
Introduction
Biliary tract cancer (BTC) consists of intrahepatic cholangiocarcinoma (IHCC), extrahepatic cholangiocarcinoma (EHCC), gallbladder cancer (GB ca) and ampulla of vater cancer (AoV ca), and it has a poor prognosis. [1]
Gallstones, chronic hepatitis B or C, inflammatory disease of bile duct such as primary sclerosing cholangitis and certain liver parasites are well known risk factors of BTC, which might make the chronic inflammation state. [2-4]
The human immune system could recognize cancer cells and suppress cancer progression or metastasis. However, cancer cells have innate or acquired immune evasion mechanisms, which result in disease progression. [5, 6] Immune-related cells including neutrophils, lymphocytes and platelets could suppress the circulating tumor cells. [7, 8] Recently, immuno-oncology has become a promising approach in the field of new anti-cancer drug development, especially with the success of immune checkpoint inhibitors in melanoma, non-small cell lung cancer and renal cell carcinoma. [9-12]
In BTC, there is also a strong potential to use immune modulation strategy to fight against cancer. [13-15] In the genomic spectra of BTC, unsupervised clustering of global gene expression levels determined by transcriptome sequencing revealed 4 molecular subgroups. [13] Among these, the worst prognostic group was enriched with genes involved in the immune system and cytokine activity. Hypermutated cases were significantly enriched in this subgroup, and the expression of immunosuppressive immune checkpoint molecules including programmed death-ligand 1 (PD-L1) (CD274) was significantly higher in this worst prognosis subgroup. In total, 45.2% of cases showed an increase in the expression of immune checkpoint molecules. This subgroup may be a good target population for immunotherapy.
For these immunotherapies, many candidate biomarkers such as Wnt inhibitor Dickkopf-1, IFN-γ and TGF-β are under investigation. [14, 15] PD-L1 expression in cancer cells or tumor microenvironment is a candidate biomarker for immune checkpoint inhibitors. [16-19] PD-L1 is expressed in macrophages and dendritic cells and can bind to programmed death-l (PD1) in activated T and B lymphocytes and NK cells. [20] When PD-L1 binds to PD1, inhibitory signals are activated, which in turn act as a negative regulator of T cell activity in tissue. [21, 22] Tumor cells also express PD-L1 to activate inhibitory signals as a mechanism of overcoming host immune response, so-called immune checkpoints. [23, 24]
For assessment of PD-L1 expression on tumor cells or immune cells, acquisition of tumor tissue in invasive measure is needed, which is always a challenging issue, especially in BTC. The soluble form of PD-L1 (sPDL1) in peripheral blood is believed to impair host immunity and cause poor clinical outcomes in renal cell carcinoma, diffuse large B cell lymphoma and multiple myeloma. [25-27]
The purpose of this study was to measure sPDL1 in the serum of BTC patients and to evaluate its clinical implication in advanced BTC patients receiving palliative chemotherapy.
Results
Patient characteristics
In the entire cohort (N = 158), median age was 59.6 years old (range, 31.3- 76.2) and primary sites of tumor were: IHCC 43.0%, GB ca 35.4%, EHCC 13.9% and AoV ca 7.6% (Table 1).
Median follow-up duration was 95.3 months, and median OS was 9.07 months (95% CI: 8.20- 11.33) (Supplementary Figure 1).
A total of 143 patients received 5-FU based chemotherapy. Among them, 140 patients received combined chemotherapy with 5-FU and platinum. Three patients were treated with 5-FU+doxorubicin+ mitomycin C. Fifteen patients received gemcitabine with platinum combination chemotherapy.
Using a simple random sampling method, 79 patients were randomly assigned to the training cohort and the other 79 patients to validation cohort to validate biomarkers. Median OS was 8.23 months (95% CI: 6.80-11.30) and 10.13 months (95% CI: 8.53-13.60) in the training cohort and validation cohort, respectively (Supplementary Figure 1). The clinical characteristics such as age, sex, primary origin, albumin, CEA, CA19-9, etc. did not show significant differences between cohorts.
