
Introduction
Breast cancer is one of the most frequent diagnosed cancers and the second most common cause of death in females around the world [1]. Neoadjuvant chemotherapy (NAC), which is known as primary or preoperative chemotherapy, is a treatment option for breast cancer patients with large primary tumors or locally advanced disease [2].NAC significantly contributes in controlling locoregional disease and improves the rate of breast conservation[3, 4]. A total of 23% to 32% patients with proven metastatic axillary lymph nodes exhibited no residual tumor cells in their lymph node after NAC [5, 6]. The residual of axillary lymph node disease after NAC is a prognostic marker for local recurrence and survival [7]. Axillary lymph node dissection (ALND) is the standard procedure for axillary lymph node staging and local control in breast cancer patients. Sentinel lymph node biopsy (SLNB) was also used as a method to obtain information on the status of axillary lymph nodes[8]. Current research aimed to identify novel and non-invasive nodal staging techniques with high sensitivity and negative predictive value (NPV) that could replace SLNB [9-13].
Although the optimal approach for the staging of axillary lymph nodes in patients receiving NAC remains unclear, axillary ultrasound (AUS) is commonly used in clinical practice in staging and following-up of regional lymph nodes. AUS has a sensitivity of 50%–70% and specificity of 87%–95% for breast cancer nodal metastasis [14-17].The findings of abnormal nodes on AUS after NAC correlated with pathological residual positive nodes at surgery [18]. The Z1071 trial showed that 71.8% of patients who had suspicious nodes identified by AUS had residual node-positive disease after completing NAC [19].The current study demonstrates the potential use of AUS after completing NAC before surgery to evaluate residual nodal disease. However, the accuracy of different number of cycles of NAC remains unclear. Therefore, the aim of this study was to evaluate the accuracy of AUS in detecting axillary lymph node metastases after different numbers of chemotherapy cycles.
Results
Clinic–pathological features with the different chemotherapy cycle
We analyzed a total of 656 patients who received NAC and had subsequent ALND in our institute. The patients were divided into three groups based on the cycles of NAC: the two-cycle (n = 229), four-cycle (n = 201), and six-cycle (n = 226) subgroups. Table 1 describes the clinic–pathological features of the three groups. Age, menopausal status, clinical N stage, chemotherapy regimens, histological type, pathological tumor size, and pathological N stage, ER, HER2, Ki67, and the subtype of breast cancer were not significantly different among the three groups. The proportion of patients with T4 tumors at primary before NAC in the six-cycle subgroup (p < 0.001) was higher than that of patients in the two- or four-cycle subgroup. The patients in the four- or six-cycle subgroup achieved a more complete or partial response (CR/PR) to NAC and exhibited more significant shrinkage of tumors than patients in the two-cycle subgroup (p < 0.001). Comparison of the clinical–pathological features of the three groups indicates that the patients in six-cycle group have larger tumors at the primary but have better response to NAC than the other groups.
Table 1: Clinic-pathological features with the different chemotherapy cycle
Variables |
Total (656) |
2-cycle (229) |
4-cycle (201) |
6-cycle (226) |
P-value |
Age(years) |
0.158 |
||||
mean±SD |
49.6± 9.8 |
50± 10.3 |
50± 9.49 |
49± 9.54 |
|
Menopausal status |
0.69 |
||||
Pre-menopausal |
346 (52.7%) |
120 (52.4%) |
102 (50.7%) |
124 (54.9%) |
|
Post-menopausal |
310 (47.3%) |
109 (47.6%) |
99 (49.3%) |
102 (45.1%) |
|
clinical T stage before NAC |
<0.001 |
||||
cT1-2 |
386 (58.8%) |
130 (56.8%) |
133 (66.2%) |
123 (54.4%) |
|
cT3 |
203 (30.9%) |
83 (36.2%) |
54 (26.9%) |
66 (29.2%) |
|
cT4 |
67 (10.2%) |
16 (7.0%) |
14 (7.0%) |
37 (16.4%) |
|
clinical N stage before NAC |
0.413 |
||||
cN0 |
118 (18.0%) |
42 (18.3%) |
41 (20.4%) |
35 (15.5 %) |
|
≥cN1 |
