mi J, Wang H, Wang J and Yan X. Differences of immunophenotypic markers and signaling molecules between adenocarcinomas of gastric cardia and distal stomach. Human pathology. 2011; 42:594-601.
17. Kim YI, Kim SY, Kim JH, Lee JH, Kim YW, Ryu KW, Park JH and Choi IJ. Long-term Low-dose Aspirin use Reduces Gastric Cancer Incidence: A Nationwide Cohort Study. Cancer research and treatment. 2016; 48: 798-805.
18. Gong EJ, Ahn JY, Jung HY, Lim H, Choi KS, Lee JH, Kim do H, Choi KD, Song HJ, Lee GH, Kim JH, Choi SY, Choe JW and Kim MJ. Risk factors and clinical outcomes of gastric cancer identified by screening endoscopy: a case-control study. Journal of gastroenterology and hepatology. 2014; 29:301-309.
19. Jacobs EJ, Newton CC, Gapstur SM and Thun MJ. Daily aspirin use and cancer mortality in a large US cohort. Journal of the National Cancer Institute. 2012; 104:1208-1217.
20. Lee J, Lee SH, Hur KY, Woo SY, Kim SW and Kang WK. Statins and the risk of gastric cancer in diabetes patients. BMC cancer. 2012; 12:596.
21. Rothwell PM, Fowkes FG, Belch JF, Ogawa H, Warlow CP and Meade TW. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet. 2011; 377:31-41.
22. Figueroa JD, Terry MB, Gammon MD, Vaughan TL, Risch HA, Zhang FF, Kleiner DE, Bennett WP, Howe CL, Dubrow R, Mayne ST, Fraumeni JF, Jr. and Chow WH. Cigarette smoking, body mass index, gastro-esophageal reflux disease, and non-steroidal anti-inflammatory drug use and risk of subtypes of esophageal and gastric cancers by P53 overexpression. Cancer causes & control. 2009; 20:361-368.
23. Epplein M, Nomura AM, Wilkens LR, Henderson BE and Kolonel LN. Nonsteroidal antiinflammatory drugs and risk of gastric adenocarcinoma: the multiethnic cohort study. American journal of epidemiology. 2009; 170:507-514.
24. Duan L, Wu AH, Sullivan-Halley J and Bernstein L. Nonsteroidal anti-inflammatory drugs and risk of esophageal and gastric adenocarcinomas in Los Angeles County. Cancer epidemiology, biomarkers & prevention. 2008; 17:126-134.
25. Fortuny J, Johnson CC, Bohlke K, Chow WH, Hart G, Kucera G, Mujumdar U, Ownby D, Wells K, Yood MU and Engel LS. Use of anti-inflammatory drugs and lower esophageal sphincter-relaxing drugs and risk of esophageal and gastric cancers. Clinical gastroenterology and hepatology. 2007; 5:1154-1159.e1153.
26. Trivers KF, De Roos AJ, Gammon MD, Vaughan TL, Risch HA, Olshan AF, Schoenberg JB, Mayne ST, Dubrow R, Stanford JL, Abrahamson P, Rotterdam H, West AB, Fraumeni JF and Chow WH. Demographic and lifestyle predictors of survival in patients with esophageal or gastric cancers. Clinical gastroenterology and hepatology. 2005; 3:225-230.
27. Lindblad M, Lagergren J and Garcia Rodriguez LA. Nonsteroidal anti-inflammatory drugs and risk of esophageal and gastric cancer. Cancer epidemiology, biomarkers & prevention. 2005; 14:444-450.
28. Ratnasinghe LD, Graubard BI, Kahle L, Tangrea JA, Taylor PR and Hawk E. Aspirin use and mortality from cancer in a prospective cohort study. Anticancer research. 2004; 24:3177-3184.
29. Sorensen HT, Friis S, Norgard B, Mellemkjaer L, Blot WJ, McLaughlin JK, Ekbom A and Baron JA. Risk of cancer in a large cohort of nonaspirin NSAID users: a population-based study. British journal of cancer. 2003; 88:1687-1692.
30. Nomura AM, Hankin JH, Kolonel LN, Wilkens LR, Goodman MT and Stemmermann GN. Case-control study of diet and other risk factors for gastric cancer in Hawaii (United States). Cancer causes & control. 2003; 14:547-558.
