
INTRODUCTION
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death among females worldwide, with an estimated 1.7 million incidence and 521,900 mortalities in 2012 [1]. Importantly, Breast cancer alone accounts for 25% of all cancers and 15% of all cancer-related deaths among females [1]. Lack of effective adjuvant therapies may be an important reason for its recurrence and metastasis, which would even result in the death of the patients. Postmastectomy radiation therapy (PMRT), a commonly used practice, can prevent locoregional recurrence and increase survival in breast cancer patients after definite surgery [2–4]. Previous studies have shown that PMRT therapy yielded both a substantial reduction in locoregional failure from 32% to 9% and a significant improvement in 10-year overall survival from 45% to 54% [5]. At present, National Comprehensive Cancer Network (NCCN) guidelines have intended to list PMRT as a recommended therapy for breast cancer patients with four or more positive lymph nodes. Interestingly, personalized therapy has been favored by oncologists to treat different breast cancer patients. A recent research have shown that PMRT did not have any effect on survival of these patients with four or more positive lymph nodes in a defined subgroup [6]. Therefore, whether all breast cancer patients with four or more positive lymph nodes who underwent modified radical mastectomy should be treated with PMRT needs to be tested and validated.
In the present study, using the Surveillance, Epidemiology, and End Results (SEER)-registered database, we analyzed the prognostic factors of breast cancer patients with four or more positive lymph nodes after PMRT, and answered this interesting clinical question.
RESULTS
Characteristics of the patients who underwent PMRT between 1998 and 2001
A total of 3972 female breast cancer patients with four or more positive lymph nodes who underwent PMRT were reported in the SEER database from 1998 to 2001. The clinical characteristics and pathological features of all the patients were summarized in Table 1. Most of the patients were diagnosed at the age of more than 40-year-old (87.9%). 51.9% of the patients were in stage IIIA according to AJCC stage, and 44.6% of the patients were in AJCC T2 stage (tumor size) and 60.6% of the patients were in N2 (lymph node stage). Almost all the patients were diagnosed in grade II and III (87.3%). In addition, 64.4%of patients were ER positive and 54.4% of patients were PR positive. The detailed statistical results were showed in Table 1.
Table 1: Characteristics of breast cancer patients with four or more positive lymph nodes after PMRT from SEER Database from 1998-2001
Characteristic |
Number |
% |
|---|---|---|
Age |
|
|
< 40 |
482 |
12.1 |
≥ 40 |
3490 |
87.9 |
Laterality |
|
|
Right |
2029 |
51.0 |
Left |
1942 |
48.9 |
AJCC Stage |
|
|
II |
71 |
1.8 |
IIIA |
2063 |
51.9 |
IIIB |
371 |
9.3 |
IIIC |
1463 |
36.8 |
AJCC T |
|
|
T1 |
675 |
17.0 |
T2 |
1773 |
44.6 |
T3 |
771 |
19.4 |
T4 |
644 |
16.2 |
AJCC N |
|
|
N2 |
2408 |
60.6 |
N3 |
1560 |
39.3 |
Grade |
|
|
I |
196 |
4.9 |
II |
1305 |
32.9 |
III |
2159 |
54.4 |
ER status |
|
|
Positive |
2557 |
64.4 |
Negative |
1022 |
25.7 |
PR status |
|
|
Positive |
2159 |
54.4 |
Negative |
1361 |
34.3 |
Survival outcomes of patients between 1998 and 2001
As universally acknowledged, PMRT has been a standard adjuvant postoperative therapy for patients with four or more positive lymph nodes. In our study, we identified breast cancer patients without PMRT after modified radical mastectomy to compare prognosis with those who underwent PMRT from 1998 to 2001. The clinical characteristics and pathological features of all the patients with non-PMRT were summarized in supply Table 1. As expected, the results showed that PMRT patients had better outcomes with significantly improved overall survival rate (OS) (χ2=186.4, P < 0.001) and cancer specific survival rate (CSS) (χ2=74.8, P < 0.001) compared to the non-PMRT patients (Figure 1A and 1B).