538 (82.0%) |
187 (81.7%) |
160 (79.6%) |
191 (84.5%) |
|
clinical stage |
0.211 |
||||
IIa-IIb |
280 (42.7%) |
99 (43.2%) |
94 (46.8%) |
87 (38.5%) |
|
IIIa-IIIc |
376 (57.3%) |
130 (56.8%) |
107 (53.2%) |
139 (61.5%) |
|
Responseto chemotherapy |
<0.001 |
||||
CR |
41 (6.3%) |
9 (3.9%) |
15 (7.5%) |
17 (7.5%) |
|
PR |
323 (49.2%) |
91 (39.7%) |
108 (53.7%) |
124 (54.9%) |
|
SD |
261 (39.8%) |
118 (51.5%) |
70 (34.8%) |
73 (32.3%) |
|
PD |
31 (4.7%) |
11 (4.8%) |
8 (4.0%) |
12 (5.3%) |
|
Chemotherapy regimens |
0.304 |
||||
T and (or) E regimens |
606 (92.4%) |
215 (93.9%) |
181 (90.0%) |
210 (92.9%) |
|
Others |
50 (7.6%) |
14 (6.1%) |
20 (10.0%) |
16 (7.1%) |
|
Histological type |
0.029 |
||||
IDC |
544 (83.9%) |
192 (83.8%) |
174 (86.6%) |
178 (78.8%) |
|
ILC |
24 (3.7%) |
11 (4.8%) |
7 (3.5%) |
6 (2.7%) |
|
Others |
88 (13.4%) |
26 (11.4%) |
20 (10%) |
42 (18.6%) |
|
Estrogen receptor |
0.189 |
||||
Negative |
195 (29.7%) |
74 (32.3%) |
59 (29.4%) |
62 (27.4%) |
|
Positive |
461 (70.3%) |
155 (67.7%) |
142 (70.6%) |
164 (72.6%) |
|
Progesterone receptor |
0.001 |
||||
Negative |
317 (48.3%) |
94 (41%) |
91 (45.3%) |
132 (58.4%) |
|
Positive |
339 (51.7%) |
135 (59%) |
110 (54.7%) |
94 (41.6%) |
|
Her2/Neu |
0.783 |
||||
Negative |
561 (85.5%) |
197 (86%) |
169 (84.1%) |
195 (86.3%) |
|
Positive |
95 (14.5%) |
32 (14.0%) |
32 (15.9%) |
31 (13.7%) |
|
Ki-67 levels |
0.082 |
||||
≤14% |
198 (30.2%) |
58 (25.3%) |
61 (30.3%) |
79 (35%) |
|
>14% |
458 (69.8%) |
171 (74.7%) |
140 (69.7%) |
147 (65%) |
|
Breast cancer subtype |
0.492 |
||||
Luminal A |
152 (23.2%) |
47 (20.5 %) |
46 (22.9%) |
59 (26.1%) |
|
Luminal B |
326 (49.7%) |
117 (51.1%) |
103 (51.2%) |
106 (46.9%) |
|
Her2-enriched |
63 (9.6%) |
20 (8.7%) |
22 (10.9%) |
21 (9.3%) |
|
TNBC |
115 (17.5%) |
45 (19.7%) |
30 (14.9%) |
40 (17.7%) |
|
Pathological tumor size |
0.062 |
||||
ypT0 |
53 (8.1%) |
9 (3.9%) |
19 (9.5%) |
25 (11.1%) |
|
ypT1 |
185 (28.2%) |
58 (25.3%) |
55 (27.4%) |
72 (31.9%) |
|
ypT2 |
311 (47.4%) |
126 (55.0%) |
96 (47.8%) |
89 (39.4%) |
|
ypT3-T4 |
107 (16.3%) |
36 (15.7%) |
31 (15.4%) |
40 (17.7%) |
|
Pathological N stage |
0.213 |
||||
pN0 |
155 (23.6%) |
53 (23.1%) |
56 (27.9%) |
46 (20.4%) |
|
pN1 |
178 (27.1%) |
59 (25.8%) |
49 (24.4%) |
70 (31.0%) |
|
pN2 |
149 (22.7%) |
47 (20.5%) |
51 (25.4%) |
51 (22.6%) |
|
pN3 |
174 (26.5%) |
70 (30.6%) |
45 (22.4%) |
59 (26.1%) |
NAC, neoadjuvant chemotherapy;TNBC,triple-negative breast cancer;
CR, complete response; PR, partial response;SD,stable disease;PD,progressive disease;
T, paclitaxel or docetaxel; E, anthracylines;
IDC, invasive ductal cancer;ILC, invasive lobular cancer.
The accuracy of AUS after different cycles of NAC
Table 2 shows that the sensitivity of AUS in determining nodal involvement was 80.2% (95% CI: 74.3%-86.2%) in the two-cycle NAC group with a specificity of 61.4% (95% CI: 48.8%-74.0%). The accuracy was 75.5% (95% CI: 70.0%-81.1%). The positive likelihood ratio (+LR) was 2.07 (95% CI: 1.49-2.91), and the negative likelihood ratio (-LR) was 0.32 (95% CI: 0.22-0.46). The positive predictive value (PPV) and negative predictive value (NPV) were 86.3% (95% CI: 80.9%-91.6%) and 50.7% (95% CI: 38.9%-62.5%), respectively. The diagnostic odds ratio (DOR) was 6.46 (95% CI: 3.36-12.4). In the four-cycle group, the sensitivity was 69.7% (95% CI: 62.2%-77.1%), specificity was 66.1% (95% CI: 53.7%-78.5%), accuracy was 68.7% (95% CI: 62.2%-75.1%), +LR was 2.06 (95% CI: 1.40-3.00), -LR was 0.45 (95% CI: 0.34-0.63), PPV was 84.2% (95% CI: 77.64%-90.7%), NPV was 46.3% (95% CI: 34.8%-56.2%) and DOR was 4.47 (95% CI: 2.32-8.62). In the six-cycle group, the sensitivity was 56.7% (95% CI: 49.5%-64%), the specificity was 75.0% (95% CI: 62.8%-87.2%), accuracy was 60.6% (95% CI: 54.2%-67.0%), +LR was 2.22 (95% CI: 1.37-3.77), -LR was 0.58 (95% CI: 0.46-0.73), PPV was 89.4% (95% CI: 83.7%-95.1%), NPV was 31.3% (95% CI: 23.3%-40.4%) and DOR was 3.83 (95% CI: 1.863-7.86). As the number of cycles of chemotherapy increased, the sensitivity, DOR and NPV of AUS dramatically decreased and the false negative rate increased.