31. Akre K, Ekstrom AM, Signorello LB, Hansson LE and Nyren O. Aspirin and risk for gastric cancer: a population-based case-control study in Sweden. British journal of cancer. 2001; 84:965-968.
32. Langman MJ, Cheng KK, Gilman EA and Lancashire RJ. Effect of anti-inflammatory drugs on overall risk of common cancer: case-control study in general practice research database. BMJ. 2000; 320:1642-1646.
33. Coogan PF, Rosenberg L, Palmer JR, Strom BL, Zauber AG, Stolley PD and Shapiro S. Nonsteroidal anti-inflammatory drugs and risk of digestive cancers at sites other than the large bowel. Cancer epidemiology, biomarkers & prevention. 2000; 9:119-123.
34. Zaridze D, Borisova E, Maximovitch D and Chkhikvadze V. Aspirin protects against gastric cancer: results of a case-control study from Moscow, Russia. International journal of cancer. 1999; 82:473-476.
35. Thun MJ, Namboodiri MM, Calle EE, Flanders WD and Heath CW, Jr. Aspirin use and risk of fatal cancer. Cancer research. 1993; 53:1322-1327.
36. de Pedro M, Baeza S, Escudero MT, Dierssen-Sotos T, Gomez-Acebo I, Pollan M and Llorca J. Effect of COX-2 inhibitors and other non-steroidal inflammatory drugs on breast cancer risk: a meta-analysis. Breast cancer research and treatment. 2015; 149:525-536.
37. Friis S, Riis AH, Erichsen R, Baron JA and Sorensen HT. Low-Dose Aspirin or Nonsteroidal Anti-inflammatory Drug Use and Colorectal Cancer Risk: A Population-Based, Case-Control Study. Annals of internal medicine. 2015; 163:347-355.
38. Lapi F, Levi M, Simonetti M, Cancian M, Parretti D, Cricelli I, Sobrero A and Cricelli C. Risk of prostate cancer in low-dose aspirin users: A retrospective cohort study. International journal of cancer. 2016; 139:205-211.
39. Jana NR. NSAIDs and apoptosis. Cellular and molecular life sciences. 2008; 65:1295-1301.
40. Sawaoka H, Kawano S, Tsuji S, Tsujii M, Murata H and Hori M. Effects of NSAIDs on proliferation of gastric cancer cells in vitro: possible implication of cyclooxygenase-2 in cancer development. Journal of clinical gastroenterology. 1998; 27 Suppl 1:S47-52.
41. Nam KT, Hahm KB, Oh SY, Yeo M, Han SU, Ahn B, Kim YB, Kang JS, Jang DD, Yang KH and Kim DY. The selective cyclooxygenase-2 inhibitor nimesulide prevents Helicobacter pylori-associated gastric cancer development in a mouse model. Clinical cancer research. 2004; 10:8105-8113.
42. Jiang XH and Wong BC. Cyclooxygenase-2 inhibition and gastric cancer. Current pharmaceutical design. 2003; 9:2281-2288.
43. Piazza GA, Alberts DS, Hixson LJ, Paranka NS, Li H, Finn T, Bogert C, Guillen JM, Brendel K, Gross PH, Sperl G, Ritchie J, Burt RW, Ellsworth L, Ahnen DJ and Pamukcu R. Sulindac sulfone inhibits azoxymethane-induced colon carcinogenesis in rats without reducing prostaglandin levels. Cancer research. 1997; 57:2909-2915.
44. Kopp E and Ghosh S. Inhibition of NF-kappa B by sodium salicylate and aspirin. Science. 1994; 265:956-959.
45. Yamamoto Y, Yin MJ, Lin KM and Gaynor RB. Sulindac inhibits activation of the NF-kappaB pathway. The Journal of biological chemistry. 1999; 274:27307-27314.
46. Elwood PC, Gallagher AM, Duthie GG, Mur LA and Morgan G. Aspirin, salicylates, and cancer. Lancet. 2009; 373:1301-1309.
47. Langley RE, Burdett S, Tierney JF, Cafferty F, Parmar MK and Venning G. Aspirin and cancer: has aspirin been overlooked as an adjuvant therapy? British journal of cancer. 2011; 105:1107-1113.
48. Wang WH, Wong WM, Dailidiene D, Berg DE, Gu Q, Lai KC, Lam SK and Wong BC. Aspirin inhibits the growth of Helicobacter pylori and enhances its susceptibility to antimicrobial agents. Gut. 2003; 52:490-495.
