
INTRODUCTION
Prostate cancer (PCa) is the second most frequently diagnosed cancer among men, and is the fifth leading cause of cancer-related death worldwide [1]. For most men with organ-confined PCa, radical prostatectomy (RP) provides effective oncologic outcomes [2]. The trifecta of optimal outcomes after RP includes preservation of urinary continence, potency and oncologic control [3], and is only achieved in 62–70% of patients [3, 4]. Despite improved surgical techniques, urinary incontinence remains a major postoperative complication, significantly affecting quality of life (Qol) in many men [5, 6]. On average, 16% of men are incontinent 12 months post surgery (using a no-pad definition) [7]. Post-RP incontinence may result in patient preoccupation with leakage avoidance and/or bathroom locations, and feelings of helplessness and embarrassment [8, 9].
To refine the RP technique, Azuma and coworkers [10] suggested a novel surgical approach incorporating “seven key elements of operative skill for the early recovery of urinary continence” (“7 key elements”). Bladder neck preservation (BNP), first introduced in 1992 by Klein [11], has been proposed as a method to accelerate continence recovery, as BNP during RP promotes early return of urinary continence and erectile function [12–16]. However, some clinical trials have suggested little difference in the return of continence with BNP [17–19], and risk of a positive surgical margin (PSM) may be increased [18, 20–22].
The primary objective of this study was to conduct a systematic review and meta-analysis to evaluate the effectiveness of BNP for improving post-RP urinary continence outcomes. The secondary objective was to assess whether or not BNP compromises surgical margin clearance and increases PCa recurrence rate.
RESULTS
Characteristics of eligible studies
Thirteen studies with 2284 total participants (1130 cases and 1154 controls) fulfilled the predefined inclusion criteria and were considered suitable for meta-analysis, including two RCTs [18, 23], six prospective [24–29] and five retrospective [19, 30–33] studies (Figure 1).
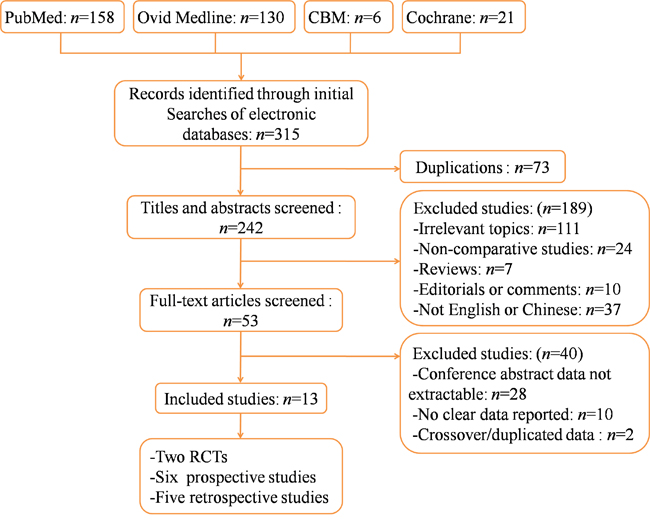
Figure 1: Flow chart illustrating identification and screening of studies. RCT, randomized controlled trial.
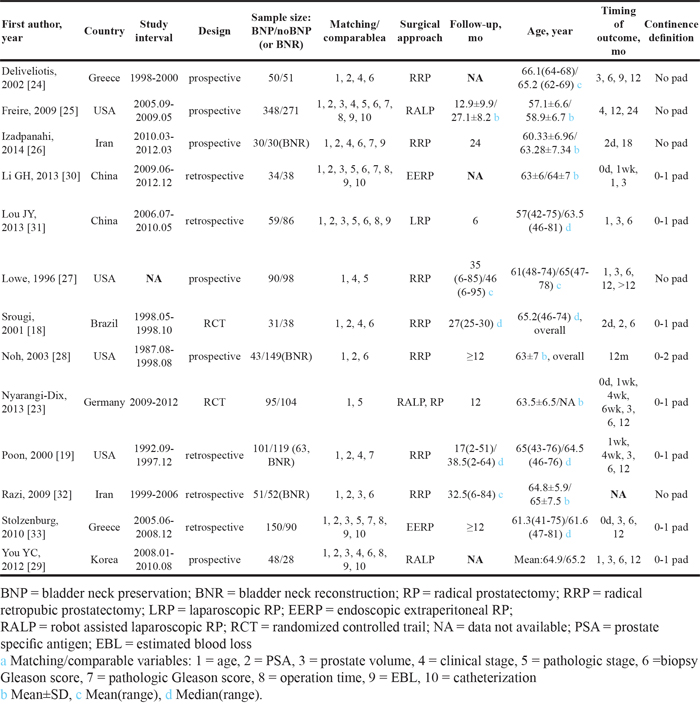
Study sample sizes ranged between 60 [26] and 619 [25]. Studies were conducted between 1987 and 2012. One prospective study [28] was conducted from August 1987 to August 1998: tennis racquet reconstruction (TRR) was performed from 1987 to 1995 and BNP from 1995 to 1996. Surgical approaches included open, laparoscopic and robot-assisted. Most of the included studies reported BNP versus noBNP (resection or unspecified), and others compared BNP to BNR. One study [19] reported BNP versus BNR and noBNP independently. Baseline continence was poorly reported. Approximately half of the included studies used a no-pad definition for continence; others used a 0–1 pad definition; only one study [28] defined continence as 0–2 pads per day. Timing of continence assessment and reporting ranged from immediately after catheter removal [23, 30, 33] to 24 mo [25].
Demographics, comparative variables of BNP vs. control (noBNP or BNR), continence definitions and follow-up times were extracted individually from each study (Table 1).
