
INTRODUCTION
There are two main types of esophageal cancer, i.e., squamous cell carcinoma and adenocarcinoma [1]. Esophageal squamous cell carcinoma has a poor prognosis and the highest incidence occurs in Eastern Asia and Eastern and Southern Africa [1]. The risk factors of esophageal squamous cell carcinoma are not well characterized. While poor nutrition, low intake of fruits and vegetables and drinking hot beverages have been identified in Asian countries [1, 2], alcohol and smoking account for 90% of the cases in Western countries [1]. In Taiwan, the incidence of esophageal cancer is increasing steadily [3] and squamous cell carcinoma represents 91% of all cases in men and 76% in women [4]. Esophageal adenocarcinoma, more common in Western countries, is associated with obesity and gastroesophageal reflux disease [1, 2].
In patients with type 2 diabetes mellitus (T2DM), metformin reduces the risk of several types of cancer, including thyroid cancer [5], oral cancer [6], colon cancer [7], kidney cancer [8], bladder cancer [9], prostate cancer [10], breast cancer [11], endometrial cancer [12], ovarian cancer [13] and cervical cancer [14]. However, whether metformin may reduce the risk of esophageal cancer remains to be answered. Two previous studies concluded a null association. In the 1:10 case-control study using the UK-based General Practice Research Database, metformin did not significantly alter the risk in either the analysis of all patients (3819 cases and 38190 controls) or in patients with diabetes (370 cases and 3700 controls) [15]. While compared to those with no prior use, the adjusted odds ratio (95% confidence interval) for patients who had received metformin prescription of 1–14, 15–29 and ≥ 30 times was 0.99 (0.74–1.33), 1.01 (0.71–1.43) and 1.23 (0.92–1.65), respectively, in the analysis of all patients; and was 0.95 (0.68–1.33), 1.02 (0.69–1.50) and 1.31 (0.93–1.85), respectively, in the analysis of diabetes patients [15]. Another retrospective cohort study using the reimbursement database of the Taiwan’s National Health Insurance (NHI) estimated an adjusted hazard ratio of 0.44 (95% confidence interval: 0.07–2.61) [16].
By using the Taiwan’s NHI database, the present study further explored whether metformin use in patients with T2DM might reduce the risk of esophageal cancer. The tertile cutoffs of cumulative duration were used to evaluate a dose-response relationship, with the consideration of some infections, i.e., Helicobacter pylori (HP), hepatitis B virus (HBV), hepatitis C virus (HCV) and Epstein-Barr virus (EBV) [17–20]. Only patients with newly diagnosed diabetes and incident users of metformin were recruited to reduce the “prevalent user bias” [21]. To reduce “immortal time bias” when the outcome can not occur during the initial period of follow-up [21, 22], patients should have been prescribed antidiabetic drugs for at least two times, and those who were followed up for < 180 days were excluded. To reduce the confounding from the differences in baseline characteristics, Cox regression models incorporated with the inverse probability of treatment weighting (IPTW) using propensity score (PS) were created [23, 24] and sensitivity analyses were conducted in a matched-pair sample.
RESULTS
There were 16216 never users and 288013 ever users of metformin in the original sample (Figure 1). All baseline characteristics differed significantly, except for peripheral arterial disease, pioglitazone and EBV-related diagnoses (Table 1). Ever users were characterized by younger age, less males, higher proportions of dyslipidemia, obesity, eye disease, and tobacco abuse, lower proportions of hypertension, nephropathy, stroke, ischemic heart disease, chronic obstructive pulmonary disease, alcohol-related diagnoses, HP infection, HBV infection and HCV infection, higher proportions of use of rosiglitazone, statin, fibrate and non-steroidal anti-inflammatory drugs (NSAID), but lower proportions of using other antidiabetic medications, angiotensin converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB) and aspirin. The baseline characteristics were more comparable in the matched sample and only 6 variables (i.e., age, dyslipidemia, obesity, eye disease, insulin, and sulfonylurea) differed significantly. While examining the standardized differences, 14 of the 31 variables had values > 10% in the original sample, but none in the matched sample. Therefore, the results derived from the matched sample would be less influenced by residual confounding from the baseline characteristics.