Table 1: Patient characteristics
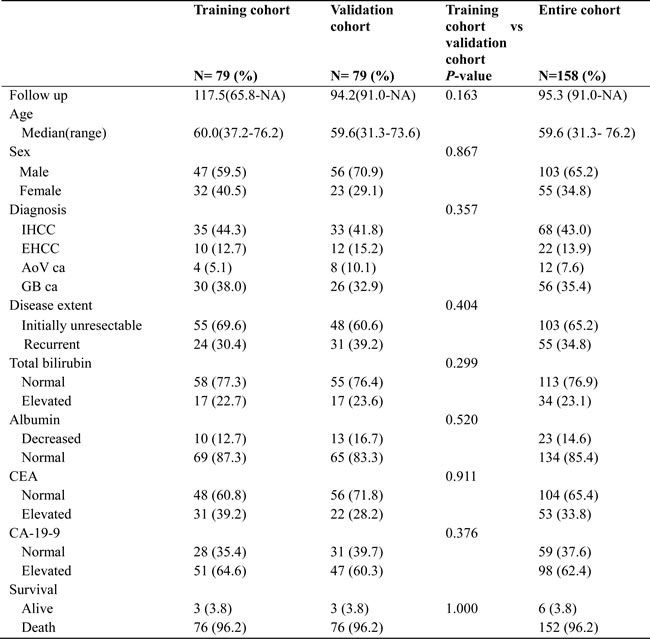
IHCC, intrahepatic cholangiocarcinoma; EHCC, extrahepatic cholangiocarcinoma; AoV ca, ampulla of vater cancer; GB ca, gallbladder cancer; CEA, carcinoembryonic antigen; CA-19-9, carbohydrate antigen 19-9.
Normal value; total bilirubin, 0.2- 1.2 mg/dL; albumin, 3.3-5.2 g/dL; CEA 0-5 ng/dL; CA-19-9, 0-37 U/mL
Biomarkers for host immunity
Median sPDL1 of enrolled patients was 1.20 ng/mL (range, 0.5-2.1) (Table 2). Median sPDL1 of normal healthy populations was 1.20 ng/mL (range, 0.5- 1.9) which was similar to BTC patients’ serum level (Supplementary Figure 2). There are no significant difference of sPDL1 according to age and gender between healthy population and BTC cancer patients (Supplementary Table 1A and 1B).
Median sPDL1 according to disease extent differed in patients: 1.44 ng/mL (range, 0.03-7.28) in initially unresectable cases and 0.94 ng/mL (range, 0.06-4.39) in recurrent cases (p = 0.005). According to primary origin, level of sPDL1 was highest in IHCC and lowest in EHCC. The patients with lower sPDL1 showed more prolonged OS (Figure 1A). Analysis of cubic splines between hazard ratio and sPDL1 showed an increased risk of death with increasing level of sPDL1 (Figure 1B).
Table 2: Biomarkers for host immunity
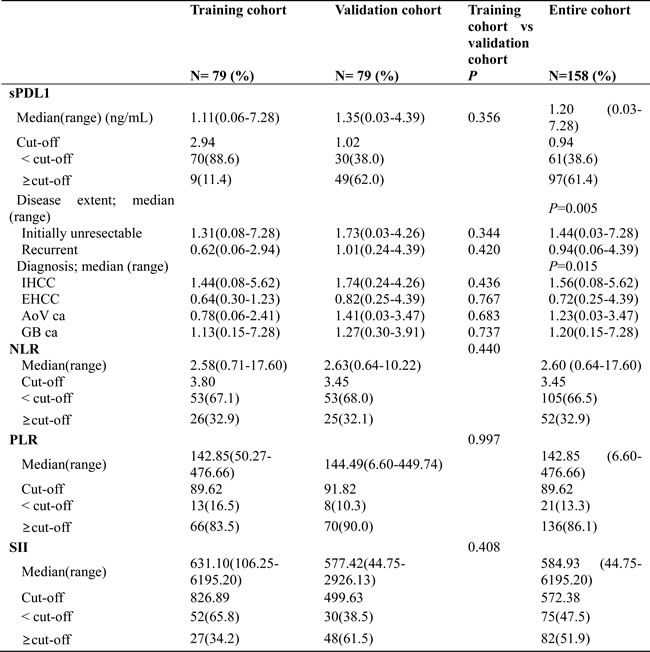
NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic immune-inflammation index; sPDL1, soluble form PD-L1.