Table 1: Characteristics of included studies
Demographic and clinical baseline characteristics
There were no significant differences with respect to age, PSA, clinical stage, pathologic stage, biopsy Gleason score or pathologic Gleason score (Table 2). BNP was more commonly performed in smaller-sized prostates (WMD = -2.24 ml; 95% CI, -4.27 to -0.22; P = 0.03). There was no significant prostate volume heterogeneity between studies (Chi2 = 0.34, df = 4, I2 = 0%; P = 0.99) (Figure 2).
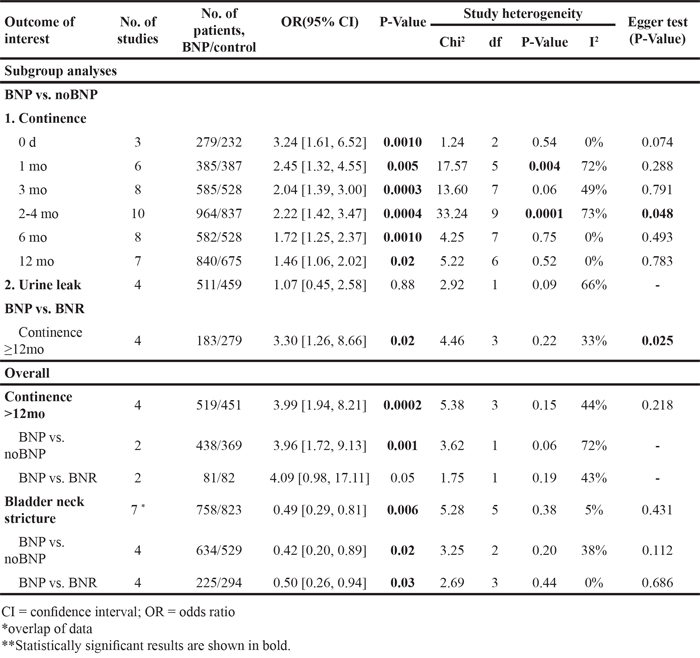
Table 2: Analyses of demographic, clinical, pathologic and perioperative characteristics, and oncologic control comparison
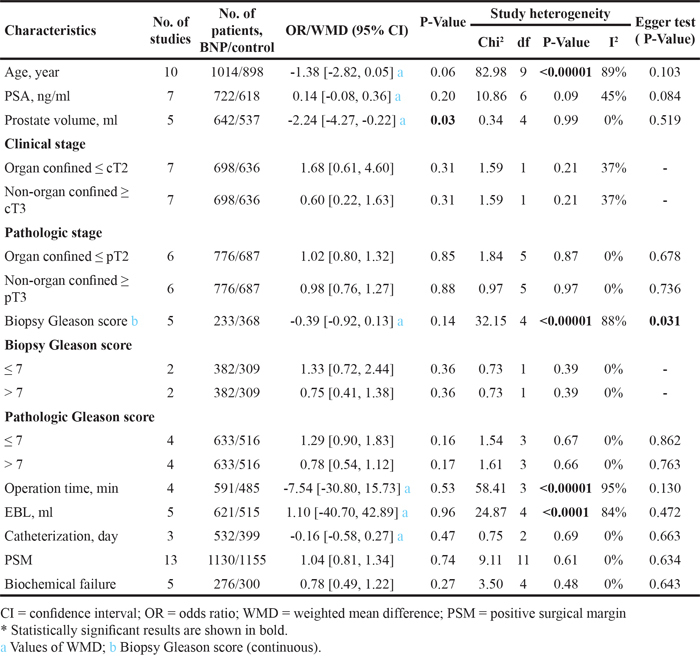
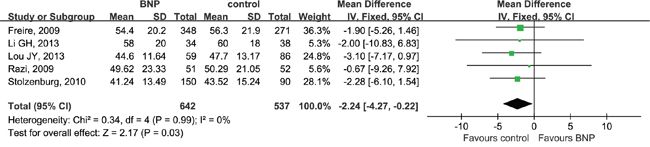
Figure 2: Forest plot of prostate volume. CI, confidence interval; IV, inverse variance; BNP, bladder neck preservation; SD, standard deviation. A fixed-effects meta-analysis was conducted (P >0.05, heterogeneity).
Perioperative variables
We extracted operation times from four studies, estimated blood loss (EBL) from five studies, and length of catheterization from three studies. No differences were observed between BNP and control (noBNP or BNR) with respect to operation time (WMD = -7.54 min; 95% CI, -30.80 to 15.73; P = 0.53), EBL (WMD = 1.10 ml; 95% CI, -40.70 to 42.89; P = 0.96) or length of catheterization (WMD = -0.16 d; 95% CI, -0.58 to 0.27; P = 0.47) (Table 2).
Relevant complications
Data pooled from seven studies with 1581 total patients with bladder neck stricture associated BNP with lower stricture rates (OR = 0.49; 95% CI, 0.29–0.81; P = 0.006) (Table 3). Subgroup analyses according to surgery type showed differences between BNP and noBNP (OR = 0.42; 95% CI, 0.20–0.89; P = 0.02) or BNR (OR = 0.50; 95% CI, 0.26–0.94; P = 0.03) (Figure 3). In view of one study [19] reported BNP vs. BNR and noBNP independently, the total effect were not calculated directly in Figure 3 but shown in Table 3. There were no differences between BNP and noBNP in urine leak (OR = 1.07; 95% CI, 0.45–2.58; P = 0.88).