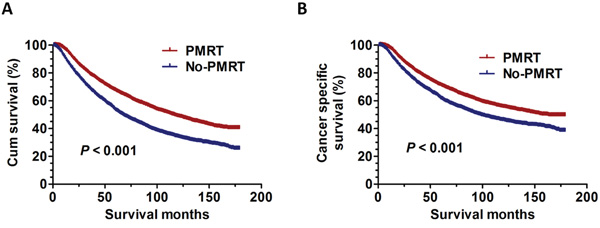
Figure 1: The survival curves in breast cancer patients with PMRT and No-PMRT between 1998 and 2001. A. The OS curves: (χ2=186.4, P < 0.001). B. The CSS curves (χ2=74.8, P < 0.001).
Determination of the risk factors of patients who underwent PMRT from 1998 to 2001
The prognoses of all the patients who underwent PMRT were further analyzed using univariate and multivariate Cox proportional hazards regression analysis. The correlation between OS and various variables are summarized in Table 2. The clinicopathological features, including AJCC stage (χ2=213.6, P < 0.001), AJCC T (χ2=132.2, P < 0.001), AJCC N (χ2=107.3, P < 0.001), Grade (χ2=84.6, P < 0.001), ER status (χ2=153.9, P < 0.001), PR status (χ2=129.5, P < 0.001), were significant risk factors for OS using univariate analysis. Multivariate analysis with Cox regression was further performed and found that AJCC stage (hazard ratio [HR] 1.505; 95% confidence interval [CI] 1.308-1.732; P < 0.001), AJCC T (HR 1.369; 95% CI 1.245-1.505; P < 0.001), Grade (HR 1.226; 95% CI 1.115-1.350; P < 0.001), ER status (HR 1.424; 95% CI 1.258-1.613; P < 0.001), PR status (HR 1.213; 95% CI 1.078-1.364; P = 0.001) were independent prognostic factors for OS.
Table 2: Univariate analysis and multivariate survival analyses to evaluate the prognostic factors according to various clinicopathological variables from SEER Database from 1998-2001
Variable |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
Log rank χ2 test |
P |
HR (95%CI) |
P |
|
Age |
0.067 |
0.796 |
|
NI |
< 40 |
|
|
|
|
≥ 40 |
|
|
|
|
Laterality |
0.079 |
0.778 |
|
NI |
Left |
|
|
|
|
Right |
|
|
|
|
AJCC Stage |
213.644 |
<0.001 |
|
<0.001 |
II and IIIA |
|
|
reference |
|
IIIB and IIIC |
|
|
1505 (1.308-1.732) |
<0.001 |
AJCC T |
132.227 |
<0.001 |
|
<0.001 |
T1 and T2 |
|
|
reference |
|
T3 and T4 |
|
|
1.369 (1.245-1.505) |
<0.001 |
AJCC N |
107.269 |
<0.001 |
|
0.510 |
N2 |
|
|
reference |
|
N3 |
|
|
1.079 (0.945-1.232) |
0.261 |
Grade |
84.629 |
<0.001 |
|
<0.001 |
I and II |
|
|
reference |
|
III |
|
|
1.226 (1.115-1.350) |
<0.001 |
ER status |
153.872 |
<0.001 |
|
<0.001 |
Positive |
|
|
reference |
|
Negative |
|
|
1.424 (1.258-1.613) |
<0.001 |
PR status |
129.475 |
<0.001 |
|
0.001 |
Positive |
|
|
reference |
|
Negative |
|
|
1.213 (1.078-1.364) |
0.001 |
NI: not included in the multivariate survival analysis.
Establishment of the predictive model for overall survival
Since we have already shown that AJCC stage, AJCC T, Grade, ER status, PR status were independent prognostic factors for OS, we then construct a predictive index for the patients with four or more positive lymph nodes who underwent PMRT based on these confirmed factors. The included factors were the five risk factors, including AJCC stage, AJCC T, Grade, ER status and PR status. The predictive index was defined as the number of the risk factor (NRF). Using the NRF model, we estimated the respective OS and revealed the statistically significant differences in every group (P < 0.001) (Figure 2A). We then divided the patients into good prognosis (NRF 0-1), intermediate prognosis (NRF 2-3), poor prognosis (NRF 4-5) using the predictive index model. The statistically significant differences were also detected in three groups (P < 0.001) (Figure 2B). Besides, we try to ascertain whether the patients undergoing PMRT still have an increased OS and CSS than those without PMRT in the poor prognosis group. Interestingly, the results showed that PMRT can still significantly improve the OS (χ2=15.7, P < 0.001) and CSS (χ2=13.4, P < 0.001) of these breast cancer patients (Figure 2C–2D).