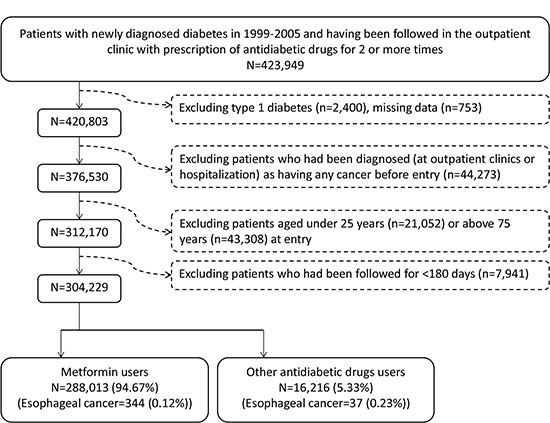
Figure 1: Flowchart showing the procedure in selecting the original sample into the study.
Table 1: Baseline characteristics between metformin never users and ever users in the original sample and the propensity score matched sample
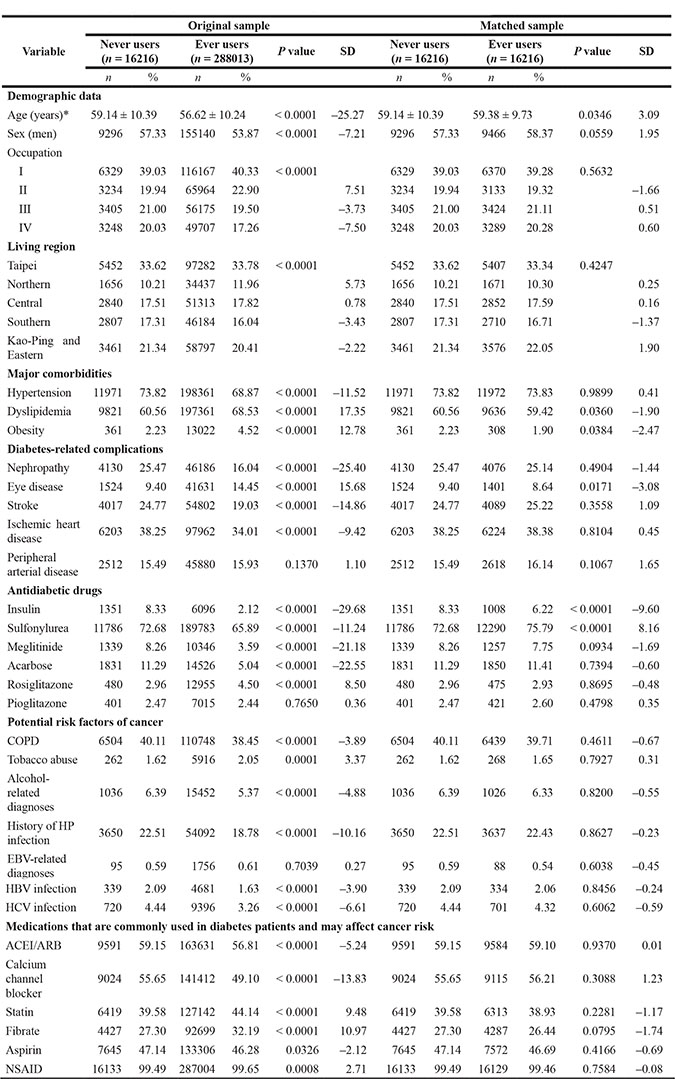
*Age is expressed as mean ± standard deviation
SD: standardized difference, COPD: chronic obstructive pulmonary disease, HP: Helicobacter pylori, EBV: Epstein-Barr virus, HBV: hepatitis B virus, HCV: hepatitis C virus, ACEI/ARB: angiotensin converting enzyme inhibitor/angiotensin receptor blocker, NSAID: non-steroidal anti-inflammatory drugs (excluding aspirin)
Table 2 shows the incidences and hazard ratios by metformin exposure. The respective number of incident esophageal cancer in ever users and never users in the original sample was 344 and 37, with respective incidence of 25.03 and 50.87 per 100,000 person-years. There was a trend of decreasing incidence with longer cumulative duration. The overall hazard ratios showed a significantly lower risk associated with metformin in either the original sample or the matched sample. When analyzed by the tertiles of cumulative duration, a reduced risk was observed mainly for the second and third tertiles, or after a cumulative duration of approximately 2 years.