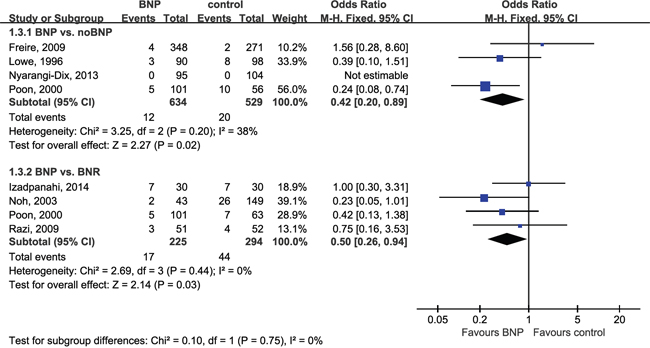
Figure 3: Forest plot of bladder neck stricture. CI, confidence interval; M-H, Mantel-Haenszel; BNP, bladder neck preservation; BNR, bladder neck reconstruction. A fixed-effects meta-analysis was conducted (P >0.05, heterogeneity).
Table 3: Continence-related outcomes comparison
Urinary continence
Patients who had BNP surgery had better early and long-term (12 mo) continence outcomes as compared with noBNP (resection or unspecified) surgery (Figure 4). ORs were 3.24 (95% CI, 1.61–6.52; P = 0.0010) at 0 d, 2.45 (1.32–4.55; P = 0.005) at 1 mo, 2.04 (1.39–3.00; P = 0.0003) at 3 mo, 2.22 (1.42–3.47; P = 0.0004) at 2–4 mo, 1.72 (1.25–2.37; P = 0.0010) at 6 mo, and 1.46 (1.06–2.02; P = 0.02) at 12 mo. A difference in continence outcomes with BNP compared to BNR was seen at ≥12mo (OR = 3.30; 95% CI, 1.26–8.66; P=0.02; Figure 5A). Continence differences between BNP and BNR groups at other time points were not subjected to cumulative analysis due to poorly reported data.
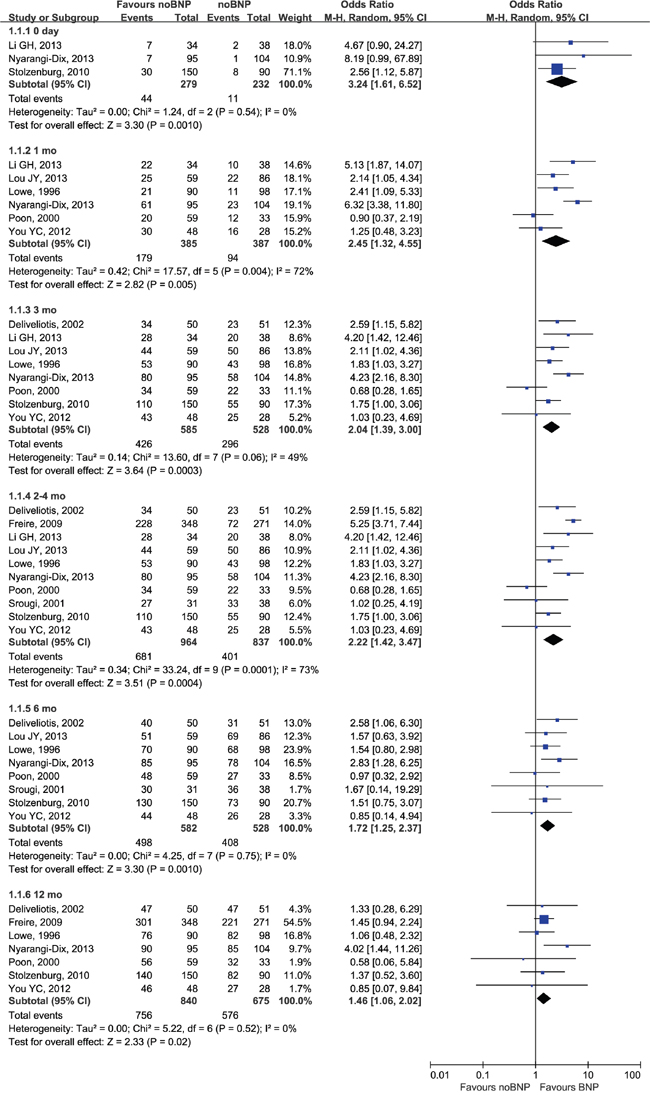
Figure 4: Forest plot of continence rates for BNP vs. noBNP. CI, confidence interval; M-H, Mantel-Haenszel; BNP, bladder neck preservation. A random-effects meta-analysis was conducted (P <0.05, heterogeneity).
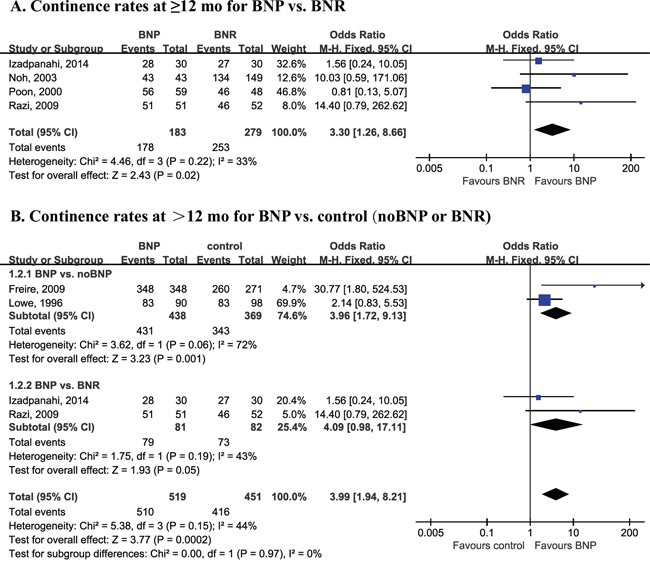
Figure 5: Forest plot of long-term continence outcomes. CI, confidence interval; M-H, Mantel-Haenszel; BNP, bladder neck preservation; BNR, bladder neck reconstruction. A fixed-effects meta-analysis was conducted (P >0.05, heterogeneity).