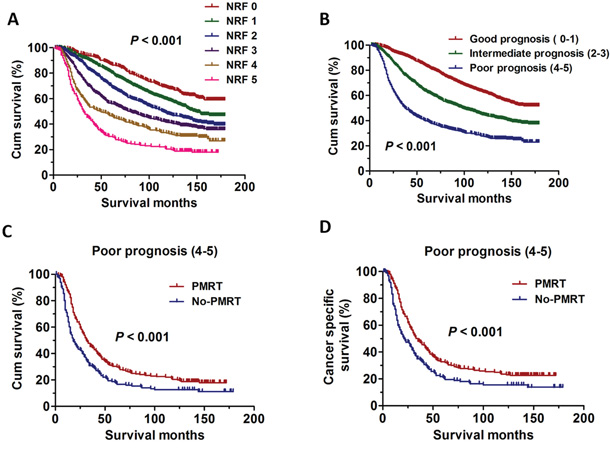
Figure 2: The survival curves in breast cancer patients according to different NRF scoring between 1998 and 2001. A. Kaplan-Meier curves for overall survival rate according to NRF scoring in six groups (P < 0.001). B. Kaplan-Meier curves for overall survival rate according to NRF scoring in three groups (P < 0.001). C. Kaplan-Meier curves for overall survival rate in breast cancer patients with PMRT and No-PMRT in poor prognosis group (χ2=15.7, P < 0.001). D. Kaplan-Meier curves for cancer specific survival rate in breast cancer patients with PMRT and No-PMRT in poor prognosis group (χ2=13.4, P < 0.001).
Subgroup analysis of OS in the predictive model
In the previous prediction model, AJCC Stage IIIB and IIIC, AJCC T3 and T4 were employed as variables to analyze prognosis (Table 2). Next, AJCC Stage IIIB, AJCC Stage IIIC, AJCC T3, AJCC T4 were taken as an independent variable to further analyze prognosis. Univariate and multivariate analyses were used to evaluate the relationships between OS and various variables. The results were summarized in Table 3. The results showed that AJCC T4 (χ2=9.5, P = 0.002) was risk factors for poor OS using univariate analysis. Multivariate analysis with Cox regression was further performed and found that AJCC T (HR 1.340; 95% CI 1.110-1.618; P = 0.002) was independent prognostic factors for OS. Based on these prognostic analyses, we also constructed a predictive index for these patients using the same method. The patients who were in AJCC T3-4 was quantified by the predictive index. Patients being in AJCC T3 get a point of 0 and those in AJCC T4 get a point of 1. Therefore, the NRF 0 stand for those patients with AJCC T3; the NRF 1 stand for those patients with AJCC T4; Then the patients with NRF 0 were categorized into the sub-good prognosis group. The patients with NRF 1 were categorized into the sub-poor prognosis group. The results also showed the statistically significant differences among the two groups (P = 0.002) (Figure 3A). In addition, we also try to ascertain whether patients undergoing PMRT still have an increased OS and CSS than those without PMRT in the sub-poor prognosis group (NRF 1). The Kaplan-Meier analyses were used to generate the survival curves and the Log Rank test was applied to analyze the differences. Interestingly, the results showed that PMRT still have survival benefit on OS (χ2=18.6, P < 0.001) or CSS (χ2=20.0, P < 0.001) for these patients (Figure 3B–3C).
Table 3: Univariate analysis and multivariate survival analyses to evaluate the prognostic factors according to various clinicopathological variables in sub-groups from SEER Database from 1998-2001
Variable |
Univariate analysis |
Multivariate analysis |
||
|---|---|---|---|---|
Log rank χ2 test |
P |
HR (95%CI) |
P |
|
AJCC Stage |
0.981 |
0.322 |
|
NI |
IIIB |
|
|
|
|
IIIC |
|
|
|
|
AJCC T |
9.463 |
0.002 |
|
0.002 |
T3 |
|
|
reference |
|
T4 |
|
|
1.340 (1.110-1.618) |
0.002 |
NI: not included in the multivariate survival analysis.