Table 2: Incidences of esophageal cancer and hazard ratios by metformin exposure
Metformin use |
n |
N |
Person-years |
Incidence rate |
HR |
95% CI |
P value |
|---|---|---|---|---|---|---|---|
I. Original sample |
|||||||
Never users |
37 |
16216 |
72733.53 |
50.87 |
1.000 |
||
Ever users |
344 |
288013 |
1374345.55 |
25.03 |
0.487 |
(0.347–0.684) |
< 0.0001 |
Tertiles of cumulative duration of metformin therapy (months) |
|||||||
Never users |
37 |
16216 |
72733.53 |
50.87 |
1.000 |
||
< 21.47 |
210 |
95183 |
344813.60 |
60.90 |
1.184 |
(0.834–1.680) |
0.3455 |
21.47–46.00 |
99 |
94864 |
472599.13 |
20.95 |
0.403 |
(0.276–0.588) |
< 0.0001 |
> 46.00 |
35 |
97966 |
556932.83 |
6.28 |
0.113 |
(0.071–0.179) |
< 0.0001 |
II. Matched sample |
|||||||
Never users |
37 |
16216 |
72733.53 |
50.87 |
1.000 |
||
Ever users |
22 |
16216 |
77211.50 |
28.49 |
0.557 |
(0.329–0.944) |
0.0298 |
Tertiles of cumulative duration of metformin therapy (months) |
|||||||
Never users |
37 |
16216 |
72733.53 |
50.87 |
1.000 |
||
< 21.47 |
15 |
5355 |
19409.77 |
77.28 |
1.490 |
(0.816–2.720) |
0.1945 |
21.47–45.93 |
6 |
5344 |
26465.42 |
22.67 |
0.439 |
(0.185–1.040) |
0.0614 |
> 45.93 |
1 |
5517 |
31336.31 |
3.19 |
0.063 |
(0.009–0.460) |
0.0064 |
HR: hazard ratio, CI: confidence interval
Table 3 shows the separate effects of some infections (i.e., HP, EBV, HBV and HCV in Model I) and the joint effect of metformin and HP infection (Model II). In Model I, only HP infection was associated with a significantly higher risk. Metformin seemed to further reduce the risk in either the patients with or without HP infection (Model II).
Table 3: The effects of some infections and the joint effect of metformin and Helicobacter pylori infection on the risk of esophageal cancer in patients with type 2 diabetes mellitus
Model |
n |
N |
Person-years |
Incidence rate |
HR |
95% CI |
P value |
|---|---|---|---|---|---|---|---|
Model I. Separate effect of infection |
|||||||
History of HP infection |
|||||||
No |
268 |
246487 |
1187121.28 |
22.58 |
1.000 |
||
Yes |
113 |
57742 |
259957.80 |
43.47 |
1.493 |
(1.188–1.876) |
0.0006 |
History of EBV-related diagnoses |
|||||||
No |
378 |
302378 |
1438471.85 |
26.28 |
1.000 |
||
Yes |
3 |
1851 |
8607.23 |
34.85 |
1.280 |
(0.410–3.996) |
0.6703 |
History of HBV infection |
|||||||
No |
372 |
299209 |
1426369.10 |
26.08 |
1.000 |
||
Yes |
9 |
5020 |
20709.98 |
43.46 |
1.192 |
(0.612–2.321) |
0.6063 |
History of HCV infection |
|||||||
No |
358 |
294113 |
1402059.96 |
25.53 |
1.000 |
||
Yes |
23 |
10116 |
45019.12 |
51.09 |
1.373 |
(0.893–2.111) |
0.1486 |
Model II. Joint effect of metformin and HP infection |
|||||||
Metformin (–)/HP infection (+) |
12 |
3650 |
14896.45 |
80.56 |
1.000 |
||
Metformin (+)/HP infection (+) |
101 |
54092 |
245061.34 |
41.21 |
0.583 |
(0.319–1.064) |
0.0789 |
Metformin (–)/HP infection (–) |
25 |
12566 |
57837.07 |
43.22 |
0.694 |
(0.347–1.388) |
0.3023 |
Metformin (+)/HP infection (–) |
243 |
233921 |
1129284.21 |
21.52 |
0.389 |
(0.216–0.700) |
0.0017 |
All models were created from the original sample with adjustment for all covariates in Table 1. Follow-up started on January 1, 2006 and ended on December 31, 2011.