Four studies reported long-term results (>12 mo), including 18 and 24 mo. Patients who underwent BNP had better long-term (>12 mo) continence outcomes compared with noBNP or BNR (Table 3). OR was 3.99 (1.94–8.21; P = 0.0002; Figure 5B) at >12 mo. Subgroup analyses according surgery type demonstrated differences between BNP and noBNP (OR = 3.96; 95% CI, 1.72–9.13; P = 0.001) in continence rate at >12 mo; no difference was seen at >12 mo with BNP compared to BNR (OR = 4.09; 95% CI, 0.98–17.11; P = 0.05).
Oncologic control
Patients with or without BNP had similar PSM outcomes (OR = 1.04; 95% CI, 0.81–1.34; P = 0.74) and biochemical failure rates (OR = 0.78; 95% CI, 0.49–1.22; P = 0.27) (Table 2). Biochemical failure rates were extracted from five studies. However, the definitions of biochemical failure were inconsistent: one study [26] set PSA level limits to 0.4 ng/ml; two [18, 27] set these to 0.3 ng/ml; one [32] set this to 0.2 ng/ml; and one [19] did not mention limits.
Sensitivity analysis and publication bias
Sensitivity analysis was carried out for prospective studies. There was no change in significance for any outcomes in sensitivity analysis. The funnel plots and Egger test revealed that publication bias existed in only three (Biopsy Gleason score [continuous], continence at 2–4 mo, and continence at ≥12mo) of the 27 comparisons performed in the present analysis (Table 2, 3).
DISCUSSION
In this systematic review, we analyzed thirteen trials (1130 cases and 1154 controls) to evaluate the efficacy of BNP on urinary continence and its effect on oncologic outcomes. Our meta-analysis included two RCTs, six prospective and five retrospective studies, and demonstrated that BNP surgery improved early recovery and overall long-term (1 year) urinary continence outcomes, decreased bladder neck stricture rates and was effective in eradicating PCa without increasing recurrence rate.
Radical prostatectomy provides effective oncologic control for most men with localized PCa [2]. Despite improved surgical techniques, urinary incontinence remains a chief postoperative complication and affects quality of life in many men [5, 6]. The pathophysiology of post-RP urinary incontinence is not clearly demonstrated. Moreover, the precise anatomy of the bladder neck (BN) and its effect on continence have proven difficult to clarify. The male urethral sphincter complex, composed of an inner smooth muscle lissosphincter and an outer skeletal muscle rhabdosphincter, is essential to continence. In normal physiology, the external urethral sphincter (rhabdosphincter) maintains active continence during stress, whereas the internal urinary sphincter (lissosphincter) provides passive continence at rest [34]. The BN is composed of two different muscles, the ventrolateral and dorsal longitudinal muscles, which are positioned obliquely. In a truly transverse direction of the BN, there is a distinct circular muscle called the musculus sphincter vesicae [35, 36], also named internal urinary sphincter or preprostatic sphincter. In most cases, post-RP incontinence is the result of rhabdosphincter insufficiency [37, 38]. The effect of BNP on early continence outcomes could possibly be explained by preservation of the musculus sphincter vesicae [39], which constitutes an integral part of the male urethral sphincter complex. Additionally, obtaining a BN diameter approximately equal to the diameter of the urethral stump simplifies [40].
Since the first reported anatomic RP, several surgical technique modifications have been proposed to improve early continence recovery and continence outcomes [15, 28, 41, 42]. Some surgeons have attempted to reconstruct the bladder neck by tubularization [43]. Klein [11] first reported the association of BNP with improved early continence. In a multivariate analysis, Sakai et al. [44] reported BNP as the only independent predictor of return to continence at 1 and 3 mo. These results were verified by Gacci et al. [13]. However, other variables such as preoperative pelvic floor muscle exercises and preservation of the neurovascular bundles (NVB) may also influence early continence recovery [45, 46]. Application of preoperative and postoperative continence rehabilitative programs is difficult to control for and was poorly reported in the included studies. Thus, it is unclear if patient groups in each study received these interventions equally.
The effect of BNP on long-term (1 year) continence outcomes has been controversial. Some trials found long-term continence rate benefits from BNP [26, 32, 47], while others did not [24, 28]. This meta-analysis demonstrated improved long-term continence outcomes for patients who had BNP surgery compared with those who had noBNP or BNR (>12 mo, OR = 3.99; P = 0.0002). As comparative data were poorly reported, differences between BNP and BNR groups at other time points were not analyzed except for ≥12 mo. However, the funnel plots and Egger test (Table 3) indicated that publication biases existed in two outcomes: continence at 2–4 mo and ≥12 mo.
Benefits from BNP as compared to controls (noBNP or BNR) with respect to early recovery and overall long-term continence suggest that the bladder neck itself is essential to continence. However, these results are limited by relatively small sample sizes in these analyses.
In addition, type 2 diabetes, baseline continence, different surgical approaches, presenceof other interventions, surgeon experience, surgical technique variations, definition of BNP status, selective outcome reporting and patients lost to follow-up represent risks of bias that could not be controlled for in our analysis. Patients with type 2 diabetes need longer to return to continence than non-diabetics, though this may not affect overall continence [48]. Decreased surrounding tissue damage as a result of careful dissection may also improve urethral preservation and protect supporting continence structures. NVB and urethral length preservation are correlated with improved continence outcomes [46, 49], and highlight the importance of having a detailed knowledge of prostatic and surrounding anatomy in optimal post-RP outcomes. Stolzenburg et al. [50] previously provided an exemplary review of surgical anatomy for RP. Compared with radical retropubic prostatectomy (RRP), patients appeared to benefit from more precise robot-assisted laparoscopic RP (RALP) [51].
Our meta-analysis found no differences between studies regarding patient age, PSA, clinical stage, pathological stage, biopsy Gleason score, pathologic Gleason score, operation time, EBL or length of catheterization. Consequently, our included studies appeared well matched, although variable biopsy Gleason scores (continuous) revealed publication bias.