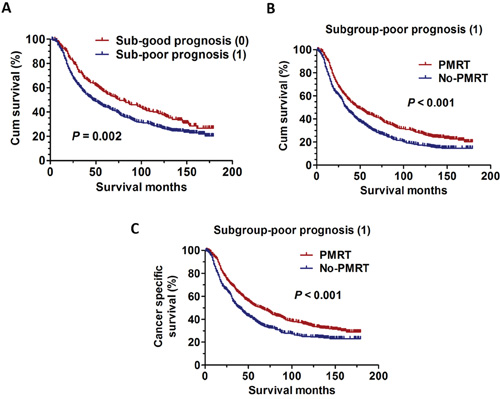
Figure 3: The survival curves in breast cancer patients according to different sub-groups NRF scoring between 1998 and 2001. A. Kaplan-Meier curves for overall survival rate according to sub-groups NRF scoring in two groups (P = 0.002). B. Kaplan-Meier curves for overall survival rate in breast cancer patients with PMRT and No-PMRT in Subgroup-poor prognosis group (χ2=18.6, P < 0.001). C. Kaplan-Meier curves for cancer specific survival rate in breast cancer patients with PMRT and No-PMRT in Subgroup-poor prognosis group (χ2=20.0, P < 0.001).
Validation of the predictive model for overall survival
We have established a predictive index for the patients with four or more positive lymph nodes who underwent PMRT. Next, we identified another group of breast cancer patients with four or more positive lymph nodes who underwent PMRT reported in the SEER database from 2006 to 2009. The clinical characteristics and pathological features of all the patients were summarized in supply Table 2. Consistent with the prediction model, the results also showed the statistically significant differences among the groups using the same predictive index model (P < 0.001) (Figure 4A). In addition, the results also showed that the statistically significant differences were detected in the good prognosis (NRF 0-1), intermediate prognosis (NRF 2-3), poor prognosis (NRF 4-5) group (P < 0.001) (Figure 4B). Then, the subgroup analyses were further performed and the statistically significant differences were also detected in Sub-good prognosis (NRF 0), Sub-intermediate prognosis (NRF 1) (P < 0.001) (Figure 4C).
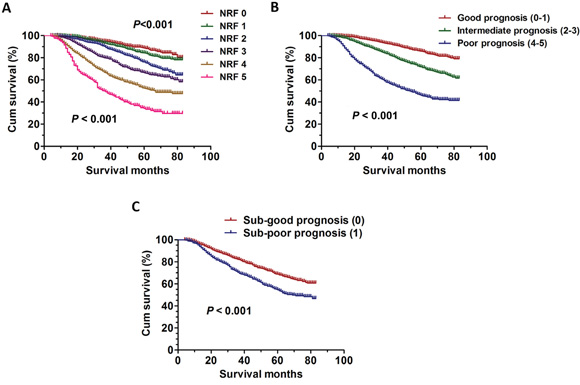
Figure 4: The survival curves in breast cancer patients according to different NRF scoring between 2006 and 2009. A. Kaplan-Meier curves for overall survival rate according to NRF scoring in six groups (P < 0.001). B. Kaplan-Meier curves for overall survival rate according to NRF scoring in three groups (P < 0.001). C. Kaplan-Meier curves for overall survival rate according to NRF scoring in three sub-groups (P < 0.001).
Whether patients in the sub-poor group can benefit from PMRT: the validation
We have shown that the breast cancer patients with four or more positive lymph nodes after modified radical mastectomy can benefit from the PMRT even if the patients were in AJCC T4 (Figure 3B–3C). Next, according to the same standards, we identified the patients with AJCC T4 in the SEER database from 2006 to 2009. The Kaplan-Meier analyses were used to generate the survival curves and the Log Rank test was applied to analyze the differences. As expected, the results also showed PMRT still have some survival benefit on OS (χ2=62.1, P < 0.001) or CSS (χ2=42.5, P < 0.001) for these patients (Figure 5A–5B).
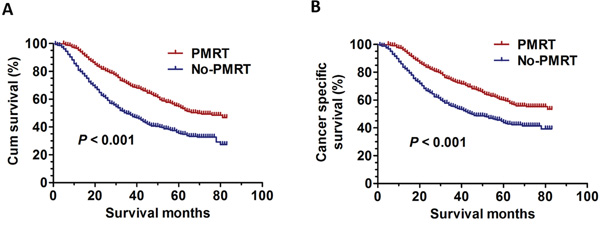
Figure 5: The survival curves in breast cancer patients with PMRT and No-PMRT in Sub-poor prognosis group. A. Kaplan-Meier curves for overall survival rate in breast cancer patients with PMRT and No-PMRT in Sub-poor prognosis group between 2006 and 2009 (χ2=62.1, P < 0.001). B. Kaplan-Meier curves for cancer specific survival rate in breast cancer patients with PMRT and No-PMRT in Sub-poor prognosis group between 2006 and 2009 (χ2=42.5, P < 0.001).