HR: hazard ratio, CI: confidence interval
HP: Helicobacter pylori, EBV: Epstein-Barr virus, HBV: hepatitis B virus, HCV: hepatitis C virus
DISCUSSION
The findings strongly suggested that metformin significantly reduced the risk of esophageal cancer (Tables 2 and 3). Such a protective effect was consistently observed in the original sample and the matched sample, and in a dose-response pattern (Table 2). Furthermore, HP infection was associated with an increased risk, which could be attenuated by metformin (Table 3).
The mechanisms by which metformin reduces the risk of esophageal cancer remains to be explored. In general, metformin may exert its anticancer effect through the inhibition of tumor angiogenesis [25], suppressing cancer cell metabolism [26], activation of apoptosis and autophagy [27], inhibition of mammalian target of rapamycin (mTOR) [28], immunomodulation by increasing the number of CD8+ tumor-infiltrating lymphocytes [29], and impairing one-carbon metabolism acting like an antifolate drug [30]. Some in vitro and in vivo studies supported these potential mechanisms. Metformin may inhibit esophageal cancer cell proliferation, both through an activation of 5’-adenosine monophosphate-activated protein kinase followed by the inhibition of mTOR/p70S6K/pS6 signaling, and through upregulation of USP7, a positive regulator of tumor suppressor p53 [31, 32]. Additionally, metformin blocks cell cycle in G0/G1 phase in esophageal cancer cell lines by reducing the expression of cyclin D1, Cdk4 and Cdk6 [33], and causes autophagy and apoptosis by downregulating Stat3 (signal transducer and activator of transcription 3), resulting in a reduced expression of Bcl-2 [34].
Although the UK study evaluated a dose-response relationship by using three categories of prescriptions, i.e., 1–14, 15–29 and ≥ 30, it suffered from the inherent limitations of a case-control design [15]. The previous Taiwanese study used a retrospective cohort design, but it suffered from limitations of small numbers of esophageal cancer (6 and 21 incident cases in comparator group and metformin users, respectively) and lack of sufficient power for a dose-response analysis [16]. Furthermore, both studies did not adjust for HP infection, and did not consider the effects of “prevalent user bias” and “immortal time bias” [21, 22].
The present study has several strengths. First, the diagnoses were considered from all sources of claims records including outpatient visits and hospital admission. Second, most medical co-payments can be waived by the NHI in patients with cancer, and there is a low drug cost-sharing in patients with certain conditions (e.g. low-income), veterans or prescription refills for chronic disease. Therefore, the detection rate of esophageal cancer would be less biased by social classes. Third, self-reporting bias could be reduced by the use of medical records.
Some limitations should be mentioned here. First, infection with human papillomavirus is a possible risk factor of esophageal cancer [17, 18]. However, this infection was not considered in the analysis because only 8 patients with such a diagnosis could be identified from the NHI database. Second, although none of the standardized differences had a value > 10%, the use of insulin and sulfonylurea remained statistically significant in the matched sample (Table 1). Both have been previously linked to a significantly higher risk of cancer in our patients with T2DM [35] and might potentially exert a confounding. However, their impacts should be minimal because of the following reasons: analysis after excluding insulin users did not change the results (data not shown), and a higher proportion of sulfonylurea use in ever users of metformin would only underestimate the protective effect of metformin if sulfonylurea did increase the risk of esophageal cancer. Other limitations included a lack of actual measurement data for confounders such as anthropometric factors, smoking, alcohol drinking, family history, lifestyle, nutritional status, dietary pattern, history of drinking hot beverages and genetic parameters. In addition, we could not evaluate the impact of biochemical data. Another limitation is the lack of information on the pathology, grading and staging of esophageal cancer. Because squamous cell carcinoma represents 91% and 76% of all cases of esophageal cancer in men and women, respectively, in Taiwan [4], the findings should better be applied to squamous cell carcinoma rather than to adenocarcinoma.
In summary, this is the first study that clearly shows a risk reduction of esophageal cancer associated with metformin use, especially after 2 years of its use. Furthermore, HP infection is an important risk factor and metformin may attenuate such a risk association.
