
Introduction
Since its clinical debut in 1987 for a patient undergoing cholecystectomy, laparoscopic arm has emerged as a catalyst of surgical renovation during the past three decades, which rapidly spreads its application to the entire abdominal operations [1]. Traditional two-dimensional (2D) laparoscopy features higher definition of graphic display and more visional comforts, as well as lower threshold expenditure. Nevertheless, lacking of stereoscopic perception not only leads to elongated learning curves among surgical novices, but also endangers the estimate of surgical depth during critical operations, especially the current trend for laparoscopy is moving towards deeper and riskier surgical regions such as radical pancreatectomy and prostatectomy [2]. Therefore, a three-dimensional (3D) view with better stereoscopic demonstration is urgently needed.
In 1993, Wenzl et al [3] firstly implemented a gynecological operation under a laparoscopic 3D instrument. However, the initial 3D display was mainly based on Shutter Glass (SG) technique, which provided poor-definition images and was harmful to surgeons’ eyes. Owing to the manufactural improvements in optic industry, 3D laparoscope characterized by Film-type Patterned Retarder (FPR) was subsequently invented. This new generation of 3D laparoscopic facility features high-definition and stable image, alleviating the visional burdens of surgical operators and truly bringing laparoscopic operations into a tridimensional era. Therefore, Buchs et al [4] firstly reported a smooth operation by FPR glasses in 2012, and from then on, 3D laparoscopy began globally popularized among surgeon communities including China [5].
Unfortunately, the comparative efficacy of 3D laparoscopy against 2D laparoscopy remains undetermined, due to the scarcity of clinical evidences especially a systematic summary of surgical indicators. Hence based on current literatures, we performed this systematic review and meta-analysis in order to explore the comparative efficacy of 3D laparoscopy in abdominal operations.
Results
General characteristics
Among 3126 retrieved records, 21 studies were included into the quantitative analysis (Figure 1). 12 investigations were written in English while the remaining was published in Chinese (n = 9). China was the chief source region of eligible trials (n = 10), followed by Italy (n = 5) and Turkey (n = 3). A total of 13 studies were retrospectively conducted, while 8 trials were randomly designed. The most frequent surgical type was cholecystectomy (n = 4) and prostatectomy (n = 4). The total amount of sample-size was 1520 (two-dimensional: 819; three-dimensional: 701), individually ranging from 22 to 154. According to the statistical analysis of demographic parameters (age, sex ratio), included studies were confirmed to be internally comparable (P > 0.05) (Table 1).