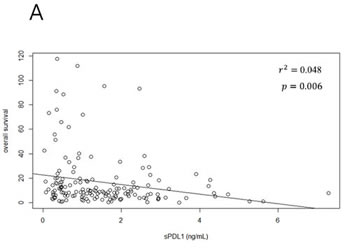
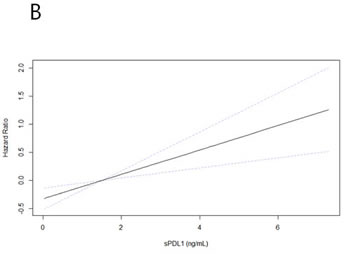
Figure 1: sPDL1 and overall survival. A. Correlation between sPDL1 and overall survival: Each dot represents a patient. Patients with high levels of sPDL1 were distributed in the shorter overall survival group. B. Cubic splines model between sPDL1 and overall survival: sPDL1 shows an increased hazard ration with increasing level. Hazard ratio is represented by a solid line and 95% confidential interval is a dotted line.
The cut-off value of sPDL1 in entire cohort to separate different prognosis groups, calculated by the minimum P value approach, was 0.94 ng/mL. The sPDL1 cut-off value in training and validation cohorts was 2.94 and 1.02 ng/mL, respectively, and it was analyzed for validation of sPDL cut-off in entire cohort. The p value of sPDL1 cross-validation was 0.024, meaning that the patients with sPDL1 ≥0.94 ng/mL had worse OS than sPDL1 <0.94 ng/mL (Table 3, Figure 2A).
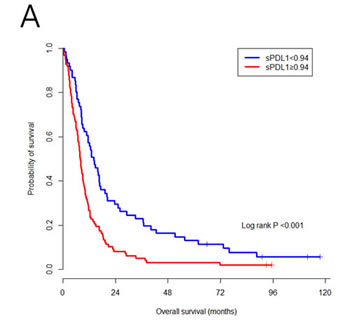
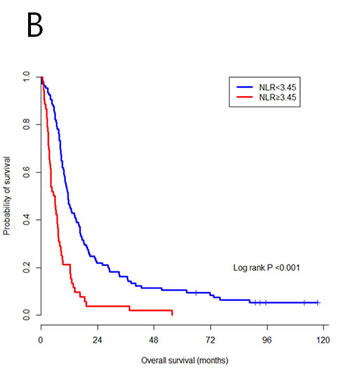
Figure 2: Survival outcomes according to sPDL1 A. and NLR B. The patients with a high level of sPDL1 or NLR had worse overall survival.
Median NLR was 2.60 (range, 0.64-17.60), PLR was 142.85 (range, 6.60-17.60) and SII was 584.93 (44.75-6195.20). Cut-off values of NLR, PLR and SII to separate OS were 3.45, 89.62 and 572.38, respectively (Table 2), and NLR was the only biomarker with significant p value in cross-validation, as shown in Table 3. The patients with lower NLR than the cut-off showed longer OS (p < 0.001) (Figure 2B). Cubic splines model between hazard ratio and each marker of NLR, PLR and SII also showed a positive relation (Supplementary Figure 3A-3C).
Table 3: Validation of cut-off value

sPDL, soluble form of PD-L1; OS, overall survival; HR, hazard ratio; CI, confidence interval.
Prognostic factors for OS
In univariate analysis, performance status, diagnosis, disease extent (initially unresectable vs. recurrent), number of metastasized organs, low albumin and high CEA/CA-19-9 were significant prognostic factors (Table 4). Among immune-related biomarkers, sPDL1, NLR and SII were significant for OS (HR (95% CI): sPDL1, 1.891 (1.35-2.65), p < 0.001; NLR, 2.604 (1.84-3.69), p < 0.001; and SII, 1.917 (1.38-2.66), p < 0.001). sPDL1 and NLR were also significant independent prognostic factors in multivariate analysis along with disease extent, albumin and CEA.