Selection bias may exist for patients who had BNP, as surgeons may choose patients who are generally fitter to ensure technical ease of preservation. In our meta-analysis, the BNP group had a smaller average prostate size (WMD = -2.24 ml; P = 0.03), which revealed potential bias in selection of patients with low prostate volume. There was no significant heterogeneity between included studies (P = 0.99) that reported prostate size. However, none of the observed differences were seen across all studies. According to a study by Pettus et al. [52], prostate volume is associated with surgical challenges, but not continence outcome after RP.
Heterogeneity existed between studies in terms of operation time (P <0.00001) and EBL (P <0.0001). These could be attributed to differences in surgical approaches, technique, surgeon experience and so on.
Bladder neck strictures are a relatively common, manageable RP complication [26]. PCa patients having BNP surgery may benefit from lower stricture rates (OR = 0.49; P = 0.006). Subgroup analyses demonstrated bladder neck stricture differences in BNP vs. noBNP (OR = 0.42; P = 0.02) and BNP vs. BNR (OR = 0.50; P = 0.03). During reconstruction of the bladder neck (usually a tennis racket method), pressure and tension on the bladder neck tissue due to suture and distortion of normal bladder neck anatomy can promote bladder neck strictures [26]. BNP is also associated with lower rates of ureteral injury [53], which can lead to stricture. Additionally, a larger bladder neck diameter post-RP can result in the need for time-consuming, reconstructive tapering, which may increase susceptibility to anastomotic leak as a result of the longer suture line [25].
With regard to oncologic results, this meta-analysis revealed that patients who underwent BNP had similar outcomes with respect to positive surgical margins (PSM) (OR = 1.04; P = 0.74) and biochemical failure (OR = 0.78; P = 0.27). Some authors argue that BNP surgery may increase the likelihood of PSM [18, 20–22]. However, a randomized controlled trial [23] and other studies [14, 16, 54–56] showed that BNP does not compromise oncologic control. Golabek et al. [16] found that the relatively high incidence of PSM could be due to a large number of extracapsular disease cases.
A major limitation of this study was the small number of well-designed prospective studies. First, there are only two RCTs included in our analysis, along with the six prospective and five retrospective studies. Second, analysis was limited to English- or Chinese-language publications and only published results were included. Third, short follow-up time in some patients, marked heterogeneity for several continuous variables and potential patient selection bias may have influenced the confidence of our results to varying degrees. Additionally, one well-designed study [14] including 1067 patients was not included in the meta-analysis due to absence of discrete data on continence and biochemical recurrence.
To the best of our knowledge, this is the first meta-analysis comparing BNP and noBNP (or BNR) conducted using this type of systematic approach. We applied stringent inclusion criteria to identify studies and compare the two procedures, the Egger test to assess publication bias and sensitivity analysis to minimize the effects of heterogeneity. We provide up-to-date information on the impacts of BNP during RP as compared with traditional techniques. Despite our rigorous systematic approach, because of the inherent limitations of the included studies and the absence of long-term outcomes, further large, prospective, multi-centric, long-term follow-up studies and RCTs should be undertaken to confirm our findings.
MATERIALS AND METHODS
Data sources and search strategies
A systematic search of PubMed, Ovid Medline, Embase, CBM and the Cochrane Central Register of Controlled Trials (Cochrane Library) was conducted (February 2016) to identify potentially relevant studies that assessed the association between BNP and post-RP urinary continence. The search was limited to studies published in or after 1992, as BNP surgery was not formally described before that time.
The following terms were searched: [“bladder neck preservation” OR “bladder neck sparing”] AND [“prostatic neoplasms” OR ‘‘prostate tumor’’ OR ‘‘prostate cancer’’ OR ‘‘prostatectomy” OR ‘‘radical prostatectomy’’] AND [‘‘urinary incontinence’’ OR ‘‘continence’’ OR ‘‘postoperative complications’’]. The ‘‘related articles’’ or similar function was used to broaden the search, and all abstracts, studies and citations were reviewed.
Inclusion and exclusion criteria
Articles were further refined through a filtering process based upon the following eligibility criteria: (1) Participants: All subjects were men formally diagnosed with PCa, who underwent radical prostatectomy. (2) Interventions: BNP techniques were defined as bladder neck preservation or bladder neck sparing in radical prostatectomy. (3) Controls: Non-BNP (bladder neck resection or unspecified, noBNP) and active (bladder neck reconstruction, BNR) control conditions were both considered. (4) Outcomes: The primary outcome was urinary continence. (5) Studies: Only controlled trials were considered, including randomized controlled trials (RCT) and non-randomized clinical studies. When multiple publications from the same institution and/or authors with potentially overlapping patient samples were identified, the most recent and/or informative study was included unless the articles were reporting on different outcomes or populations.
Studies were excluded from the meta-analysis if: (1) the inclusion criteria were not met, (2) no outcomes of interest (specified later) were reported or it was impossible to calculate or extrapolate the necessary data from the published results, (3) studies were single-cohort or cross-sectional, (4) the publication language was not English or Chinese.
Study selection and data extraction
Two reviewers (Xueyou Ma and Kun Tang) separately screened all search results (titles and abstracts). The full text of any potentially relevant publication was retrieved for review and studies were selected based on the criteria previously outlined.
Data were extracted and studies analyzed by two independent reviewers using a standardized data collection form designed by the authors. Any disagreement regarding study selection or analysis was resolved through discussion and consultation with a third reviewer (Zhihua Wang) to reach a consensus. In all cases of missing or incomplete data, the corresponding authors were contacted, but no additional information was provided.
The following data were extracted including: first author, year of publication, country, study interval, study design, number of patients who underwent BNP or noBNP or BNR, surgical approach, baseline characteristics of the study population and outcomes of interest.