Table1: Demographic characteristics of included studies
Study |
Country |
Trial type |
Surgical type |
Group |
Sample-size |
Age (Y) |
Sex (M/F) |
Agrusa 2015 [6] |
Italy |
Retrospective |
Adrenalectomy |
2D |
26 |
54.3±9.0 |
17/9 |
3D |
13 |
55.8±7.5 |
8/5 |
||||
Aykan 2014 [7] |
Turkey |
Retrospective |
Prostatectomy |
2D |
66 |
64.5±8.0 |
66/0 |
3D |
29 |
65.0±6.0 |
29/0 |
||||
Bilgen 2013 [8] |
Turkey |
Randomized |
Cholecystectomy |
2D |
11 |
53.0 |
1/10 |
3D |
11 |
54.0 |
0/11 |
||||
Bove 2015 [9] |
Italy |
Retrospective |
Prostatectomy |
2D |
43 |
60.1 |
43/0 |
3D |
43 |
63.9 |
43/0 |
||||
Chen 2014 [10] |
China |
Retrospective |
Gastrectomy |
2D |
40 |
51.0±5.2 |
30/10 |
3D |
40 |
49.0±4.8 |
27/13 |
||||
Chen 2015 [11] |
China |
Retrospective |
Thyroidectomy |
2D |
34 |
49.2±11.6 |
6/28 |
3D |
26 |
46.2±11.7 |
6/20 |
||||
Chen 2016 [12] |
China |
Randomized |
Ureterotomy |
2D |
20 |
45.8±12.3 |
10/10 |
3D |
25 |
41.6±13.2 |
14/11 |
||||
Curro 2015-1 [13] |
Italy |
Randomized |
Gastric bypass |
2D |
20 |
38.0±8.8 |
4/16 |
3D |
20 |
39.0±9.5 |
4/16 |
||||
Curro 2015-2 [13] |
Italy |
Randomized |
Sleeve gastrectomy |
2D |
20 |
36.0±8.3 |
3/17 |
3D |
20 |
36.0±9.8 |
4/16 |
||||
Curro 2016 [14] |
Italy |
Retrospective |
Colectomy |
2D |
25 |
68.0±8.0 |
14/11 |
3D |
25 |
69.0±9.5 |
12/13 |
||||
Hanna 1998 [15] |
UK |
Randomized |
Cholecystectomy |
2D |
30 |
52.0±15.0 |
8/22 |
3D |
30 |
58.0±11.8 |
7/23 |
||||
Hou 2015 [16] |
China |
Randomized |
Esophagectomy |
2D |
76 |
55.1±7.6 |
44/32 |
3D |
78 |
55.7±6.3 |
41/37 |
||||
Ji 2014 [17] |
China |
Retrospective |
Rectectomy |
2D |
20 |
59.0±8.0 |
15/5 |
3D |
16 |
55.0±8.0 |
9/7 |
||||
Kinoshita 2015 [18] |
Japan |
Randomized |
Prostatectomy |
2D |
57 |
65.9±4.7 |
57/0 |
3D |
59 |
66.5±4.5 |
59/0 |
||||
Navarra 2015 [19] |
Italy |
Randomized |
Cholecystectomy |
2D |
35 |
50.0±10.5 |
9/26 |
3D |
35 |
56.0±9.8 |
7/28 |
||||
Ruan 2015 [20] |
China |
Randomized |
Nephrectomy |
2D |
45 |
58.7±3.2 |
22/23 |
3D |
45 |
60.4±2.7 |
24/21 |
||||
Usta 2014 [21] |
Turkey |
Retrospective |
Hysterectomy |
2D |
91 |
52.2 |
0/91 |
3D |
56 |
49.5 |
0/56 |
||||
Velayutham 2016 [22] |
France |
Retrospective |
Hepatectomy |
2D |
40 |
NA |
24/16 |
3D |
20 |
NA |
9/11 |
||||
Xu 2014 [23] |
China |
Retrospective |
Pyeloplasty |
2D |
15 |
31.0±6.0 |
7/8 |
3D |
16 |
30.0±6.0 |
9/7 |
||||
Xu 2015 [24] |
China |
Retrospective |
Prostatectomy |
2D |
32 |
67.8±8.4 |
32/0 |
3D |
18 |
67.3±6.6 |
18/0 |
||||
Zeng 2016 [25] |
China |
Retrospective |
Cholecystectomy |
2D |
43 |
57.0±12.0 |
28/15 |
3D |
46 |
59.0±11.0 |
28/18 |
||||
Zou 2014 [26] |
China |
Retrospective |
Thyroidectomy |
2D |
30 |
44.4±7.6 |
12/18 |
3D |
30 |
43.3±7.8 |
10/20 |
Y: years; M/F: male/female; NA: not available; 2D: two-dimensional; 3D: three-dimensional;
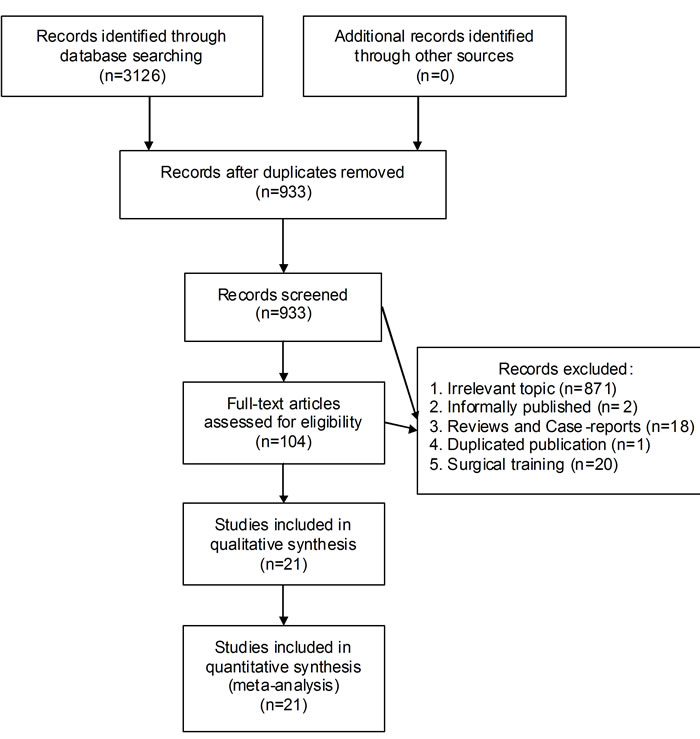
Figure 1: Selection flow chart of our meta-analysis.