Table 2: The accuracy of AUS during different cycles of NAC
2cycle (n= 229) |
4cycle (n= 201) |
6cycle (n= 226) |
total (n= 656) |
|
sensitivity (95%-CI) |
80.2% (74.3%-86.2%) |
69.7% (62.2%-77.1%) |
56.7% (49.5%-64%) |
68.7% (64.6%-72.8%) |
specificity (95%-CI) |
61.4% (48.8%-74.0%) |
66.1% (53.7%-78.5%) |
75.0% (62.8%-87.2%) |
67.1% (59.8%-74.3%) |
accuracy (95%-CI) |
75.5% (70.0%-81.1%) |
68.7% (62.2%-75.1%) |
60.6% (54.2%-67.0%) |
68.3 (64.7%-71.9%) |
+LR (95%-CI) |
2.07 (1.49-2.91) |
2.06 (1.40-3.00) |
2.22 (1.37-3.77) |
2.08 (1.66-2.62) |
-LR (95%-CI) |
0.32 (0.22-0.46) |
0.45 (0.34-0.63) |
0.58 (0.46-0.73) |
0.47 (0.39-0.55) |
DOR (95%-CI) |
6.46 (3.36-12.4) |
4.47 (2.32-8.62) |
3.83 (1.863-7.86) |
4.43 (3.06-6.53) |
PPV (95%-CI) |
86.3% (80.9%-91.6%) |
84.2% (77.64%-90.7%) |
89.4% (83.7%-95.1%) |
86.5% (83.1%-89.9%) |
NPV (95%-CI) |
50.7% (38.9%-62.5%) |
46.3% (34.8%-56.2%) |
31.3% (23.3%-40.4%) |
40.8% (35.1%-47.0%) |
+LR, positive linkhood ratios; -LR, negative linkhood ratios; DOR, diagnostic odds ratio;
PPV, positive predictive value; NPV, negative predictive value.
False-negative AUS
Among the 656 patients, 262 patients exhibited normal findings in AUS after NAC. The 262 patients with negative AUS were examined. The patients were divided into two groups based on the pathological examination of the lymph nodes: the true-negative AUS group and the false-negative AUS group. Out of the 262 patients with negative AUS, 154 patients had a false-negative ultrasound (55.6%). These patients were found to have positive nodes after ALND. We compared the tumor characteristics between the true-negative and false-negative groups, and the results are summarized in Table 3. Age, histological type, menopausal status, nodal status, chemotherapy regimens, PR, HER2, were not significant in the two groups, which were excluded from further consideration. The clinical T stage (p < 0.01), cycles of chemotherapy (p = 0.018), pathological T stage (p < 0.001), ER status (p = 0.003), Ki67 (p = 0.034), and the subtype of breast cancer (p = 0.028) after NAC was significantly different between the two groups.
Table 3: Differences in patient and tumor characteristics between false-negative and true-negative axillary ultrasound
Variables |
N (%) (262) |
true negative (108) |
false negative (154) |
P-value |
Age(years) |
0.916 |
|||
≤50 |
140(53.8%) |
58(53.7%) |
82(53.5%) |
|
>50 |
122(46.2%) |
50(46.3%) |
72(46.5%) |
|
Menopausal status |
0.383 |
|||
Pre-menopausal |
148(56.5%) |
58(53.7%) |
90(58.5%) |
|
Post-menopausal |
114(43.5%) |
50(46.3%) |
64(41.5%) |
|
clinical T stage before NAC |
<0.01 |
|||
cT1-T2 |
151(57.6%) |
73(67.6%) |
78(50.6%) |
|
cT3-T4 |
111(42.4%) |
35(32.4%) |
76(49.4%) |
|
clinical N stage before NAC |
0.099 |
|||
cN0 |
86(32.8%) |
42(38.9%) |
44(28.6%) |
|
≥cN1 |
176(67.2%) |
66(61.1%) |
110(71.4%) |
|
Response to chemotherapy |
0.141 |
|||
CR |
29(11.1%) |
15(13.9%) |
14(9.1%) |
|
PR |
146(55.7%) |
65(60.2%) |
81(52.6%) |
|
SD |
77(29.4%) |
26(24.1%) |
51(33.1%) |
|
PD |
10(3.8%) |
2(1.9%) |
8(5.2%) |
|
Chemotherapy regimens |
0.305 |
|||
Include T and (or) E regimens |
242(92.4%) |
102(94.5%) |
140(90.9%) |
|
Others |
20(7.6%) |
6(5.5%) |
14(9.1%) |
|
The chemotherapy cycles before surgery |
0.018 |
|||
2-cycle |
69(26.3%) |
35(32.4%) |
34(22.1%) |
|
4-cycle |
81(30.9%) |
38(35.2%) |
43(27.9%) |
|
6-cycle |
112(42.7%) |
35(32.4%) |
77(50.0%) |
|
Histological type |
0.714 |
|||
IDC |
169(64.5%) |
69(63.9%) |
100(64.9%) |
|
Others |
93(35.5%) |
39(36.1%) |
54(35.1%) |
|
Estrogen receptor |
0.003 |
|||
Negative |
72(27.5%) |
40(37.0%) |
32(20.8%) |
|
Positive |
190(72.5%) |
68(63.0%) |
122(79.2%) |
|
Progesterone receptor |
0.685 |
|||
Negative |
130(47.8%) |
55(50.9%) |