Outcomes of interest
The clinical outcomes that were analyzed and compared between BNP and noBNP or BNR included patient baseline characteristics (age, prostate specific antigen [PSA], prostate volume, clinical stage and pathology results [pathologic stage, biopsy Gleason score, pathologic Gleason score]) and perioperative outcomes (operation time, estimated blood loss [EBL], length of catheterization and relevant complications). Relevant complications included urine leak and bladder neck stricture.
The primary outcome of this review was postoperative urinary continence and the effect of BNP on the timing of urinary continence return after RP. Outcome timing categories (0d, 1, 3, 2–4, 6, 12 and >12 mo) were selected based on all available results. The secondary outcome was evaluation of oncologic control through positive surgical margin (PSM) and biochemical failure.
Some variables were deemed unsuitable for cumulative analysis due to small study numbers. These variables included body mass index (BMI), duration of hospital stay, lymphadenopathy and previous radiotherapy history.
Statistical analysis
The present meta-analysis was conducted according to the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses (QUOROM) guidelines [57]. The weighted mean differences (WMD) and the odds ratios (OR) were used to evaluate continuous and dichotomous variables, respectively. All outcomes were expressed with 95% confidence intervals (CI). For continuous variables (eg, age and length of catheterization), we calculated the difference in mean values and the 95% CI between BNP and control (noBNP or BNR). This method required that studies represent the standard errors of the mean (SEM), the standard deviations (SD) or the CIs. However, some studies did not express any of these parameters, but reported continuous data as medians and ranges. In these cases, we made an approximate transformation using the technique described by Hozo [58]. For dichotomous variables derived from contingency tables (eg, continence rate), ORs and 95% CI were computed. If data were presented as percentages, raw numbers were calculated. An OR significantly <1.0 favored control groups (noBNP and BNR), whereas an OR significantly >1.0 favored BNP groups. All P values are two-tailed with P <0.05 representing statistical significance.
A Mantel-Haenszel fixed-effects (FE) meta-analysis was conducted for dichotomous variable, and Inverse Variance (IV) FE for continuous variable. The quantity of heterogeneity was evaluated using chi-squared and I2 statistics with significance set at P <0.05. In cases where higher I2 and chi-squared statistic values indicated increasing inconsistency between studies and significant inter-study heterogeneity, a random-effects (RE) model was adopted. Funnel plots and the Egger test of funnel plot symmetry were used to evaluate publication bias.
In forest plots, vertical lines represent the null hypothesis (OR = 1.0), each square represents the point estimate of the OR, and the size of the square represents its relative weighting in the meta-analysis. 95% CIs are depicted by horizontal lines.
Sensitivity analysis was performed by considering studies with RCT or studies clearly of a prospective design. Subgroup analyses according to surgery type (noBNP or BNR) were conducted. Variables were pooled only if studies numbered more than three in the overall meta-analysis.
Statistical analyses were conducted and forest plots generated using Review Manager (RevMan) 5.3 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). The Egger test was performed using the metabias procedure in STATA12.0 (StataCorp, College Station, TX).
CONFLICTS OF INTEREST
All authors declare that there are no conflicts of interest.
GRANT SUPPORT
This work was supported by the National Natural Science Foundation of China (NSFC No.81101944 & No. 81173608), the “12th Five-year Plan” for Sci&Tech Research of China (No. 2012BAI10B01) and the Major Science and Technology Innovation Plan of Hubei Province (No. 2014AEA048).
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA: A Cancer Journal for Clinicians. 2015; 65:87-108.
2. Sooriakumaran P, Nyberg T, Akre O, Haendler L, Heus I, Olsson M, Carlsson S, Roobol MJ, Steineck G, Wiklund P. Comparative effectiveness of radical prostatectomy and radiotherapy in prostate cancer: observational study of mortality outcomes. The BMJ. 2014; 348:g1502.
3. Eastham JA, Scardino PT, Kattan MW. Predicting an Optimal Outcome after Radical Prostatectomy: The “Trifecta” Nomogram. J Urol. 2008; 179:2207-2211.
4. Patel VR, Sivaraman A, Coelho RF, Chauhan S, Palmer KJ, Orvieto MA, Camacho I, Coughlin G, Rocco B. Pentafecta: A New Concept for Reporting Outcomes of Robot-Assisted Laparoscopic Radical Prostatectomy. Eur Urol. 2011; 59:702-707.
5. Cambio AJ, Evans CP. Minimising Postoperative Incontinence Following Radical Prostatectomy: Considerations and Evidence. Eur Urol. 2006; 50:903-913.
6. Kojima Y, Takahashi N, Haga N, Nomiya M, Yanagida T, Ishibashi K, Aikawa K, Lee DI. Urinary incontinence after robot-assisted radical prostatectomy: Pathophysiology and intraoperative techniques to improve surgical outcome. Int J Urol. 2013; 20:1052-1063.
7. Ficarra V, Novara G, Rosen RC, Artibani W, Carroll PR, Costello A, Menon M, Montorsi F, Patel VR, Stolzenburg J, Van der Poel H, Wilson TG, Zattoni F, Mottrie A. Systematic Review and Meta-analysis of Studies Reporting Urinary Continence Recovery After Robot-assisted Radical Prostatectomy. Eur Urol. 2012; 62:405-417.
8. Miller DC, Sanda MG, Dunn RL, Montie JE, Pimentel H, Sandler HM, McLaughlin WP, Wei JT. Long-term outcomes among localized prostate cancer survivors: health-related quality-of-life changes after radical prostatectomy, external radiation, and brachytherapy. J Clin Oncol. 2005; 23:2772-2780.
9. Clark JA, Inui TS, Silliman RA, Bokhour BG, Krasnow SH, Robinson RA, Spaulding M, Talcott JA. Patients’ perceptions of quality of life after treatment for early prostate cancer. J Clin Oncol. 2003; 21:3777-3784.