Table 4: Prognostic factors for OS
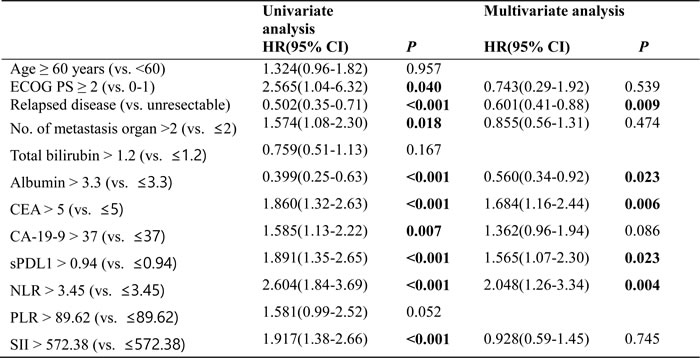
ECOG PS, Estern Cooperative Oncology Group Performance Status; UNL, upper normal limit; LNL, lower normal limit; CEA, carcinoembryonic antigen; CA-19-9, carbohydrate antigen 19-9; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic immune-inflammation index; sPDL1, soluble form of PD-L1; OS, overall survival; HR, hazard ratio; CI, confidence interval.
Normal value; total bilirubin, 0.2- 1.2 mg/dL; albumin, 3.3-5.2 g/dL; CEA 0-5 ng/dL; CA-19-9, 0-37 U/mL
Discussion
This study demonstrated that sPDL1 could be measured by ELISA in the serum of BTC patients and that high level of sPDL1 was a negative prognostic factor in BTC patients who received palliative chemotherapy. NLR and SII which represent a host immune-inflammation state were also significant prognostic factors for survival in univariate analysis, and only NLR was significant in multivariate analysis.
PD1/PD-L1 is associated with an inflammatory tumor microenvironment as a regulator of inhibitory signals, and its expression could be a candidate biomarker for patient selection for anti-PD1/PD-L1 monoclonal antibodies. [28, 29] To evaluate PD1/PD-L1 in tumor cells and tumor microenvironment, the acquisition of adequate tissue is obligatory. Tumor biopsy is a challenge in the management of cancer patients. Especially in BTC, some types of tumor spread only along the bile duct, which make it difficult to get adequate tumor tissue. To overcome such issue, the liquid biopsy or liquid biomarker is an appealing approach to pursue.
PD-L1 is expressed on the surface of activated antigen presenting cells. It is also expressed on the membrane of human tumor cells, which is one of the mechanisms of escaping the host immune system. sPDL1 is thought to be a circulating biologically active protein which is released from PD-L1-positive tumor cells or immune cells. It could contribute to systemic immunosuppression. [25, 26]
However, the exact function and role of sPDL1 is mainly unresolved so far. In the current study, we measured sPDL1 by ELISA in the serum of BTC patients, which was collected before initiation of palliative chemotherapy. Importantly, sPDL1 could be measured in all patients, whose range was 0.03-7.28 ng/mL. The recurrent cases, which are believed to have low tumor burden, showed a lower level of sPDL1 than initially unresectable cases. In parallel with this sPDL1 level, OS was longer in recurrent cases than initially unresectable cases (14.20 month vs 7.93 months). Among the 4 origins of BTC, IHCC showed the highest level of sPDL1 and worst OS (8.32 months).
The level of sPDL1 is an independent poor prognostic factor for OS in univariate and multivariate analysis. The patients with sPDL1 <0.94 ng/mL had significantly prolonged OS which was validated by the twofold cross-validation method in training and validation cohorts. The level of sPDL1 before chemotherapy could be a useful biomarker to predict prognosis of BTC patients.
Recently, several studies on the antitumor action of the host immune have shown that NLR, PLR and SII have prognostic value in solid tumors including BTC. [30-32] We also analyzed the association between OS and immune biomarkers such as NLR, PLR and SII. According to the cut-off in each cohort, patients with a high level of NLR, PLR and SII had worse OS. When we validated the cut-off value of these immune markers, NLR was the only validated one with adverse prognostic value. On multivariate analysis, a high level of NLR implied prognostic impact on OS.