DISCUSSION
In the present study, we concluded that the breast cancer patients with four or more positive lymph nodes aftermodified radical mastectomy can benefit from the PMRT even if the patients were in AJCC T4.
In fact, early randomized trials of breast cancer with PMRT did not prove the improvement in overall survival and just demonstrated that the risk of locoregional recurrence was reduced [8–10]. With the popularity of systemic therapy and the development of radiotherapy, several studies have demonstrated that the patients of breast cancer may benefit from the administration of PMRT. In a Danish trial of premenopausal patients, The frequency of locoregional recurrence alone or with distant metastases was 9% among the women who received radiotherapy plus systemic chemotherapy and 32% among those who received systemic chemotherapy alone; In addition, the probability of survival free of disease and the overall survival after 10 years was 48% and 54% among the women assigned to radiotherapy systemic chemotherapy and 34% and 45% among those treated only with systemic chemotherapy; Importantly, multivariate analysis demonstrated that PMRT significantly improved disease-free survival and overall survival, irrespective of tumor size, the number of positive nodes, or the histopathological grade [5]. In a Danish trial of postmenopausal patients, the rate of locoregional recurrence was 8% in the radiotherapy plus tamoxifen group and 35% in the tamoxifen group; Disease-free survival was 36% in the radiotherapy plus tamoxifen group and 24% in the tamoxifen alone group; Overall survival was also higher in the radiotherapy group (385 vs 434 deaths; survival 45 vs 36% at 10 years) [11]. Importantly, several other studies have also demonstrated PMRT does indeed decrease the mortality and locoregional recurrence [12–14]. The most influential study of these was a meta-analysis conducted by the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). This study included 8500 with mastectomy, axillary clearance, and node-positive disease in trials of radiotherapy, with similar absolute gains from radiotherapy; 5-year local recurrence risks 6% versus 23% (reduction 17%), and 15-year breast cancer mortality risks 54.7% versus 60.1% (reduction 5.4%) [15]. However, some limitation still exist in these trials. For example, the median number of lymph nodes removed was 7 in the Danish 82b and 82c trials. Interestingly, the status and dissection of axillary lymph nodes especially with regard to the number of removed lymph nodes has a critical role in breast cancer patients, and the number of negative lymph nodes can affect the prognosis of breast cancer patients [6, 16–19]. Indeed, the breast cancer patients after mastectomy with 1 to 3 positive lymph nodes who haven’t received PMRT has been demonstrated have lower rates of locoregional recurrence than observed in the Danish and other trials [20–22]. Therefore, at present, consensus guidelines have intended to recommend PMRT for patients who have ≥ 4 involved positive lymph nodes [23–26]. Importantly, the National Comprehensive Cancer Network has recommend that the breast cancer patients with ≥ 4 positive lymph nodes should perform PMRT to the chest wall, supraclavicular, and infraclavicular regions and radiation to the internal mammary region.
Similar to these studies, using the SEER database, we screened the breast cancer patients with four or more positive lymph nodes after PMRT between 1998 and 2001. Our results also showed that PMRT significantly improved patient prognosis on OS and CSS.
At present, individualized treatments are a trend for oncologists to determine different treatment options. Studies have demonstrated that the patients with four or more positive lymph nodes who did not receive PMRT have the local recurrence rate from 11.9 to 59% [27, 28]. That means about 40% of these patients do not benefit from PMRT. Interestingly, a study from China has demonstrated that PMRT did not have any effect on the survival of breast cancer patients with four or more positive lymph nodes if the patients have more than 12 negative lymph nodes [6]. Therefore, it is very important to identify those patients with four or more positive lymph nodes that are not likely to benefit from PMRT. Also, we aim to ascertain whether all breast cancer patients with four or more positive lymph nodes should be treated with PMRT.