75(48.7%) |
|
Positive |
132(52.2%) |
53(49.1%) |
79(51.3%) |
|
Her2/Neu |
0.117 |
|||
Negative |
225(86.1%) |
88(81.5%) |
137(89.0%) |
|
Positive |
37(13.9%) |
20(18.5%) |
17(11.0%) |
|
Ki-67 levels |
0.034 |
|||
≤14% |
84(32.1%) |
27(25.0%) |
57(37.0%) |
|
>14% |
178(67.9%) |
81(75.0%) |
97(63.0%) |
|
Breast cancer subtype |
0.028 |
|||
Luminal A |
66(25.2%) |
20(13.0%) |
46(30.0%) |
|
Luminal B |
131(50.0%) |
53(49.1%) |
78(50.6%) |
|
Her2-enriched |
22(8.4%) |
9(8.3%) |
13(8.4%) |
|
TNBC |
43(16.4%) |
26(24.1%) |
17(11.0%) |
|
Pathological tumor size |
<0.001 |
|||
ypT0 |
32(12.2%) |
18(16.7%) |
14(9.1%) |
|
ypT1 |
84(32.1%) |
42(38.9%) |
42(27.3%) |
|
ypT2 |
112(42.7%) |
45(41.7%) |
67(43.5%) |
|
ypT3-T4 |
34(13.0%) |
3(2.8%) |
31(20.1%) |
Univariate and multivariate analyses are summarized in Table 4. Both the univariate and multivariate analyses revealed that high number of cycles of NAC (p = 0.008) and large tumor size (p = 0.009) were associated with having a false-negative AUS for patients with normal AUS findings after NAC. Compared with the two-cycle group, patients with normal AUS findings after six cycles of NAC were more likely to find lymph nodes with residual tumor cells in pathologic examination. However, no significant difference was observed between the two-cycle group and the four-cycle group.
Table 4: Univariate and multivariate associations between tumor characteristics and false-negative axillary ultrasound
Univariate analysis |
Multivariate analysis |
|||||
Characteristics |
HR |
95%CI |
P-value |
HR |
95%CI |
P-value |
Primary Clinical T stage before NAC |
||||||
T3 and T4 vs T1 and T2 |
2.032 |
1.218-3.391 |
0.007 |
1.509 |
0.855-2.663 |
0.155 |
Number of NAC |
||||||
4-cycle vs 2-cycle |
1.224 |
0.643-2.329 |
0.538 |
1.147 |
0.580-2.267 |
0.694 |
6-cycle vs 2-cycle |
2.173 |
1.17-4.025 |
0.014 |
2.505 |
1.270-4.941 |
0.008 |
Pathological tumor size |
||||||
>2cm vs ≤2cm |
2.107 |
1.276-3.479 |
0.004 |
2.160 |
1.217-3.834 |
0.009 |
Estrogen receptor |
||||||
positive vs negative |
2.334 |
1.34-4.06 |
0.003 |
5.000 |
0.839-29.804 |
0.077 |
Ki-67 levels |
||||||
>14% vs ≤14% |
0.552 |
0.32-0.951 |
0.032 |
0.755 |
0.27-2.115 |
0.593 |
Breast cancer subtype |
||||||
Luminal B vs Luminal A |
0.64 |
0.341-1.202 |
0.165 |
0.765 |
0.239-2.453 |
0.652 |
Her2-enriched vs Luminal A |
0.628 |
0.231-1.705 |
0.361 |
3.751 |
0.442-31.858 |
0.226 |
TNBC vs Luminal A |
0.284 |
0.127-0.636 |
0.002 |
1.643 |
0.212-12.744 |
0.635 |
Association of AUS findings with pathologic findings for six-cycle subgroup
Of the 112 patients with normal findings assessed by AUS in the six-cycle group, 33 patients (29.5%, 95% CI: 21.0%-37.9%) was pN0, 38 patients (33.9%, 95% CI: 25.2%-42.7%) was pN1, 41 patients (36.6%, 95% CI: 27.7%-45.5%) have more than three metastasized nodes. In comparison, 113 patients who had suspicious nodes identified by AUS, 12 patients (10.6%, 95% CI: 4.9%-16.3%) was pN0, 32 patients (28.3%, 95% CI: 20.0%-36.6%) was pN1, 69 patients (61.1%, 95% CI: 52.1%-70.1%) were found to have more than three metastasized nodes. The patients with normal lymph nodes on AUS examinations after six cycles of NAC have few positive nodes than patients with suspicious findings (p < 0.001).
Discussion
Our data suggests that as the number of cycles of chemotherapy increased, the sensitivity, DOR and NPV of AUS dramatically decreased and the false negative rate increased. For patients exhibited normal findings in AUS after NAC, high number of cycles of NAC and large tumor size were associated with having a false-negative AUS. The patients with normal lymph nodes on AUS examinations after six cycles of NAC have a lower nodal burden than patients with suspicious findings (p < 0.001).