Methodological quality
By Newcastle-Ottawa Scale, all retrospective studies were confirmed as high-quality trials in methodology (NOS>6) (Table 2). Moreover, by Revised Jadad’s Scale, the majority of randomized trials were methodologically rigorous, except for Bilgen 2013 and Ruan 2015 (lower than 4 points) (Table 3).
Table 2: Methodological assessment by Newcastle-Ottawa Scale
Study |
Selection |
Comparability |
Outcome |
Total |
Agrusa 2015 |
3 |
2 |
2 |
7 |
Aykan 2014 |
3 |
2 |
2 |
7 |
Bove 2015 |
3 |
2 |
3 |
8 |
Chen 2014 |
3 |
2 |
1 |
6 |
Chen 2015 |
3 |
2 |
1 |
6 |
Curro 2016 |
3 |
2 |
1 |
6 |
Ji 2014 |
3 |
2 |
2 |
7 |
Usta 2014 |
3 |
2 |
2 |
7 |
Velayutham 2016 |
3 |
2 |
2 |
7 |
Xu 2014 |
3 |
2 |
3 |
8 |
Xu 2015 |
3 |
2 |
1 |
6 |
Zeng 2016 |
3 |
2 |
1 |
6 |
Zou 2014 |
3 |
2 |
1 |
6 |
Table 3: Methodological assessment by Revised Jadad’s Scale
Study |
Randomization |
Allocation concealment |
Blindness |
Withdrawal |
Total |
Bilgen 2013 |
2 |
1 |
0 |
0 |
3 |
Chen 2016 |
2 |
1 |
0 |
1 |
4 |
Curro 2015 |
2 |
2 |
0 |
1 |
5 |
Hanna 1998 |
2 |
2 |
0 |
1 |
5 |
Hou 2015 |
2 |
1 |
0 |
1 |
4 |
Kinoshita 2015 |
2 |
2 |
0 |
1 |
5 |
Navarra 2015 |
2 |
2 |
0 |
0 |
4 |
Ruan 2015 |
1 |
1 |
0 |
1 |
3 |
Primary endpoint-surgical time
Overall
The surgical duration by 3D laparoscopy was much lower than that of 2D technique (P < 0.00001) (Figure 2).
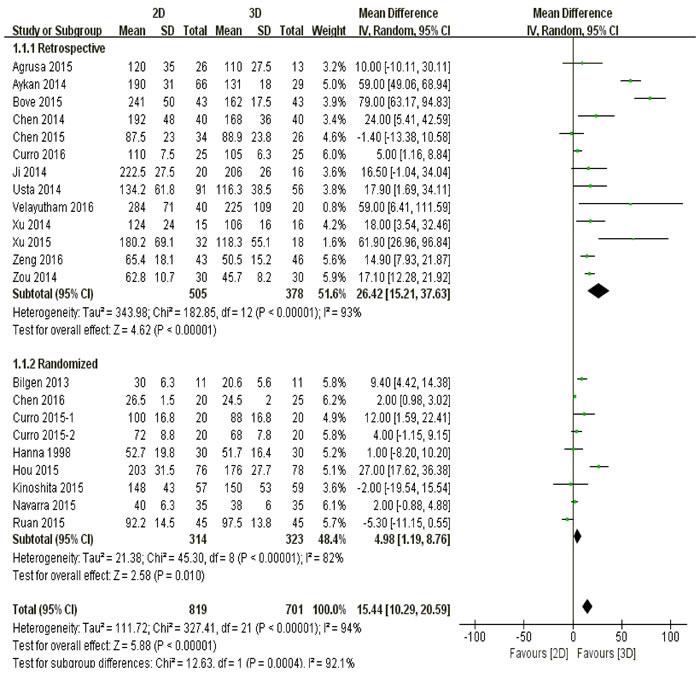
Figure 2: The comparison of surgical time according to different study types.