Firstly, we screened the breast cancer patients with four or more positive nodes who underwent modified radical mastectomy using the SEER database between 1998 and 2001. Univariate and Multivariate analysis was used and showed that AJCC stage, AJCC T, Grade, ER status, PR status were independent prognostic factors for OS. Then we construct a predictive index for these patients. The predictive index was defined as NRF refer to other study [29]. As expected, the overall survival rate was lower if the patients undergoing PMRT are with the higher NRF score. Interestingly, even if the patient has the highest NRF score, PMRT still improves the survival of patients on OS and CSS. In our study, we took AJCC stage IIIB and IIIC, AJCC T3 and T4as variables respectively. In order to identify high-risk patients, we next took AJCC stage IIIB, AJCC stage IIIC, AJCC T3, AJCC T4 as independent variables respectively. Univariate and Multivariate analysis was also used and showed that AJCC T3 and T4, were independent prognostic factors for OS. In addition, the patients with AJCC T4 have the worst prognosis. Surprisingly, we found that PMRT still have some survival benefit on OS and CSS in patients with AJCC T4.
As we all know, radiation technology has been advancing over the past few years. The accumulation of radiation experience and the development of technology also play important roles in improving prognosis of patients. Secondly, we screened the breast cancer patients with four or more positive lymph nodes after PMRT and validated the previous prognostic model in recent few years between 2006 and 2009. The results also showed the overall survival rate was lower if the patients underwent PMRT with the higher NRF score, and PMRT also have survival benefit on OS and CSS in patients with AJCC T4.
This study also has several limitations. Firstly, some studies have showed that the systemic therapy may bring some substantial survival benefits for PMRT [30–32]. However, due to the absence of information on chemotherapy or targeted therapy included in the SEER database, its effect on survival could not be evaluated. Secondly, this study is the non-randomized study and the intrinsic defects exist in any retrospective study. Thirdly, some factors that obviously influence the prognosis of breast cancer patients, such as the number of negative lymph nodes, Her2 status, were not included in our study. Given the limitations of the SEER dataset. Therefore, future prospective studies from different countries and regions are needed to further confirm these results.
In conclusion, our study demonstrated that all patients with four or more positive lymph nodes after modified radical mastectomy need be treated with PMRT even the patients with AJCC T4.
MATERIALS AND METHODS
Patient selection
The SEER Cancer Statistics Review (http://seer.cancer.gov/data/citation.html) is published annually by the Data Analysis and Interpretation Branch of the National Cancer Institute, MD, USA. A total of 18 population-based cancer registries in the United States were included in the current SEER database [7]. The SEER*Stat software (SEER*Stat 8.2.1) was used to identify the appropriate patients. Using this software, we first screened breast cancer patients after PMRT between 1998 and 2001 to determine the risk factors. Then we validated these risk factors between 2006 and 2009 and ultimately identify the breast cancer patients who are not likely to benefit from PMRT. The included patients should meet the following criteria: the diagnosis was confirmed microscopically, and they should be female with the confirmed age, active follow-up and only one primary tumor. In addition, the patients should be those who have received modified radical mastectomy, with at least four positive lymph nodes removed. Patients with benign or borderline tumors, unknown age, unknown cause of death, and unknown survival months were all excluded.
Ethics statement
This study was mainly based on the SEER database and was conducted in compliance with the Helsinki Declaration. We obtained permission to access the files of SEER program research data and the reference number is 11824-Nov2014. The informed consent was not required because personal identifying information was not involved. This study was approved by the ethics committee of the Shandong Cancer Hospital affiliated to Shandong University.
Statistical analysis
For all the patients, the following variables were analyzed: Age, Laterality, AJCC stage, AJCC T, AJCC N, Grade, ER status, PR status. In addition, the OS and CSS were regarded as the primary endpoint of this study and extracted from the SEER database. χ2 tests were used to compare the patient baseline characteristics. The Kaplan-Meier analyses were used to generate the survival curves and the Log Rank test was applied to analyze the differences among the curves. Comparative risks of mortality were evaluated using univariate and multivariate Cox proportional hazards regression models. All statistical tests were two-sided, and a P < 0.05 was considered statistically significant. The statistical software SPSS 18.0 (SPSS, IL, Chicago) was used for all data analysis.
ACKNOWLEDGMENTS
We thank Huiying Chi (Shanghai Geriatric Institute of Chinese Medicine, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai) for statistical support.
CONFLICTS OF INTEREST
All authors have reviewed the final version of the manuscript and approve it for publication. This manuscript has not been published in whole or in part nor is it being considered for publication elsewhere. The authors have no conflicts of interest to declare.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65: 87-108.