The Z0011 trial determined that dissecting the axillary in the presence of one to two positive SLN is not beneficial, which indicates that conducting an extensive surgery in the axillary does not improve the outcome [20]. We aim to identify a novel and non-invasive nodal staging technique with high sensitivity and NPV that could replace SLNB. The diagnostic performance of magnetic resonance imaging (MRI) in assessing axillary nodal staging and the response to NAC in breast cancer patients is promising because its NPV approaches the NPV of SLNB [21].However, the cost of MRI is high, and it is not always available. Thus, this approach is not easily accepted by patients. AUS is non-invasive, widely available, low-cost, and commonly used in clinical practice. The SOUND trial was designed to determine whether surgical staging method could be replaced with an imaging method of staging the axillary that can diagnose relevant nodal involvement and replace SLNB [22]. Patients with either negative cytology of a single suspicious lymph node or with negative ultrasound of the axillary will be randomly eligible to undergo SLNB±axillary dissection group or no axillary surgical group. This trial is still ongoing, and the results are not yet reported [22].
Our results suggest that AUS is a useful imaging modality to assess the axillary response to chemotherapy regimens and the status of axillary lymph node for patients with four cycles of NAC. In addition, the sensitivity of AUS with two cycles of NAC reached 80.2%, which is as high as that of MRI [21]. However, when six cycles of NAC were adopted, the sensitivity decreased from 80.2% to 56.7%. After patients completed six cycles of NAC, the sensitivity of AUS decreased and the false-negative rate (FNR) reached 43.3%, which means that almost one in two persons with normal findings in AUS will be misdiagnosed. The confirmation whether the high FNR in this subgroup can triage patients for SLNB or evaluate the status of axillary lymph node accurately is unclear. Although the FNR is relative high for patients who completed six cycles of NAC, the overall nodal burden of disease for patients with normal findings on AUS is low with a few positive nodes ( < four positive nodes in 75.3% of patients with normal lymph nodes). Basing on the results of Z1071 study, patients with normal lymph nodes in the AUS examination have a significantly lower likelihood of having residual disease[19]. Moreover, the normalized lymph node morphology on ultrasound after NAC was correlated with high pathological complete response (pCR) rates [23]. Thus, despite the high FNR of AUS, clinicians can still employ ultrasound to estimate the status of the axillary lymph node after six cycles of neoadjuvant treatment. However, another imaging modality with better sensitivity and specificity, such as positron emission tomography with computed tomography (PET/CT) or MRI, should be combined with AUS to identify patients who have clinically negative axillary after complete neoadjuvant treatment and who want to undergo axillary conservation surgery after completing six cycles of NAC [24-27].
M. Moormanet al. noted that young patients with large tumors and had lymph vascular invasion were more likely to exhibit lymph nodes with residual tumor cells in pathologic examination when the AUS were normal prior to surgery[28].The results of univariate and multivariate analyses about the false-negative AUS in this work suggest that completing six cycles of NAC is probably one of the factors that affect the prognosis of patients. The treatment effect in lymph nodes may result in the fibrosis and apoptosis of tumor cells, which may either cause ambiguous morphologic changes on imaging or not. AUS that depicts lymph nodes with metastatic disease is based on morphologic criteria and size. Thus, changes in size and morphologic causes difficulties in identifying suspicious lymph nodes. Although completing six cycles of NAC obtained a better response, the axillary pathologic complete response (pCR) was not high. A study from the Netherlands suggests that only 20% of the patients with metastasis prior to NAC achieved an axillary pCR[29]. The false-negative AUS was high in tumors ≥ 2cm after neoadjuvant treatment. Large tumor size may indicate high tumor burden. A false-negative ultrasound more likely occurs in patients with large tumors because of the high pretest probability of metastatic disease; thus, a significant number of small axillary metastases may be missed[30]. Patients with the pCR of metastatic lymph nodes were reported to be more likely to have better prognosis despite having residual primary tumors[31].The risk of local recurrence increases with the number of residual positive nodes after NAC[32]. Previous studies suggest that radiologic complete response has similar survival outcomes and recurrence-free survival to patients with pCR[33]. Our data shows that AUS is useful to evaluate the status of axillary lymph nodes with good sensitivity and specificity after NAC. However, further analysis is status necessary to determine whether AUS can replace SLNB in obtaining information on the status of axillary lymph nodes and identify patients with positive nodes as candidates for extensive surgical procedures. Limitations exist our study. Not all patients consented to the completion of ALND or some patients underwent AUS examination before surgery, thus could not be included in the analysis and decreasing our evaluable cohort. The criterion used for patients to receive NAC differs from others with a cortical thickness>3 mm with or without palpable axillary lymph node. Therefore, the criteria used for analyzing suspicious nodes mainly depend on the change of morphology in our institute.
Conclusions
Our data indicate that preoperative AUS is a potentially useful imaging modality to predict the pathologic status of the axillary with four cycles of NAC, whereas the FNR is very high for patients who received six cycles. Although the accuracy for patients who completed six cycles of NAC is significantly lower than those who underwent four cycles of NAC, the overall nodal burden of disease for patients with normal findings on AUS is low. Clinicians can still choose to employ ultrasound to estimate the status of axillary lymph node after six cycles of neoadjuvant treatment. However, radiologists should focus on evaluating the status of axillary lymph nodes for patients with large tumors and those who completed six cycles of NAC. Another imaging modality with better sensitivity and specificity, such as PET/CT or MRI, should be combined with AUS for patients who want to undergo axillary conservation surgery after completing six cycles of NAC.