10. Azuma H, Ibuki N, Inamoto T, Koyama K, Utimoto S, Fujisue Y, Mizutani Y, Nomi H, Ubai T, Katsuoka Y. Utility of transrectal ultrasonography guidance and seven key elements of operative skill for early recovery of urinary continence after laparoscopic radical prostatectomy. Int J Oncol. 2011; 38:293-304.
11. Klein EA. Early continence after radical prostatectomy. J Urol. 1992; 148:92-95.
12. Harris MJ. The anatomic radical perineal prostatectomy: an outcomes-based evolution. Eur Urol. 2007; 52:81-88.
13. Gacci M, Carini M, Simonato A, Imbimbo C, Gontero P, Briganti A, De Cobelli O, Fulcoli V, Martorana G, Nicita G, Mirone V, Carmignani G. Factors predicting continence recovery 1 month after radical prostatectomy: results of a multicenter survey. Int J Urol. 2011; 18:700-708.
14. Friedlander DF, Alemozaffar M, Hevelone ND, Lipsitz SR, Hu JC. Stepwise description and outcomes of bladder neck sparing during robot-assisted laparoscopic radical prostatectomy. J Urol. 2012; 188:1754-1760.
15. Brunocilla E, Schiavina R, Borghesi M, Pultrone C, Vagnoni V, Rossi MS, Cevenini M, Bianchi L, Molinaroli E, Gentile G, Martorana G. Preservation of the internal vesical sphincter and proximal urethra during retropubic radical prostatectomy may improve earlier recovery of continence in selected patients. ACTAS UROL ESP. 2014; 38:421-428.
16. Golabek T, Jaskulski J, Jarecki P, Dudek P, Szopinski T, Chlosta P. Laparoscopic radical prostatectomy with bladder neck preservation: positive surgical margin and urinary continence status. WideochirInne Tech Maloinwazyjne. 2014; 9:362-370.
17. Wei JT, Dunn RL, Marcovich R, Montie JE, Sanda MG. Prospective assessment of patient reported urinary continence after radical prostatectomy. J Urol. 2000; 164:744-748.
18. Srougi M, Nesrallah LJ, Kauffmann JR, Nesrallah A, Leite KR. Urinary continence and pathological outcome after bladder neck preservation during radical retropubic prostatectomy: a randomized prospective trial. J Urol. 2001; 165:815-818.
19. Poon M, Ruckle H, Bamshad BR, Tsai C, Webster R, Lui P. Radical retropubic prostatectomy: bladder neck preservation versus reconstruction. J Urol. 2000; 163:194-198.
20. Catalona WJ, Smith DS, Ratliff TL, Basler JW. Detection of organ-confined prostate cancer is increased through prostate-specific antigen-based screening. JAMA. 1993; 270:948-954.
21. Stamey TA, Villers AA, McNeal JE, Link PC, Freiha FS. Positive surgical margins at radical prostatectomy: importance of the apical dissection. J Urol. 1990; 143:1166-1173.
22. Zakri RH, Vedanayagam M, John B, Hearnden B, Simpson P, Eddy B. Bladder neck sparing (BNS) robot assisted laparoscopic prostatectomy (RALP): Does it improve continence? Eur Urol, Suppl. 2016; 15:eV20.
23. Nyarangi-Dix JN, Radtke JP, Hadaschik B, Pahernik S, Hohenfellner M. Impact of complete bladder neck preservation on urinary continence, quality of life and surgical margins after radical prostatectomy: a randomized, controlled, single blind trial. J Urol. 2013; 189:891-898.
24. Deliveliotis C, Protogerou V, Alargof E, Varkarakis J. Radical prostatectomy: bladder neck preservation and puboprostatic ligament sparing – effects on continence and positive margins. Urology. 2002; 60:855-858.
25. Freire MP, Weinberg AC, Lei Y, Soukup JR, Lipsitz SR, Prasad SM, Korkes F, Lin T, Hu JC. Anatomic bladder neck preservation during robotic-assisted laparoscopic radical prostatectomy: description of technique and outcomes. Eur Urol. 2009; 56:972-980.
26. Izadpanahi MH, Honarmand R, Khorrami MH, Najarzadegan MR, Sichani MM, Alizadeh F. A comparison of bladder neck preservation and bladder neck reconstruction for urinary incontinence after radical retro pubic prostatectomy. J RES MED SCI. 2014; 19:1140-1144.
27. Lowe BA. Comparison of bladder neck preservation to bladder neck resection in maintaining postrostatectomy urinary continence. Urology. 1996; 48:889-893.
28. Noh C, Kshirsagar A, Mohler JL. Outcomes after radical retropubic prostatectomy. Urology. 2003; 61:412-416.
29. You YC, Kim TH, Sung GT. Effect of Bladder Neck Preservation and Posterior Urethral Reconstruction during Robot-Assisted Laparoscopic Radical Prostatectomy for Urinary Continence. Korean J Urol. 2012; 53:29-33.
30. Li GH, Zhu SB, Cheng S, Wang Q, Yu SC, Ge GJ, Chen BD, Yu DM, Zhang ZG. Effect of bladder neck preservation on urinary continence in endoscopic extraperitoneal radical prostatectomy. Chinese Journal of Urology. 2013; 34:361-365.
31. Lou JY, Jin BZ, Liu F, Zhang YL, Zhang Q, Zhang DH. Urinary continence in laparoscopic radical prostatectomy with bladder neck preservation. Journal of Zhejiang University (Medical Sciences). 2013; 42:680-684.
32. Razi A, Yahyazadeh SR, Sedighi GM, Kazemeyni SM. Bladder neck preservation during radical retropubic prostatectomy and postoperative urinary continence. Urol J. 2009; 6:23-26.