Study type
No matter the studies were retrospectively (P < 0.00001) or randomly designed (P < 0.01), three-dimensional laparoscopy spent significantly less surgical time than two-dimensional did (Figure 2).
Surgical type
Patients undergoing cholecystectomy (P = 0.03), prostatectomy (P = 0.005) and digestive operations (P = 0.0004) endured less surgical time by three-dimensional laparoscopy than those by two-dimensional device. On the other hand, there was no significant difference between 3D and 2D laparoscopy in terms of urological operations (P = 0.44) and other types (P = 0.07) (Figure 3).
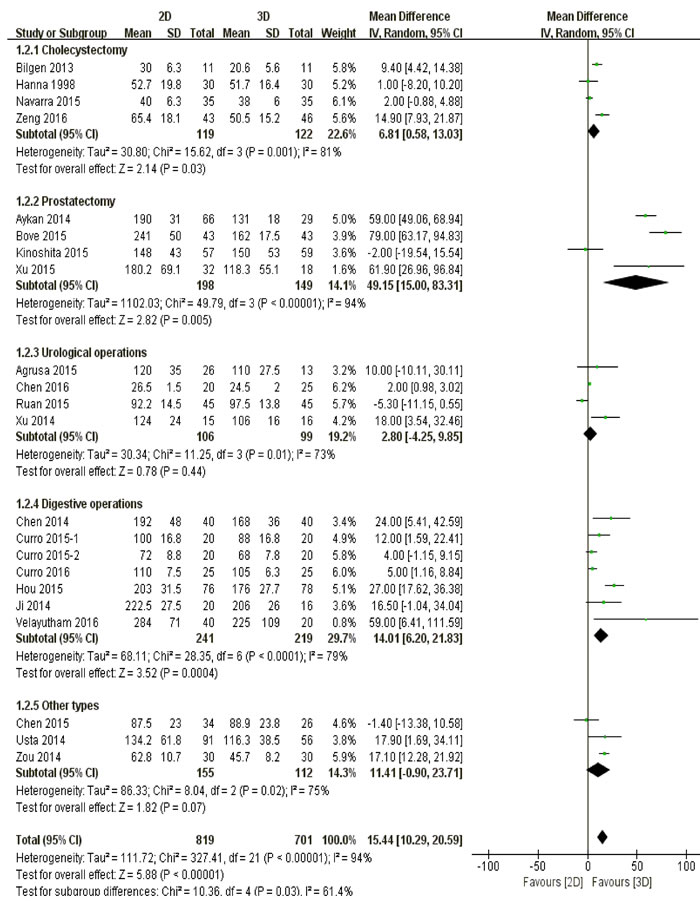
Figure 3: The comparison of surgical time according to different surgical types.
Primary endpoint-blood loss
Overall
Lower volume of intraoperative blood loss was observed among 3D group than that of 2D group (P = 0.01) (Figure 4).
Study type
It was retrospectively confirmed that 3D laparoscopy led to less blood loss against 2D laparoscopy (P = 0.0004), while randomized investigations summarized that patients undergoing both techniques had comparable volume of blood loss during operations (P = 0.38) (Figure 4).
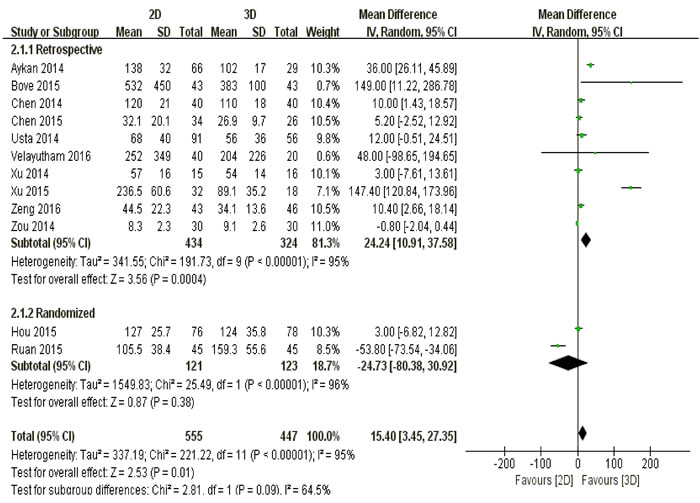
Figure 4: The comparison of blood loss according to different study types.