MATERIALS AND METHODS
The NHI implemented in Taiwan since March 1995 is a compulsory and universal system of health insurance. It covers > 99% of Taiwan residents and has contracts with > 98% of the hospitals nationwide. The reimbursement databases are handled by the National Health Research Institutes and can be used for academic researches after proposal review and approval by an ethic review board. This study was granted with an approval number 99274.
Individuals were de-identified for the protection of privacy. Diabetes was coded 250.XX and esophageal cancer 150, based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
Figure 1 shows the procedures in selecting a cohort of patients with newly diagnosed T2DM into the study (original sample). The patients should have been diagnosed as having diabetes at an onset age of 25–74 years during the period from 1999 to 2005. Patients with diabetes mellitus diagnosed during 1996–1998 were excluded to assure a first diagnosis of diabetes after 1999, and they should have been followed up in the outpatient clinic with prescription of antidiabetic drugs for 2 or more times (n = 423949). In Taiwan, patients with type 1 diabetes can be waived of much of the co-payment after a certified diagnosis with issuance of a so-called “Severe Morbidity Card”. These patients with type 1 diabetes (n = 2400) were excluded because metformin is not indicated for them. Patients with missing data (n = 753), with a diagnosis of any cancer before entry (n = 44273), aged < 25 (n = 21052) or ≥ 75 (n = 43308) years, and followed up for < 180 days (n = 7941) were also excluded.
Cumulative duration (months) of metformin use was calculated and its tertiles were used for analyses. Demographic data of age, sex, occupation and living region, and factors that might be correlated with metformin use, diabetes severity or cancer risk were considered as potential confounders. The living region and occupation were classified as detailed elsewhere [7]. In brief, the living region was classified as Taipei, Northern, Central, Southern, and Kao-Ping/Eastern. Occupation was classified as class I (civil servants, teachers, employees of governmental or private businesses, professionals and technicians), class II (people without a specific employer, self-employed people or seamen), class III (farmers or fishermen) and class IV (low-income families supported by social welfare, or veterans).
Other confounders included 1) major comorbidities associated with diabetes mellitus: hypertension (ICD-9-CM code: 401–405), dyslipidemia (272.0–272.4) and obesity (278); 2) diabetes-related complications: nephropathy (580–589), eye disease (250.5, 362.0, 369, 366.41 and 365.44), stroke (430–438), ischemic heart disease (410–414), and peripheral arterial disease (250.7, 785.4, 443.81 and 440–448); 3) antidiabetic drugs: insulin, sulfonylurea, meglitinide, acarbose, rosiglitazone and pioglitazone; 4) potential risk factors of cancer: chronic obstructive pulmonary disease (a surrogate for smoking; 490–496), tobacco abuse (305.1, 649.0 and 989.84), alcohol-related diagnoses (291, 303, 535.3, 571.0–571.3 and 980.0), history of HP infection (defined below), diagnoses related to EBV infection (075, 710.3 and 710.4), HBV infection (070.22, 070.23, 070.32, 070.33 and V02.61) and HCV infection (070.41, 070.44, 070.51, 070.54 and V02.62); and 5) medications that are commonly used in diabetes patients and may potentially affect cancer risk: ACEI/ARB, calcium channel blocker, statin, fibrate, aspirin and NSAID (excluding aspirin). History of HP infection was defined based on one of the following two criteria: 1) having received an HP eradication therapy (detailed previously [36] and defined in brief as a combination use of proton pump inhibitors or H2 receptor blockers, plus clarithromycin, metronidazole or levofloxacin, plus amoxicillin or tetracycline, with or without bismuth, in the same prescription order for 7–14 days); and/or 2) HP infection diagnosis (041.86). The accuracy of disease diagnoses in the NHI database has been studied previously. Agreements between claim data and medical records are moderate to substantial, with Kappa values ranged from 0.55 to 0.86 [37].
Baseline characteristics between never users and ever users were compared by Student’s t test for age and by Chi-square test for other variables.
The incidence density of esophageal cancer was calculated for never users and ever users and for the tertiles of cumulative duration of metformin therapy. The numerator was the case number of incident esophageal cancer during follow-up, and the denominator was the person-years of follow-up. Follow-up started on the first day of the use of antidiabetic drugs and ended on December 31, 2011, at the time of a new diagnosis of esophageal cancer, or on the date of death or the last reimbursement record.