33. Stolzenburg JU, Kallidonis P, Hicks J, Do M, Dietel A, Sakellaropoulos G, Al-Aown A, Liatsikos E. Effect of bladder neck preservation during endoscopic extraperitoneal radical prostatectomy on urinary continence. Urol Int. 2010; 85:135-138.
34. Koraitim MM. The male urethral sphincter complex revisited: an anatomical concept and its physiological correlate. J Urol. 2008; 179:1683-1689.
35. Dorschner W, Stolzenburg JU, Dieterich F. A new theory of micturition and urinary continence based on histomorphological studies. 2. The musculus sphincter vesicae: continence or sexual function? Urol Int. 1994; 52:154-158.
36. Dorschner W, Stolzenburg JU, Neuhaus J. Structure and function of the bladder neck. AdvAnatEmbryol Cell Biol. 2001; 159:1-109.
37. Chao R, Mayo ME. Incontinence after radical prostatectomy: detrusor or sphincter causes. J Urol. 1995; 154:16-18.
38. Groutz A, Blaivas JG, Chaikin DC, Weiss JP, Verhaaren M. The pathophysiology of post-radical prostatectomy incontinence: a clinical and video urodynamic study. J Urol. 2000; 163:1767-1770.
39. Myers RP. Practical surgical anatomy for radical prostatectomy. Urol Clin North Am. 2001; 28:473-490.
40. Asimakopoulos AD, Mugnier C, Hoepffner JL, Piechaud T, Gaston R. Bladder neck preservation during minimally invasive radical prostatectomy: a standardised technique using a lateral approach. BJU Int. 2012; 110:1566-1571.
41. Ren J, Wang X, Liu NB, Geng L. Effects of bladder neck preservation and reconstruction of rhabdosphincter on urinary continence recovery after laparoscopic radical prostatectomy. National Medical Journal of China. 2014; 94:1045-1047.
42. Bragayrac LN, Darwiche F, Altartir T, Kauffman E. Technique and outcomes of maximal urinary muscle preservation during robotic assisted radical prostatectomy. J Urol. 2016; 195:e518.
43. Connolly JA, Presti JJ, Carroll PR. Anterior bladder neck tube reconstruction at radical prostatectomy preserves functional urethral length – a comparative urodynamic study. Br J Urol. 1995; 75:766-770.
44. Sakai I, Harada K, Hara I, Eto H, Miyake H. Intussusception of the bladder neck does not promote early restoration to urinary continence after non-nerve-sparing radical retropubic prostatectomy. Int J Urol. 2005; 12:275-279.
45. Centemero A, Rigatti L, Giraudo D, Lazzeri M, Lughezzani G, Zugna D, Montorsi F, Rigatti P, Guazzoni G. Preoperative pelvic floor muscle exercise for early continence after radical prostatectomy: a randomised controlled study. Eur Urol. 2010; 57:1039-1043.
46. Reeves F, Preece P, Kapoor J, Everaerts W, Murphy DG, Corcoran NM, Costello AJ. Preservation of the neurovascular bundles is associated with improved time to continence after radical prostatectomy but not long-term continence rates: results of a systematic review and meta-analysis. EUR UROL. 2015; 68:692-704.
47. Smolski M, Esler RC, Turo R, Collins GN, Oakley N, Brough R. Bladder neck sparing in radical prostatectomy. Indian J Urol. 2013; 29:338-344.
48. Teber D, Sofikerim M, Ates M, Gozen AS, Guven O, Sanli O, Rassweiler J. Is type 2 diabetes mellitus a predictive factor for incontinence after laparoscopic radical prostatectomy? A matched pair and multivariate analysis. J Urol. 2010; 183:1087-1091.
49. Paparel P, Akin O, Sandhu JS, Otero JR, Serio AM, Scardino PT, Hricak H, Guillonneau B. Recovery of urinary continence after radical prostatectomy: association with urethral length and urethral fibrosis measured by preoperative and postoperative endorectal magnetic resonance imaging. Eur Urol. 2009; 55:629-637.
50. Stolzenburg JU, Schwalenberg T, Horn LC, Neuhaus J, Constantinides C, Liatsikos EN. Anatomical landmarks of radical prostatecomy. Eur Urol. 2007; 51:629-639.
51. Smith JJ, Herrell SD. Robotic-assisted laparoscopic prostatectomy: do minimally invasive approaches offer significant advantages? J Clin Oncol. 2005; 23:8170-8175.
52. Pettus JA, Masterson T, Sokol A, Cronin AM, Savage C, Sandhu JS, Mulhall JP, Scardino PT, Rabbani F. Prostate size is associated with surgical difficulty but not functional outcome at 1 year after radical prostatectomy. J Urol. 2009; 182:949-955.
53. Jenkins LC, Nogueira M, Wilding GE, Tan W, Kim HL, Mohler JL, Guru KA. Median lobe in robot-assisted radical prostatectomy: evaluation and management. Urology. 2008; 71:810-813.
54. Gomez CA, Soloway MS, Civantos F, Hachiya T. Bladder neck preservation and its impact on positive surgical margins during radical prostatectomy. Urology. 1993; 42:689-694.
55. Bianco FJ, Grignon DJ, Sakr WA, Shekarriz B, Upadhyay J, Dornelles E, Pontes JE. Radical prostatectomy with bladder neck preservation: impact of a positive margin. Eur Urol. 2003; 43:461-466.
56. Gawlas W, Golabek T, Hessel T, Szmer J, Curylo L, Chlosta P. Bladder neck preservation and the risk of positive surgical margins after laparoscopic radical prostatectomy. Eur Urol, Suppl. 2014; 13:e1275.
57. Clarke M, Horton R. Bringing it all together: Lancet-Cochrane collaborate on systematic reviews. Lancet. 2001; 357:1728.
58. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005; 5:13.