Patients and Methods
Patient population
From January 2008 to October 2015, we retrospectively analyzed 967 consecutive breast cancer patients who received NAC and 656 patients were selected in this retrospective study. 311 patients were excluded from our study, including 69 patients whose NAC received outside of our institution, 23 patients with inflammatory breast cancer, 97 patients have no preoperative AUS, 47 patients not underwent ALND, 33 patients surgery in another institute and 42 patients received more than six cycles of NAC (Figure 1). The indications for NAC were primary tumors greater than 3 cm and/or with axillary lymph node metastasis and no evidence of distant metastases. All the patients included in the study met the following inclusion criteria: (1) All patients had histologically proven invasive carcinoma by core biopsy prior to commencing primary chemotherapy. (2)No patient had detectable metastatic disease before primary chemotherapy was instituted.(3)Preoperative AUS was performed in each patient.(4) All the patients underwent NAC and breast surgery plus axillary lymph node dissection (Level I and Level II)at our institution.(5) At least 15 lymph nodes were examined for pathological diagnosis. (6) None of the patients previously received neoadjuvant therapy. Informed consent was obtained from all the patients above and research protocol for this study was approved by the Ethics Committees at the Tianjin Medical University Cancer Institute and Hospital.
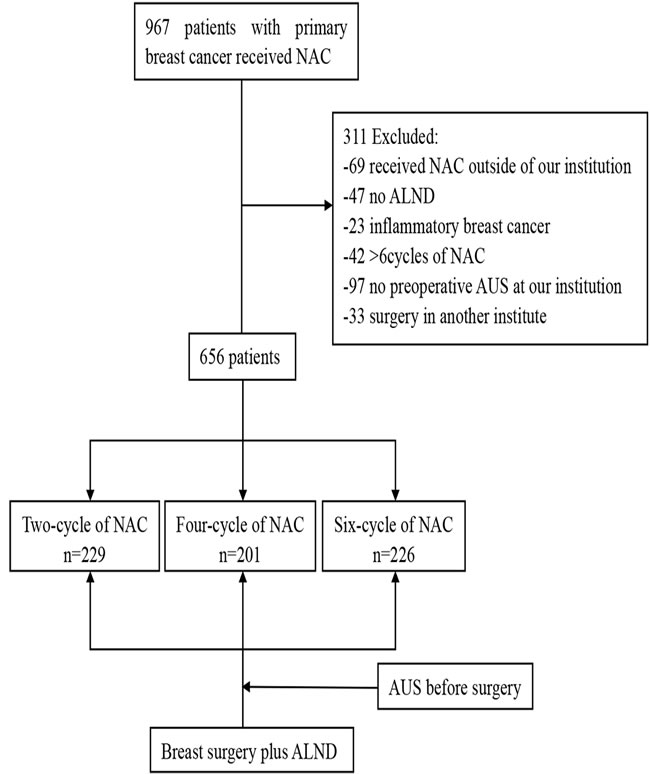
Figure 1: Study Flow chart
Ultrasound imaging protocol
The patients underwent both the breast and AUS for initial staging at presentation using the ultrasound machine Legiq E9 (General Electric Co., USA) with 6-15 MHz linear transducer in our institute. Two experienced radiologists independently analyzed the images according to the classification of the American College of Radiology BI-RADS system (2003). Axillary lymph nodes were assessed by their shape and the morphology of the cortex. A lymph node was classified as suspicious if its cortical thickness was >3 mm or if it had an irregular nodular cortex and/or a diminished or absent hilum. Since the large number of patients who are waiting in line to underwent the core biopsy test, most patients with tumors greater than 3 cm gave up the test for suspicious metastasis lymph nodes and received NAC directly. Only a few patients with tumors less than 3 cm underwent core biopsy for suspicious metastasis lymph nodes. AUS was repeated before surgery.
NAC and clinic-pathologic features
Most of the patients received anthracycline with or without taxane-based (epirubicin, cyclophosphamide, and paclitaxel, or epirubicin and paclitaxel) chemotherapy every three weeks for at least two cycles. The regimen and cycles of NAC were under the discretion of the treating medical oncologist. The responses of tumors to NAC were evaluated by RECIST 1.1 criteria [34]. All the criteria were applied in measuring the primary tumor only. Nodal metastases were not considered.
All the pathological specimens of the patients before and after NAC were microscopically reviewed. Histological type and biomarkers were diagnosed using specimens obtained after the modified radical mastectomy. Immunohistochemical staining for estrogen receptor (ER) and progesterone receptor (PR), as well as HER2, was performed. ER and PR were considered positive if nuclei stained>1% [35]. HER2 status was assessed by scoring the intensity of membrane staining using immunohistochemistry. Tumors with a score of 3+ (strong homogeneous staining) or with a >2.2-fold increase in HER2 gene amplification, which was determined by fluorescence in situ hybridization, were considered HER2-positive.Molecular subtypes were categorized into four subgroups as follows: luminal A, ER positive and/or PR positive, HER2 negative, and Ki-67≤14%; luminal B, ER positive and/or PR positive, HER2 positive and/or Ki-67 > 14%; HER2-enriched, ER negative, PR negative and HER2 3+; triple-negative breast cancer (TNBC), ER-negative, PR-negative and HER2-negative.