49. Sawaoka H, Kawano S, Tsuji S, Tsuji M, Sun W, Gunawan ES and Hori M. Helicobacter pylori infection induces cyclooxygenase-2 expression in human gastric mucosa. Prostaglandins, leukotrienes, and essential fatty acids. 1998; 59:313-316.
50. Farrow DC, Vaughan TL, Hansten PD, Stanford JL, Risch HA, Gammon MD, Chow WH, Dubrow R, Ahsan H, Mayne ST, Schoenberg JB, West AB, Rotterdam H, Fraumeni JF, Jr. and Blot WJ. Use of aspirin and other nonsteroidal anti-inflammatory drugs and risk of esophageal and gastric cancer. Cancer epidemiology, biomarkers & prevention. 1998; 7:97-102.
51. Kamangar F, Dawsey SM, Blaser MJ, Perez-Perez GI, Pietinen P, Newschaffer CJ, Abnet CC, Albanes D, Virtamo J and Taylor PR. Opposing risks of gastric cardia and noncardia gastric adenocarcinomas associated with Helicobacter pylori seropositivity. Journal of the National Cancer Institute. 2006; 98:1445-1452.
52. Cavaleiro-Pinto M, Peleteiro B, Lunet N and Barros H. Helicobacter pylori infection and gastric cardia cancer: systematic review and meta-analysis. Cancer causes & control. 2011; 22:375-387.
53. Ratnasinghe D, Tangrea JA, Roth MJ, Dawsey SM, Anver M, Kasprzak BA, Hu N, Wang QH and Taylor PR. Expression of cyclooxygenase-2 in human adenocarcinomas of the gastric cardia and corpus. Oncology reports. 1999; 6:965-968.
54. Hwang D, Scollard D, Byrne J and Levine E. Expression of cyclooxygenase-1 and cyclooxygenase-2 in human breast cancer. Journal of the National Cancer Institute. 1998; 90:455-460.
55. Tsuji S, Tsujii M, Kawano S and Hori M. Cyclooxygenase-2 upregulation as a perigenetic change in carcinogenesis. Journal of experimental & clinical cancer research. 2001; 20:117-129.
56. Ye X, Fu J, Yang Y and Chen S. Dose-risk and duration-risk relationships between aspirin and colorectal cancer: a meta-analysis of published cohort studies. PloS one. 2013; 8:e57578.
57. Xiaohua Y, Zhenjiang Y, Weidong L, Pengcheng X and Sidong C. The non-linear threshold association between aspirin use and esophageal adenocarcinoma: results of a dose-response meta-analysis. Pharmacoepidemiology and drug safety. 2014; 23:278-284.
58. Patrono C, Coller B, Dalen JE, FitzGerald GA, Fuster V, Gent M, Hirsh J and Roth G. Platelet-active drugs : the relationships among dose, effectiveness, and side effects. Chest. 2001; 119(1 Suppl):39S-63S.
59. Oshima T, Miwa H and Joh T. Aspirin induces gastric epithelial barrier dysfunction by activating p38 MAPK via claudin-7. American journal of physiology Cell physiology. 2008; 295:C800-806.
60. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. European journal of epidemiology. 2010; 25:603-605.
61. Zhang J and Yu KF. What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. Jama. 1998; 280:1690-1691.
62. Greenland S and Longnecker MP. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. American journal of epidemiology. 1992; 135:1301-1309.
63. Orsini N BR, Greenland S. Generalized least squares for trend estimation of summarized dose-response data. Stata Journal. 2006; 6:40-57.
64. Berlin JA, Longnecker MP and Greenland S. Meta-analysis of epidemiologic dose-response data. Epidemiology. 1993; 4:218-228.
65. Orsini N, Li R, Wolk A, Khudyakov P and Spiegelman D. Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software. American journal of epidemiology. 2012; 175:66-73.
66. Bagnardi V, Zambon A, Quatto P and Corrao G. Flexible meta-regression functions for modeling aggregate dose-response data, with an application to alcohol and mortality. American journal of epidemiology. 2004; 159:1077-1086.
67. Higgins JP, Thompson SG, Deeks JJ and Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003; 327:557-560.
68. Egger M, Davey Smith G, Schneider M and Minder C. Bias in meta-analysis detected by a simple, graphical test. Bmj. 1997; 315:629-634.
69. Begg CB and Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994; 50:1088-1101.
70. Duval S and Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56:455-463.