Surgical type
Patients undergoing cholecystectomy (P = 0.008), prostatectomy (P = 0.03) and digestive operations (P = 0.03) suffered less intraoperative blood loss by 3D laparoscopic arm. However, both techniques resulted in similar magnitude of blood loss amid patients with urological (P = 0.38) or other types of diseases (P = 0.32) (Figure 5).
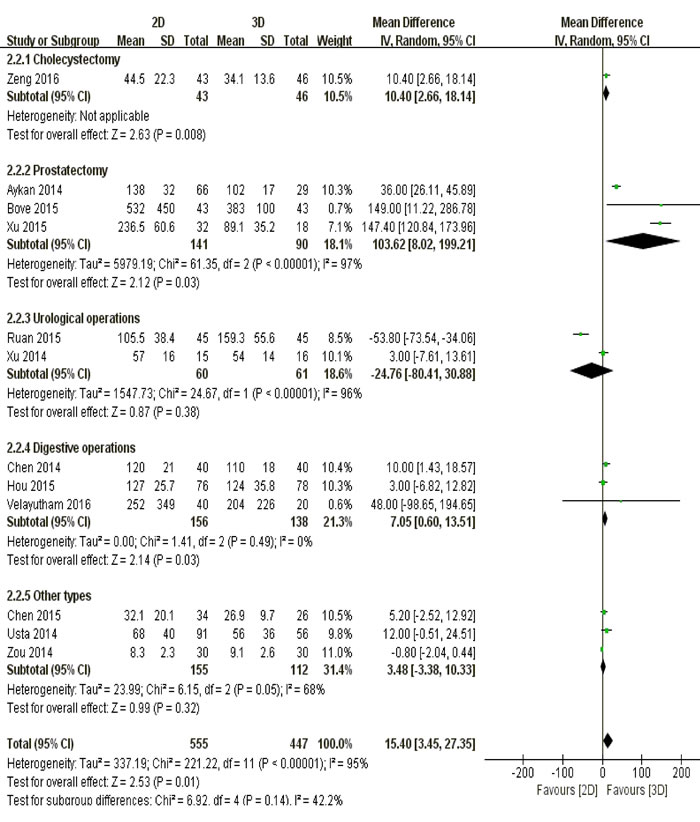
Figure 5: The comparison of blood loss according to different surgical types.
Primary endpoint-perioperative complications
Overall
Patients had lower incidence of perioperative complications following 3D management than those of 2D group (P = 0.04) (Supplementary Figure S1).
Study type
In terms of perioperative complications, there was no significant difference between 3D and 2D laparoscopy, regardless of retrospective (P = 0.07) or randomized studies (P = 0.29) (Supplementary Figure S1).
Surgical type
Comparable incidence of perioperative complications was observed between 3D and 2D laparoscopy, whichever of cholecystectomy (P = 0.93), prostatectomy (P = 0.05), urological operations (P = 0.18), digestive operations (P = 0.87) or other types (P = 0.37) (Supplementary Figure S2).
Primary endpoint-hospital stay
Overall
Patients receiving 3D laparoscopic management experienced shorter period of hospital stay than those with two-dimensional intervention (P = 0.03) (Supplementary Figure S3).
Study type
The pooled analysis of retrospective studies suggested that 3D laparoscopy was more effective in reducing hospital stay than 2D laparoscopy was (P = 0.04). However, evidence from randomized trials revealed a similar hospital stay among patients undergoing both interventions (P = 0.58) (Supplementary Figure S3).
Surgical type
Patients between 3D and 2D group had similar length of hospital stay, including those undergoing cholecystectomy (P = 0.58), urological operations (P = 0.39), digestive operations (P = 0.90) and other types of operations (P = 0.05). Nevertheless, 3D laparoscopic prostatectomy resulted in shorter hospital stay against 2D technique (P = 0.04) (Supplementary Figure S4).