The baseline characteristics shown in Table 1 were used for creating PS by logistic regression, and the treatment effect was estimated by Cox regression incorporated with IPTW using the PS [23, 24]. Hazard ratios were estimated for ever versus never users and for each tertile of cumulative duration using never users as referent.
Because the baseline characteristics were imbalanced between metformin ever and never users, additional analyses were conducted in a 1:1 PS matched-pair sample (matched sample), which was created by using the Greedy 8 → 1 digit match algorithm as recommended by Parsons [38]. Because the case number of metformin never users was much smaller than the ever users, the matching was based on the case number of never users. This matching method has also been applied in our previous studies [6, 14, 39–41].
If residual systematic differences in baseline characteristics exist, the IPTW approach may not achieve unbiased estimates [42]. A quantitative method based on the calculation of standardized difference has been proposed by Austin and Stuart as a test for balance diagnostics [42]. A value of > 10% might indicate potential confounding from the variable [42]. The standardized differences for all covariates were calculated for both the original sample and the matched sample [42].
Traditional Cox regression models were created to evaluate the separate effect of infection of HP, EBV, HBV and HCV, and the joint effect of metformin and HP infection by categorizing the patients into 4 subgroups: 1) metformin (–)/HP infection (+), treated as the referent group; 2) metformin (+)/HP infection (+); 3) metformin (–)/HP infection (–); and 4) metformin (+)/HP infection (–). These models were created by setting an entry date on January 1, 2006, and followed patients without esophageal cancer before this date for 6 years until December 31, 2011.
Analyses were conducted using SAS statistical software, version 9.3 (SAS Institute, Cary, NC). P < 0.05 was considered statistically significant.
ACKNOWLEDGMENTS
The study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
CONFLICTS OF INTEREST
The author declares no conflicts of interest.
FUNDINGS
The study was supported by the Ministry of Science and Technology (MOST 103-2314-B-002-187-MY3) of Taiwan. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The publication fee of this paper is supported by the Weng Yuan Endocrine Fund.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. Cancer J Clin. 2015; 65:87–108.
2. Trevellin E, Scarpa M, Carraro A, Lunardi F, Kotsafti A, Porzionato A, Saadeh L, Cagol M, Alfieri R, Tedeschi U, Calabrese F, Castoro C, Vettor R. Esophageal adenocarcinoma and obesity: peritumoral adipose tissue plays a role in lymph node invasion. Oncotarget. 2015; 6:11203–15. doi: 10.18632/oncotarget.3587.
3. Chiang CJ, Chen YC, Chen CJ, You SL, Lai MS. Taiwan Cancer Registry Task Force. Cancer trends in Taiwan. Jpn J Clin Oncol. 2010; 40:897–904.
4. Bureau of Health Promotion. Cancer Registry Annual Report 2008. Taiwan: Department of Health, Executive Yuan, 2010. http://www.hpa.gov.tw/DOWNLOAD/Statistics/1.%E7%99%8C%E7%97%87%E7%99%BB%E8%A8%98%E5%B9%B4%E5%BA%A6%E5%A0%B1%E5%91%8A%EF%BC%88%E5%85%A8%EF%BC%89(92%E5%B9%B4%E4%BB%A5%E5%BE%8C%E8%B3%87%E6%96%99%E5%83%85%E5%90%AB%E4%BE%B5%E8%A5%B2%E7%99%8C)/Y97-%E7%99%8C%E7%97%87%E7%99%BB%E8%A8%98%E5%B9%B4%E5%BA%A6%E5%A0%B1%E5%91%8A%EF%BC%88%E5%85%A8).pdf (21 October 2014, date last accessed)
5. Tseng CH. Metformin reduces thyroid cancer risk in Taiwanese patients with type 2 diabetes. PLoS ONE. 2014; 9:e109852.
6. Tseng CH. Metformin may reduce oral cancer risk in patients with type 2 diabetes. Oncotarget. 2016; 7:2000–8. doi: 10.18632/oncotarget.6626.
7. Tseng CH. Diabetes, metformin use, and colon cancer: A population-based cohort study in Taiwan. Eur J Endocrinol. 2012; 167:409–16.