Statistical analysis
The differences in the characteristics between patients who received different cycles of NAC from the analysis were tested using the t-statistic or F-statistic for continuous variable and χ2statistics or Kruskal-Wallis H test for categorical variables. Sensitivity (the proportion of patients with ypN+ who had a positive pre-op AUS) and specificity (the proportion of patients with ypN- who had a negative pre-op AUS) were calculated for AUS with the final pathologic findings as gold standard. The method that uses AUS was assessed by determining the positive and negative likelihood ratios. Multivariate logistic regression was used to determine the factors associated with a false-negative event. All the statistical tests were two-sided, and P < 0.05 was considered significant. SPSS software version 17.0 was utilized for the analysis.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81372843, No. 81472472 and No. 81502518) and the National Key Clinical Specialist Construction Programs of China (No. 2013-544).
Conflicts of interest
The authors have no conflict of interest or financial ties to disclose.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81372843, No. 81472472 and No. 81502518) and the National Key Clinical Specialist Construction Programs of China (No. 2013-544).
References
1. Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M, MacIntyre MF, Allen C, Hansen G, Woodbrook R, Wolfe C, Hamadeh RR, Moore A, Werdecker A, et al. The Global Burden of Cancer 2013. JAMA Oncology. 2015; 1:505.
2. Kaufmann M, von Minckwitz G, Mamounas EP, Cameron D, Carey LA, Cristofanilli M, Denkert C, Eiermann W, Gnant M, Harris JR, Karn T, Liedtke C, Mauri D, et al. Recommendations from an International Consensus Conference on the Current Status and Future of Neoadjuvant Systemic Therapy in Primary Breast Cancer. Annals of Surgical Oncology. 2011; 19:1508-1516.
3. Redden MH and Fuhrman GM. Neoadjuvant Chemotherapy in the Treatment of Breast Cancer. Surgical Clinics of North America. 2013; 93:493-499.
4. Untch M, Konecny GE, Paepke S and von Minckwitz G. Current and future role of neoadjuvant therapy for breast cancer. The Breast. 2014; 23:526-537.
5. Mieog JS, van der Hage JA and van de Velde CJ. Neoadjuvant chemotherapy for operable breast cancer. The British journal of surgery. 2007; 94:1189-1200.
6. Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A, Margolese RG, Hoehn JL, Vogel VG, Dakhil SR, Tamkus D, King KM, Pajon ER, et al. Preoperative Chemotherapy: Updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. Journal of Clinical Oncology. 2008; 26:778-785.
7. Al-Hilli Z, Hieken TJ and Boughey JC. Axillary Ultrasound in the Management of the Newly Diagnosed Breast Cancer Patient. The Breast Journal. 2015; 21:634-641.
8. Reintgen M, Kerivan L, Reintgen E, Swaninathan S and Reintgen D. Breast Lymphatic Mapping and Sentinel Lymph Node Biopsy: State of the Art: 2015. Clin Breast Cancer. 2016.
9. Schaefgen B, Mati M, Sinn HP, Golatta M, Stieber A, Rauch G, Hennigs A, Richter H, Domschke C, Schuetz F, Sohn C, Schneeweiss A and Heil J. Can Routine Imaging After Neoadjuvant Chemotherapy in Breast Cancer Predict Pathologic Complete Response? Ann Surg Oncol. 2016; 23:789-795.
10. Liu Q, Wang C, Li P, Liu J, Huang G and Song S. The Role of (18)F-FDG PET/CT and MRI in Assessing Pathological Complete Response to Neoadjuvant Chemotherapy in Patients with Breast Cancer: A Systematic Review and Meta-Analysis. Biomed Res Int. 2016; 2016:3746232.
11. Hyun SJ, Kim EK, Moon HJ, Yoon JH and Kim MJ. Preoperative axillary lymph node evaluation in breast cancer patients by breast magnetic resonance imaging (MRI): Can breast MRI exclude advanced nodal disease? Eur Radiol. 2016.
12. Fukuda T, Horii R, Gomi N, Miyagi Y, Takahashi S, Ito Y, Akiyama F, Ohno S and Iwase T. Accuracy of magnetic resonance imaging for predicting pathological complete response of breast cancer after neoadjuvant chemotherapy: association with breast cancer subtype. SpringerPlus. 2016; 5:152.
13. Schipper RJ, Moossdorff M, Beets-Tan RGH, Smidt ML and Lobbes MBI. Noninvasive nodal restaging in clinically node positive breast cancer patients after neoadjuvant systemic therapy: A systematic review. European Journal of Radiology. 2015; 84:41-47.
14. Yamashita M, Hovanessian-Larsen L and Sener SF. The role of axillary ultrasound in the detection of metastases from primary breast cancers. The American Journal of Surgery. 2013; 205:242-245.
15. Ahn JH, Son EJ, Kim JA, Youk JH, Kim EK, Kwak JY, Ryu YH and Jeong J. The role of ultrasonography and FDG-PET in axillary lymph node staging of breast cancer. Acta Radiologica. 2010; 51:859-865.
16. Swinson C, Ravichandran D, Nayagam M and Allen S. Ultrasound and fine needle aspiration cytology of the axilla in the pre-operative identification of axillary nodal involvement in breast cancer. European Journal of Surgical Oncology (EJSO). 2009; 35:1152-1157.