Primary endpoint-conversion rate
Overall
The conversion rate between three-dimensional and two-dimensional laparoscopy was statistically equivalent (P = 0.68) (Supplementary Figure S5).
Study type
The pooled outcome of retrospective trials revealed that both 3D and 2D interventions resulted in similar conversion rate (P = 0.68). Data of randomized studies was not estimable (Supplementary Figure S5).
Surgical type
Both 3D and 2D techniques led to similar conversion rate among patients undergoing cholecystectomy (P = 0.63), digestive operations (P = 0.62) and other types of operations (P = 0.60). Data of prostatectomy and urological operations was not estimable (Supplementary Figure S6).
Secondary endpoints
Drainage volume
The drainage volume of surgical patients was quantitatively identical between three-dimensional and two-dimensional group (P = 0.74) (Supplementary Figure S7).
Drainage time
There was no significant difference of drainage time between 3D and 2D techniques (P = 0.26) (Supplementary Figure S8).
Numbers of retrieved lymph nodes
Comparable amount of lymph nodes was retrieved irrespective of tridimensional and two-dimensional laparoscopy (P = 0.85) (Supplementary Figure S9).
Hospital expenses
The average hospital expenses between 2D and 3D laparoscopy were statistically equivalent (P = 0.49) (Supplementary Figure S10).
Anastomosis time in prostatectomy
The pooled result suggested that there was no significant difference of anastomosis time between 2D and 3D interventions (P = 0.15) (Supplementary Figure S11).
6-month continence rate
Patients had similar 6-month continence rate regardless of 2D or 3D laparoscopy (P = 0.61) (Supplementary Figure S12).
Sensitivity analysis
Firstly, the sensitivity analysis was performed by excluding low-quality trials. Despite Bilgen 2013 and Ruan 2015 were eliminated from primary endpoint analysis, the majority of pooled outcomes remained stable, except for perioperative complications (P value changing from 0.04 to 0.06).
Secondly, by interchanging fixed-effects and random-effects models, the pooled results of primary endpoints were confirmed to be stable, except for blood loss (P value changing from 0.01 to 0.29)
Thirdly, by randomly excluding one trial from pooled analysis in STATA 12.0, the outcome of surgical time was verified to be stable (Supplementary Figure S13).
Publication bias
We took surgical time as an exemplary indicator for publication bias assessment. P values of Begg’s test (Supplementary Figure S14) and Egger’s test (Supplementary Figure S15) were 0.215 and 0.003 respectively, revealing a potential existence of publication bias across included studies. Thus we additionally carried out a Trim-and-Fill method, whose result indicated that no studies were trimmed or filled and the outcome was therefore stable (Supplementary Figure S16).
Discussion
According to the pooled outcomes of primary endpoints, three-dimensional laparoscopy resulted in significantly less surgical time, blood loss, perioperative complications and hospital stay among surgical patients. It is relatively comprehensible that its overwhelming preponderance against 2D laparoscopy may mainly attribute to the more stereoscopic surgical view. A tridimensional reconstruction of target region greatly facilitates the estimate of anatomic depth and accuracy of surgical manipulation [27]. Meanwhile, despite of wearing 3D glasses, current technological improvements successfully prevent surgical operators from visual fatigue. However, in terms of conversion rate, 3D laparoscopy resulted in similar outcome compared to 2D technique. This is probably because that although two-dimensional image leads to higher risk of surgical errors, those potential mistakes are still unable to threaten the overall operative safety in most circumstances, especially among surgeons with rich experiences and advanced skills [28-30]. Therefore a traditional laparoscopy is quite enough to deal with the intraoperative accidents. Furthermore, based on different study types and surgical types, subgroup analysis had brought more specific evidences besides the overall comparisons. Due to its significant advantages on primary endpoints, 3D laparoscopy was strongly recommended for cholecystectomy and prostatectomy. It is known to all that a neat dissection of Calot’s triangle and a functional reservation of surrounding structures are crucial procedures for a successful cholecystectomy and prostatectomy respectively. A more stereoscopic visual perception greatly supports tissue separation and vessel ligation. On the other hand, regardless of 2D or 3D laparoscopy, comparable efficacy was observed among patients undergoing digestive operations or urological operations, which was theoretically abnormal and hence more convincing literatures were still needed for future supplements.