8. Tseng CH. Use of metformin and risk of kidney cancer in patients with type 2 diabetes. Eur J Cancer. 2016; 52:19–25.
9. Tseng CH. Metformin may reduce bladder cancer risk in Taiwanese patients with type 2 diabetes. Acta Diabetol. 2014; 51:295–303.
10. Tseng CH. Metformin significantly reduces incident prostate cancer risk in Taiwanese men with type 2 diabetes mellitus. Eur J Cancer. 2014; 50:2831–7.
11. Tseng CH. Metformin may reduce breast cancer risk in Taiwanese women with type 2 diabetes. Breast Cancer Res Treat. 2014; 145:785–90.
12. Tseng CH. Metformin and endometrial cancer risk in Chinese women with type 2 diabetes mellitus in Taiwan. Gynecol Oncol. 2015; 138:147–53.
13. Tseng CH. Metformin reduces ovarian cancer risk in Taiwanese women with type 2 diabetes mellitus. Diabetes Metab Res Rev. 2015; 31:619–26.
14. Tseng CH. Metformin use and cervical cancer risk in female patients with type 2 diabetes. Oncotarget. 2016; 7:59548–59555. doi: 10.18632/oncotarget.10934.
15. Becker C, Meier CR, Jick SS, Bodmer M. Case-control analysis on metformin and cancer of the esophagus. Cancer Causes Control. 2013; 24:1763–70.
16. Lee MS, Hsu CC, Wahlqvist ML, Tsai HN, Chang YH, Huang YC. Type 2 diabetes increases and metformin reduces total, colorectal, liver and pancreatic cancer incidences in Taiwanese: a representative population prospective cohort study of 800,000 individuals. BMC Cancer. 2011; 11:20.
17. Zhang DH, Zhang QY, Hong CQ, Chen JY, Shen ZY, Zhu Y. Prevalence and association of human papillomavirus 16, Epstein-Barr virus, herpes simplex virus-1 and cytomegalovirus infection with human esophageal carcinoma: a case-control study. Oncol Rep. 2011; 25:1731–8.
18. Al-Haddad S, El-Zimaity H, Hafezi-Bakhtiari S, Rajendra S, Streutker CJ, Vajpeyi R, Wang B. Infection and esophageal cancer. Ann N Y Acad Sci. 2014; 1325:187–96.
19. Xie FJ, Zhang YP, Zheng QQ, Jin HC, Wang FL, Chen M, Shao L, Zou DH, Yu XM, Mao WM. Helicobacter pylori infection and esophageal cancer risk: an updated meta-analysis. World J Gastroenterol. 2013; 19:6098–107.
20. Lee MH, Yang HI, Lu SN, Jen CL, You SL, Wang LY, Wang CH, Chen WJ, Chen CJ; R.E.V.E.A.L.-HCV Study Group. Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: a community-based long-term prospective study. J Infect Dis. 2012; 206:469–77.
21. Yang XL, Ma RC, So WY, Kong AP, Xu G, Chan JC. Addressing different biases in analysing drug use on cancer risk in diabetes in non-clinical trial settings-what, why and how? Diabetes Obes Metab. 2012; 14:579–85.
22. Suissa S. Immortal time bias in pharmaco-epidemiology. Am J Epidemiol. 2008; 167:492–9.
23. Austin PC. The performance of different propensity score methods for estimating marginal hazard ratios. Stat Med. 2013; 32:2837–49.
24. Brookhart MA, Wyss R, Layton JB, Stürmer T. Propensity score methods for confounding control in nonexperimental research. Circ Cardiovasc Qual Outcomes. 2013; 6:604–11.
25. Wang J, Li G, Wang Y, Tang S, Sun X, Feng X, Li Y, Bao G, Li P, Mao X, Wang M, Liu P. Suppression of tumor angiogenesis by metformin treatment via a mechanism linked to targeting of HER2/HIF-1α/VEGF secretion axis. Oncotarget. 2015; 6:44579–92. doi: 10.18632/oncotarget.6373.
26. Wong VK, Dong H, Liang X, Bai LP, Jiang ZH, Guo Y, Kong AT, Wang R, Kam RK, Law BY, Hsiao WW, Chan KM, Wang J, et al. Rh2E2, a novel metabolic suppressor, specifically inhibits energy-based metabolism of tumor cells. Oncotarget. 2016; 7:9907–24. doi: 10.18632/oncotarget.6934.