2. Jagsi R. Progress and controversies: radiation therapy for invasive breast cancer. CA Cancer J Clin. 2014; 64: 135-152.
3. Stecklein SR, Shen X, Mitchell MP. Post-Mastectomy Radiation Therapy for Invasive Lobular Carcinoma: A Comparative Utilization and Outcomes Study. Clin Breast Cancer. 2016; [Epub ahead of print].
4. Rusthoven CG, Rabinovitch RA, Jones BL, Koshy M, Amini A, Yeh N, Jackson MW, Fisher CM. The Impact of Postmastectomy and Regional Nodal Radiation after Neoadjuvant Chemotherapy for Clinically Lymph Node Positive Breast Cancer: A National Cancer Database (NCDB) Analysis. Ann Oncol. 2016. [Epub ahead of print].
5. Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F, Kjaer M, Gadeberg CC, Mouridsen HT, Jensen MB, Zedeler K. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. N Engl J Med. 1997; 337: 949-955
6. Wu SG, Sun JY, Zhou J, Li FY, Zhou H, Lin Q, Lin HX, Bao Y, He ZY. Number of negative lymph nodes can predict survival of breast cancer patients with four or more positive lymph nodes after postmastectomy radiotherapy. Radiat Oncol. 2014; 9: 284.
7. Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence-SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2014 Sub (1973-2012 varying)-Linked To County Attributes-Total U.S., 1969-2013 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2015, based on the November 2014 submission.
8. Tapley ND, Spanos WJ Jr, Fletcher GH, Montague ED, Schell S, Oswald MJ. Results in patient with breast cancer treated by radical mastectomy and post-operative irradiation with no adjuvant chemotherapy. Cancer. 1982; 49; 1316-1319.
9. Host H, Brennhovd IO. The effect of postoperative radiotherapy in breast cancer. Int J Radiat Oncol Biol Phys. 1977; 2: 1061-1067.
10. Fisher B, Slack NH, Cavanaugh PJ, Gardner B, Ravdin RG. Postoperative radiotherapy in the treatment of breast cancer: results of the NSABP clinical trial. Ann Surg.1970; 172: 711-732.
11. Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, Andersson M, Kamby C, Kjaer M, Gadeberg CC, Rasmussen BB, Blichert-Toft M, Mouridsen HT. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999; 353: 1641-1648.
12. Ragaz J, Olivotto IA, Spinelli JJ, Phillips N, Jackson SM, Wilson KS, Knowling MA, Coppin CM, Weir L, Gelmon K, Le N, Durand R, Coldman AJ, et al. Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial. J Nat Cancer Inst. 2005; 97: 116-126.
13. Whelan TJ, Julian J, Wright J, Jadad AR, Levine ML. Does locoregional radiation therapy improve survival in breast cancer? A meta-analysis. J Clin Oncol. 2000; 18: 1220-1229.
14. Nagar H, Boothe D, Ginter PS, Sison C, Vahdat L, Shin S, Smith M, Chao KS, Nori D, Hayes MK. Disease-free survival according to the use of postmastectomy radiation therapy after neoadjuvant chemotherapy. Clin Breast Cancer. 2015; 15: 128-34.
15. Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, Godwin J, Gray R, Hicks C, James S, MacKinnon E, McGale P, McHugh T, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005; 366: 2087-2106.
16. Somner JE, Dixon JM, Thomas JS. Node retrieval in axillary lymph node dissections: recommendations for minimum numbers to be confident about node negative status. J Clin Pathol. 2004; 57: 845-848.
17. Wiznia LE, Lannin DR, Evans SB, Hofstatter EW, Horowitz NR, Killelea BK, Tsangaris TN, Chagpar AB. The number of lymph nodes dissected in breast cancer patients influences the accuracy of prognosis. Ann Surg Oncol. 2014; 21: 389-394.
18. Karlsson P, Cole BF, Price KN, Coates AS, Castiglione-Gertsch M, Gusterson BA, Murray E, Lindtner J, Collins JP, Holmberg SB, Fey MF, Thürlimann B, Crivellari D, et al. The role of the number of uninvolved lymph nodes in predicting locoregional recurrence in breast cancer. J Clin Oncol. 2007; 25: 2019-2026.