Our study had limitations. It was a retrospective, single center study. The patients’ serum collected for biomedical research before initiation of palliative chemotherapy was retrospectively analyzed. Even though we tried to validate the cut-off value of biomarkers, these findings should be further validated in a different independent patient cohort with prospective design. Furthermore, studies on the function of sPDL1 and its mechanism of action are needed. In parallel, as a prognostic factor, the more strength of sPDL1 compared with NLR, which is a very pragmatic, easily applicable clinical factor for the practice on advanced biliary tract cancer patients, should be studied. Besides the study on prognostic role of sPDL1, the study on the predictive role of sPDL1 to the chemotherapy efficacy is also interesting topic and needed to reveal the biology of sPDL1.
Despite the limitations, a prognostic impact of the host immune-inflammation system in BTC patients was uncovered in our study. To the best of our knowledge, this is the first study on the role of sPDL1 in BTC patients. In addition, analysis was performed in a relatively large cohort and by dividing the respective cohort for more exact validation.
In conclusion, sPDL1 can be measured in the serum of BTC patients, and a high level of sPDL is an independent prognostic factor in advanced BTC patients treated with palliative chemotherapy. This study suggests the possible role of sPDL1 as a liquid biomarker for immuno-oncology drug development.
Patients and Methods
Patients and data collection
In a patient cohort with pathologically diagnosed, unresectable or recurrent BTC, patients whose blood samples were collected before initiation of palliative first-line chemotherapy were considered for this study. Between 2004 and 2009, patients who provided informed consent for the biomarker analysis study in Seoul National University Hospital were finally recruited for this study (N = 158).
Data of baseline demographics were collected from medical charts. Laboratory data including total bilirubin, albumin, CEA, CA-19-9 and blood cell count with neutrophils, platelets and lymphocytes were also collected. Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were calculated by dividing the neutrophil or platelet count by the lymphocyte count obtained before initiation of first-line palliative chemotherapy. Systemic immune-inflammation index (SII) was defined as neutrophil x platelet/lymphocyte count. [31]
For evaluating the sPDL1 levels in normal healthy population, we did the age-, and sex-matched selection of normal control to the biliary tract cancer patients in a ratio of 3:1. We used the serum samples obtained from healthy population, which had been collected under IRB-approved studies (IRB number: 1103-150-357).
sPDL1 was measured using an enzyme-linked immunosorbent assay (PDCD1LG1 ELISA kit, USCN Life Science) in patient and normal healthy person’s serum according to the manufacturer’s instructions. Each sample was analyzed in duplicate. [25]
Statistical analysis
Pearson’s chi-square test or Fisher’s exact test was used for categorical variables, as appropriate. A t-test was used for comparison of means. Overall survival (OS) was defined as the time from day 1 of chemotherapy to date of death or last follow-up. Median OS was calculated using the Kaplan-Meier method and comparisons of difference between groups was assessed using log-rank tests. We defined patients’ current status on death or alive using National Mortality Tracking System at the data cut-off timing. There was no one censored case for overall survival.
Univariate and multivariate analysis for OS was performed using Cox regression models. Factors with p < 0.05 in univariate analysis were collected and analyzed in multivariate regression models. All statistical tests were two-sided, with significance defined as p < 0.05.
We randomly divided enrolled patients into two cohorts (training and validation cohort) using a simple random sampling method. [33] Cut-off values of each variable (sPDL1, NLR, PLR and SII) for OS prediction were determined by using the minimum p value approach in each group. [34] To validate the cut-off value of each biomarker, a twofold cross-validation method was used. [35] The training and validation cohort were divided into a higher and lower group according to cut-off value. If there were significant differences on survival analysis between the high and lower group, the cut-off value of the entire cohort was defined significant prognostic value.
We performed this analysis using SAS 9.2 (by SAS Institute Inc., Cary, NC, USA)
Ethics
The study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Hospital (H-1408-039-600). All studies were conducted according to guidelines for biomedical research (Declaration of Helsinki).
Acknowledgments
We thank the patients included in the current study. We thank Dr. Eun-Young Lee for providing normal healthy population serum samples.
Conflicts of Interest
The authors declare no conflicts of interest.
Grant Support
This research was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (Grant No. 1320090) and a grant from Seoul National University College of Medicine (800-20150040)
References
1. Kohler BA, Sherman RL, Howlader N, Jemal A, Ryerson AB, Henry KA, Boscoe FP, Cronin KA, Lake A and Noone A-M. Annual Report to the Nation on the Status of Cancer, 1975-2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State. Journal of the National Cancer Institute. 2015; 107(6):djv048.