17. Farrell TPJ, Adams NC, Stenson M, Carroll PA, Griffin M, Connolly EM and O’Keeffe SA. The Z0011 Trial: Is this the end of axillary ultrasound in the pre-operative assessment of breast cancer patients? European Radiology. 2015; 25:2682-2687.
18. Marinovich ML, Houssami N, Macaskill P, von Minckwitz G, Blohmer JU and Irwig L. Accuracy of ultrasound for predicting pathologic response during neoadjuvant therapy for breast cancer. International journal of cancer. 2015; 136:2730-2737.
19. Boughey JC, Ballman KV, Hunt KK, McCall LM, Mittendorf EA, Ahrendt GM, Wilke LG and Le-Petross HT. Axillary Ultrasound After Neoadjuvant Chemotherapy and Its Impact on Sentinel Lymph Node Surgery: Results From the American College of Surgeons Oncology Group Z1071 Trial (Alliance). Journal of Clinical Oncology. 2015; 33:3386-3393.
20. Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, Blumencranz PW, Leitch AM, Saha S, McCall LM and Morrow M. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. Jama. 2011; 305:569-575.
21. Kuijs VJ, Moossdorff M, Schipper RJ, Beets-Tan RG, Heuts EM, Keymeulen KB, Smidt ML and Lobbes MB. The role of MRI in axillary lymph node imaging in breast cancer patients: a systematic review. Insights into imaging. 2015; 6:203-215.
22. Gentilini O and Veronesi U. Abandoning sentinel lymph node biopsy in early breast cancer? A new trial in progress at the European Institute of Oncology of Milan (SOUND: Sentinel node vs Observation after axillary UltraSouND). Breast. 2012; 21:678-681.
23. Alvarado R, Yi M, Le-Petross H, Gilcrease M, Mittendorf EA, Bedrosian I, Hwang RF, Caudle AS, Babiera GV, Akins JS, Kuerer HM and Hunt KK. The role for sentinel lymph node dissection after neoadjuvant chemotherapy in patients who present with node-positive breast cancer. Ann Surg Oncol. 2012; 19:3177-3184.
24. Lee MC, Gonzalez SJ, Lin H, Zhao X, Kiluk JV, Laronga C and Mooney B. Prospective Trial of Breast MRI Versus 2D and 3D Ultrasound for Evaluation of Response to Neoadjuvant Chemotherapy. Annals of Surgical Oncology. 2015; 22:2888-2894.
25. Dialani V, Chadashvili T and Slanetz PJ. Role of Imaging in Neoadjuvant Therapy for Breast Cancer. Annals of Surgical Oncology. 2015; 22:1416-1424.
26. Koolen BB, Valdés Olmos RA, Wesseling J, Vogel WV, Vincent AD, Gilhuijs KGA, Rodenhuis S, Rutgers EJT and Vrancken Peeters MJ. Early Assessment of Axillary Response with 18F-FDG PET/CT during Neoadjuvant Chemotherapy in Stage II–III Breast Cancer: Implications for Surgical Management of the Axilla. Annals of Surgical Oncology. 2013; 20:2227-2235.
27. Marinovich ML, Sardanelli F, Ciatto S, Mamounas E, Brennan M, Macaskill P, Irwig L, von Minckwitz G and Houssami N. Early prediction of pathologic response to neoadjuvant therapy in breast cancer: Systematic review of the accuracy of MRI. The Breast. 2012; 21:669-677.
28. Moorman AM, Bourez RLJH, de Leeuw DM and Kouwenhoven EA. Pre-operative Ultrasonographic Evaluation of Axillary Lymph Nodes in Breast Cancer Patients: For Which Group Still of Additional Value and in Which Group Cause for Special Attention? Ultrasound in Medicine & Biology. 2015; 41:2842-2848.
29. Straver ME, Rutgers EJT, Russell NS, Oldenburg HSA, Rodenhuis S, Wesseling J, Vincent A and Peeters MTFDV. Towards rational axillary treatment in relation to neoadjuvant therapy in breast cancer. European Journal of Cancer. 2009; 45:2284-2292.
30. Johnson S, Brown S, Porter G, Steel J, Paisley K, Watkins R and Holgate C. Staging primary breast cancer. Are there tumour pathological features that correlate with a false-negative axillary ultrasound? Clinical radiology. 2011; 66:497-499.
31. Hennessy BT. Outcome After Pathologic Complete Eradication of Cytologically Proven Breast Cancer Axillary Node Metastases Following Primary Chemotherapy. Journal of Clinical Oncology. 2005; 23:9304-9311.
32. Mamounas EP, Anderson SJ, Dignam JJ, Bear HD, Julian TB, Geyer CE Jr, Taghian A, Wickerham DL and Wolmark N. Predictors of locoregional recurrence after neoadjuvant chemotherapy: results from combined analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. Journal of clinical oncology. 2012; 30:3960-3966.
33. Ko ES, Han H, Han BK, Kim SM, Kim RB, Lee GW, Park YH and Nam SJ. Prognostic Significance of a Complete Response on Breast MRI in Patients Who Received Neoadjuvant Chemotherapy According to the Molecular Subtype. Korean journal of radiology. 2015; 16:986-995.
34. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). European Journal of Cancer. 2009; 45:228-247.
35. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, Fitzgibbons PL, Francis G, Goldstein NS, Hayes M, Hicks DG, Lester S, Love R, et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. Journal of clinical oncology. 2010; 28:2784-2795.