19. Kuru B. Prognostic significance of total number of nodes removed, negative nodes removed, and ratio of positive nodes to removed nodes in node positive breast carcinoma. Eur J Surg Oncol. 2006; 32: 1082-1088.
20. Katz A, Strom EA, Buchholz TA, Thames HD, Smith CD, Jhingran A, Hortobagyi G, Buzdar AU, Theriault R, Singletary SE, McNeese MD. Locoregional recurrence patterns after mastectomy and doxorubicin-based chemotherapy: implications for postoperative irradiation. J Clin Oncol. 2000; 18: 2817-2827.
21. Taghian A, Jeong JH, Mamounas E, Anderson S, Bryant J, Deutsch M, Wolmark N. Patterns of locoregional failure in patients with operable breast cancer treated by mastectomy and adjuvant chemotherapy with or without tamoxifen and without radiotherapy: results from five National Surgical Adjuvant Breast and Bowel Project randomized clinical trials. J Clin Oncol. 2004; 22: 4247-4254.
22. Truong PT, Olivotto IA, Kader HA, Panades M, Speers CH, Berthelet E. Selecting breast cancer patients with T1-T2 tumors and one to three positive axillary nodes at high postmastectomy locoregional recurrence risk for adjuvant radiotherapy. Int J Radiat Oncol Biol Phys. 2005; 61: 1337-1347.
23. Wenz F, Sperk E, Budach W, Dunst J, Feyer P, Fietkau R, Haase W, Harms W, Piroth MD, Sautter-Bihl ML, Sedlmayer F, Souchon R, Fussl C, et al. Breast Cancer Expert Panel of the German Society of Radiation Oncology (DEGRO): DEGRO practical guidelines for radiotherapy of breast cancer IV: radiotherapy following mastectomy for invasive breast cancer. Strahlenther Onkol. 2014; 190: 705-714.
24. EBCTCG (Early Breast Cancer Trialists' Collaborative Group), McGale P, Taylor C, Correa C, Cutter D, Duane F, Ewertz M, Gray R, Mannu G, Peto R, Whelan T, Wang Y, Wang Z, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet. 2014; 383: 2127-2135.
25. Wu S, Li Q, Zhou J, Sun J, Li F, Lin Q, He Z. Post-mastectomy radiotherapy can improve survival in breast cancer patients aged 35 years or younger with four or more positive nodes but not in one to three positive nodes. Ther Clin Risk Manag. 2014; 10: 867-74.
26. Li Q, Wu S, Zhou J, Sun J, Li F, Lin Q, Guan X, Lin H, He Z. Risk factors for locoregional recurrence after postmastectomy radiotherapy in breast cancerpatients with four or more positive axillary lymph nodes. Curr Oncol. 2014; 21: e685-90.
27. Nagao T, Kinoshita T, Tamura N, Hojo T, Morota M, Kagami Y. Locoregional recurrence risk factors in breast cancer patients with positive axillary lymph nodes and the impact of postmastectomy radiotherapy. Int J Clin Oncol. 2013; 18: 54-61.
28. Wu SG, He ZY, Li Q, Li FY, Lin Q, Lin HX, Guan XX. redictive value of breast cancer molecular subtypes in Chinese patients with four or more positive nodes after postmastectomy radiotherapy. Breast. 2012; 21: 657-661.
29. Yu JI, Park HC, Lim do H, Park W, Yoo BC, Paik SW, Koh KC, Lee JH. Prognostic index for portal vein tumor thrombosis in patients with hepatocellular carcinoma treated with radiation therapy. J Korean Med Sci. 2011; 26: 1014-22.
30. Bellon JR, Harris JR. Chemotherapy and radiation therapy for breast cancer: what is the optimal sequence? J Clin Oncol. 2005; 23: 5-7.
31. Liu J, Mao K, Jiang S, Jiang W, Chen K, Kim BY, Liu Q, Jacobs LK. The role of postmastectomy radiotherapy in clinically node-positive, stage II-III breast cancer patients with pathological negative nodes after neoadjuvant chemotherapy: an analysis from the NCDB. Oncotarget. 2016; 7:24848-24859. doi: 10.18632/oncotarget.6664.
32. Whelan TJ, Julian J, Wright J, Jadad AR, Levine ML. Does locoregional radiation therapy improve survival in breast cacner? A meta-analysis. J Clin Oncol. 2000; 18: 1220-1229.