2. Lee C, Chang C, Lin Y, Yeh C, Chen M and Hsieh S. Viral hepatitis-associated intrahepatic cholangiocarcinoma shares common disease processes with hepatocellular carcinoma. British journal of cancer. 2009; 100(11):1765-1770.
3. El-Serag HB, Engels EA, Landgren O, Chiao E, Henderson L, Amaratunge HC and Giordano TP. Risk of hepatobiliary and pancreatic cancers after hepatitis C virus infection: A population-based study of US veterans. Hepatology. 2009; 49(1):116-123.
4. Chapman R. Risk factors for biliary tract carcinogenesis. Annals of oncology. 1999; 10(suppl 4):S308-S311.
5. Hanahan D and Weinberg RA. Hallmarks of cancer: the next generation. cell. 2011; 144(5):646-674.
6. Miska J, Bas E, Devarajan P and Chen Z. Autoimmunity-mediated antitumor immunity: Tumor as an immunoprivileged self. European journal of immunology. 2012; 42(10):2584-2596.
7. Lucci A, Hall CS, Lodhi AK, Bhattacharyya A, Anderson AE, Xiao L, Bedrosian I, Kuerer HM and Krishnamurthy S. Circulating tumour cells in non-metastatic breast cancer: a prospective study. The lancet oncology. 2012; 13(7):688-695.
8. Fan Z-C, Yan J, Liu G-D, Tan X-Y, Weng X-F, Wu W-Z, Zhou J and Wei X-B. Real-time monitoring of rare circulating hepatocellular carcinoma cells in an orthotopic model by in vivo flow cytometry assesses resection on metastasis. Cancer research. 2012; 72(10):2683-2691.
9. Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C and Lotem M. Pembrolizumab versus ipilimumab in advanced melanoma. New England Journal of Medicine. 2015; 372(26):2521-2532.
10. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M and Horn L. Pembrolizumab for the treatment of non-small-cell lung cancer. New England Journal of Medicine. 2015; 372(21):2018-2028.
11. Yang JC, Hughes M, Kammula U, Royal R, Sherry RM, Topalian SL, Suri KB, Levy C, Allen T and Mavroukakis S. Ipilimumab (anti-CTLA4 antibody) causes regression of metastatic renal cell cancer associated with enteritis and hypophysitis. Journal of immunotherapy (Hagerstown, Md: 1997). 2007; 30(8):825.
12. Ott PA, Hodi FS and Robert C. CTLA-4 and PD-1/PD-L1 blockade: new immunotherapeutic modalities with durable clinical benefit in melanoma patients. Clinical Cancer Research. 2013; 19(19):5300-5309.
13. Nakamura H, Arai Y, Totoki Y, Shirota T, Elzawahry A, Kato M, Hama N, Hosoda F, Urushidate T and Ohashi S. Genomic spectra of biliary tract cancer. Nature genetics. 2015.
14. Disis ML. Immunologic biomarkers as correlates of clinical response to cancer immunotherapy. Cancer immunology, immunotherapy. 2011; 60(3):433-442.
15. Sato N, Yamabuki T, Takano A, Koinuma J, Aragaki M, Masuda K, Ishikawa N, Kohno N, Ito H and Miyamoto M. Wnt inhibitor Dickkopf-1 as a target for passive cancer immunotherapy. Cancer research. 2010; 70(13):5326-5336.
16. Taube JM, Klein A, Brahmer JR, Xu H, Pan X, Kim JH, Chen L, Pardoll DM, Topalian SL and Anders RA. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clinical Cancer Research. 2014; 20(19):5064-5074.
17. Gao Q, Wang X-Y, Qiu S-J, Yamato I, Sho M, Nakajima Y, Zhou J, Li B-Z, Shi Y-H and Xiao Y-S. Overexpression of PD-L1 significantly associates with tumor aggressiveness and postoperative recurrence in human hepatocellular carcinoma. Clinical Cancer Research. 2009; 15(3):971-979.
18. Hino R, Kabashima K, Kato Y, Yagi H, Nakamura M, Honjo T, Okazaki T and Tokura Y. Tumor cell expression of programmed cell death-1 ligand 1 is a prognostic factor for malignant melanoma. Cancer. 2010; 116(7):1757-1766.