27. Nazim UM, Moon JH, Lee JH, Lee YJ, Seol JW, Eo SK, Lee JH, Park SY. Activation of autophagy flux by metformin downregulates cellular FLICE-like inhibitory protein and enhances TRAIL- induced apoptosis. Oncotarget. 2016; 7:23468–81. doi: 10.18632/oncotarget.8048.
28. Chae YK, Arya A, Malecek MK, Shin DS, Carneiro B, Chandra S, Kaplan J, Kalyan A, Altman JK, Platanias L, Giles F. Repurposing metformin for cancer treatment: current clinical studies. Oncotarget. 2016; 7:40767–80. doi: 10.18632/oncotarget.8194.
29. Eikawa S, Nishida M, Mizukami S, Yamazaki C, Nakayama E, Udono H. Immune-mediated antitumor effect by type 2 diabetes drug, metformin. Proc Natl Acad Sci U S A. 2015; 112:1809–14.
30. Corominas-Faja B, Quirantes-Piné R, Oliveras-Ferraros C, Vazquez-Martin A, Cufí S, Martin-Castillo B, Micol V, Joven J, Segura-Carretero A, Menendez JA. Metabolomic fingerprint reveals that metformin impairs one-carbon metabolism in a manner similar to the antifolate class of chemotherapy drugs. Aging (Albany NY). 2012; 4:480–98. doi: 10.18632/aging.100472.
31. Xu Y, Lu S. Metformin inhibits esophagus cancer proliferation through upregulation of USP7. Cell Physiol Biochem. 2013; 32:1178–86.
32. Cai X, Hu X, Tan X, Cheng W, Wang Q, Chen X, Guan Y, Chen C, Jing X. Metformin induced AMPK activation, G0/G1 phase cell cycle arrest and the inhibition of growth of esophageal squamous cell carcinomas in vitro and in vivo. PLoS One. 2015; 10:e0133349.
33. Kobayashi M, Kato K, Iwama H, Fujihara S, Nishiyama N, Mimura S, Toyota Y, Nomura T, Nomura K, Tani J, Miyoshi H, Kobara H, Mori H, et al. Antitumor effect of metformin in esophageal cancer: in vitro study. Int J Oncol. 2013; 42:517–24.
34. Feng Y, Ke C, Tang Q, Dong H, Zheng X, Lin W, Ke J, Huang J, Yeung SC, Zhang H. Metformin promotes autophagy and apoptosis in esophageal squamous cell carcinoma by downregulating Stat3 signaling. Cell Death Dis. 2014; 5:e1088.
35. Hsieh MC, Lee TC, Cheng SM, Tu ST, Yen MH, Tseng CH. The influence of type 2 diabetes and glucose-lowering therapies on cancer risk in the Taiwanese. Exp Diabetes Res. 2012; 2012:413782.
36. Tseng CH. Diabetes, insulin use and Helicobacter pylori eradication: a retrospective cohort study. BMC Gastroenterology. 2012,12:46.
37. Chang L. A study of validation on comorbidity derived from claims data [Master thesis]: National Yang-Ming University; 2004. http://etd.lib.nctu.edu.tw/cgi-bin/gs32/ymgsweb.cgi/ccd=ji3XTg/search#result (Accessed: October 26, 2015).
38. Parsons LS. Performing a 1:N case-control match on propensity score. http://www.google.com.tw/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CBsQFjAAahUKEwibi7HllcnIAhUDoJQKHVeZA9A&url=http%3A%2F%2Fwww2.sas.com%2Fproceedings%2Fsugi29%2F165–29.pdf&usg=AFQjCNFOHGWYu8E8Bn4-Bo1TUiJKtT987Q (last accessed October 17, 2015).
39. Tseng CH. Sitagliptin use and thyroid cancer risk in patients with type 2 diabetes. Oncotarget. 2016; 7:24871–9. doi: 10.18632/oncotarget.8399.
40. Tseng CH. Sitagliptin and heart failure hospitalization in patients with type 2 diabetes. Oncotarget. 2016; 7:62687–62696. doi: 10.18632/oncotarget.10507.
41. Tseng CH. Metformin reduces gastric cancer risk in patients with type 2 diabetes mellitus. Aging (Albany NY). 2016; 8:1636–49. doi: 10.18632/aging.101019.
42. Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015; 34:3661–79.