19. Sabatier R, Finetti P, Mamessier E, Adelaide J, Chaffanet M, Ali HR, Viens P, Caldas C, Birnbaum D and Bertucci F. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget. 2015; 6(7):5449-5464. doi: 10.18632/oncotarget.3216.
20. Agata Y, Kawasaki A, Nishimura H, Ishida Y, Tsubat T, Yagita H and Honjo T. Expression of the PD-1 antigen on the surface of stimulated mouse T and B lymphocytes. International immunology. 1996; 8(5):765-772.
21. Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB, Roche PC, Lu J, Zhu G and Tamada K. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nature medicine. 2002; 8(8):793-800.
22. Postow MA, Callahan MK and Wolchok JD. Immune checkpoint blockade in cancer therapy. Journal of Clinical Oncology. 2015:JCO. 2014.2059. 4358.
23. Zou W and Chen L. Inhibitory B7-family molecules in the tumour microenvironment. Nature Reviews Immunology. 2008; 8(6):467-477.
24. Lipson EJ, Vincent JG, Loyo M, Kagohara LT, Luber BS, Wang H, Xu H, Nayar SK, Wang TS and Sidransky D. PD-L1 expression in the merkel cell carcinoma microenvironment: association with inflammation, merkel cell polyomavirus, and overall survival. Cancer immunology research. 2013; 1(1):54-63.
25. Frigola X, Inman BA, Lohse CM, Krco CJ, Cheville JC, Thompson RH, Leibovich B, Blute ML, Dong H and Kwon ED. Identification of a soluble form of B7-H1 that retains immunosuppressive activity and is associated with aggressive renal cell carcinoma. Clinical Cancer Research. 2011; 17(7):1915-1923.
26. Rossille D, Gressier M, Damotte D, Maucort-Boulch D, Pangault C, Semana G, Le Gouill S, Haioun C, Tarte K and Lamy T. High level of soluble programmed cell death ligand 1 in blood impacts overall survival in aggressive diffuse large B-Cell lymphoma: results from a French multicenter clinical trial. Leukemia. 2014; 28(12):2367-2375.
27. Wang L, Wang H, Chen H, Wang W, Chen X, Geng Q, Xia Z and Lu Y. Serum levels of soluble programmed death ligand 1 predict treatment response and progression free survival in multiple myeloma. Oncotarget. 2015; 6(38):41228-41236. doi: 10.18632/oncotarget.5682.
28. Gajewski TF, Fuertes M, Spaapen R, Zheng Y and Kline J. Molecular profiling to identify relevant immune resistance mechanisms in the tumor microenvironment. Current opinion in immunology. 2011; 23(2):286-292.
29. Ji R-R, Chasalow SD, Wang L, Hamid O, Schmidt H, Cogswell J, Alaparthy S, Berman D, Jure-Kunkel M and Siemers NO. An immune-active tumor microenvironment favors clinical response to ipilimumab. Cancer Immunology, Immunotherapy. 2012; 61(7):1019-1031.
30. McNamara M, Templeton A, Maganti M, Walter T, Horgan A, McKeever L, Min T, Amir E and Knox J. Neutrophil/lymphocyte ratio as a prognostic factor in biliary tract cancer. European Journal of Cancer. 2014; 50(9):1581-1589.
31. Hu B, Yang X-R, Xu Y, Sun Y-F, Sun C, Guo W, Zhang X, Wang W-M, Qiu S-J and Zhou J. Systemic Immune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clinical Cancer Research. 2014; 20(23):6212-6222.
32. Qi Q, Geng Y, Sun M, Wang P and Chen Z. Clinical implications of systemic inflammatory response markers as independent prognostic factors for advanced pancreatic cancer. Pancreatology. 2015; 15(2):145-150.
33. Hansen MH, Hurwitz WN and Madow WG. Sample Survey Methods and Theor. 1953.
34. Williams BA. Finding optimal cutpoints for continuous covariates with binary and time-to-event outcomes. 2006.
35. Faraggi D and Simon R. A simulation study of cross-validation for selecting an optimal cutpoint in univariate survival analysis. Statistics in medicine. Statistics in medicine. 1996; 15(20):2203-2213.