Including drainage volume, drainage time, numbers of retrieved lymph nodes, hospital expenses, anastomosis time in prostatectomy and 6-month continence rate, both techniques displayed statistical similarity on secondary endpoints. Generally, the advantage of security could directly result in better outcomes of these secondary parameters. We assume that these exceptional consequences may blame on the limited amount of included studies, which diminishes the outcome credibility.
Currently, conclusive evidences that analyze the comparative efficacy of tridimensional laparoscopy remain in scarcity. Sorensen et al [31] performed a systematic review of 3D laparoscopy versus 2D laparoscopy on simulated settings. Without examining the clinical significance, their results merely revealed a better performance on surgical tasks and trainings by tridimensional laparoscopy. Sakata et al [2] systematically summarized the technical advantages of current 3D laparoscopy, implicating the great potential of its surgical application. By far, large-scale randomized trial of this topic is still lacking and no consensus has been reached among current literatures. Hou et al [16] , a randomized study of 154 participants, concluded that both techniques achieved similar outcomes of primary endpoints. However, Bilgen et al [8] stated that three-dimensional laparoscopy was superior to two-dimensional laparoscopy in terms of cholecystectomy. These academic inconsistencies highlight the clinical significance of our meta-analysis.
Although our meta-analysis was rigorously designed and performed, there were still some limitations within. Firstly, the statistical heterogeneity could not be thoroughly eliminated despite that we had conducted considerable amount of subgroup analyses. This is probably because that there is currently lacking of operative standards of three-dimensional laparoscopy. Different norms lead to inconsistent results and varied conclusions. Besides, more potential confounding elements are also needed to be explored and considered. Secondly, the number of included studies for secondary endpoints was not adequate to make a convincing conclusion. Well-prepared investigations are always needed for the future updates and supplements.
Taken together, through our systematic review and meta-analysis, we believe that three-dimensional laparoscopy is a preferably technical option against two-dimensional laparoscopy due to its better surgical efficacy. Thus a wider clinical application of 3D laparoscopy is strongly recommended.
Materials and methods
This systematic study was classically performed as Cochrane Collaboration recommended. Each step of pooled analysis was independently conducted by two investigators, while any disagreement was settled by mutual discussion.
Literature retrieval
Databases of PubMed, Web of Science, EMBASE and Cochrane Library were carefully screened using search term of “three dimensional laparoscopic”. Abstracts, full-texts and reference lists were thoroughly examined to avoid unnecessary omission during retrieval process.
Selection criteria
Inclusion criteria: 1. Formally published studies until February 2016; 2.Comparing the clinical efficacy between 3D and 2D laparoscopy; 3. Adequate and accessible data of target endpoints;
Exclusion criteria: 1. Overlapped or duplicated publications; 2. Insufficient scale of sample-size ( < 10); 3. Inappropriate article types such as Reviews and Case reports;
Data extraction
A standardized form was designed to facilitate the extraction process. Original data of demographic elements (Study name; Country; Trial type; Surgical type; Group; Sample-size; Age; Sex), primary endpoints (Surgical time; Blood loss; Perioperative complications; Hospital stay; Conversion rate) and secondary endpoints (Drainage volume; Drainage time; Numbers of retrieved lymph nodes; Hospital expenses; Anastomosis time in prostatectomy; 6-month continence rate) were retrieved from tables, main text, figures and supplementary information among included studies. Continuous variables were rounded to one decimal place.
Methodological quality appraisal
Observational investigations were assessed by Newcastle-Ottawa Scale (NOS). The entire scale was constituted by three categories including selection, comparability and outcome, with a maximum score of nine. Studies graded with six or more scores were identified as high-quality in methodology.
A Revised Jadad’s Scale was employed to evaluate randomized trials. Randomization, allocation concealment, blindness and withdrawal were four scoring items, with a full credit of seven. Studies rated with four marks or more were recognized as high-quality in methodology.
Statistical analysis
Review Manager 5.3 served as a statistical platform. Dichotomous and continuous variables were respectively analyzed by odds ratio (OR) and weighted mean difference (WMD). If the original data were inappropriately provided, median was taken for mean while standard deviation was estimated from range, interquartile range or 95% confidence interval, according to the instructions from Cochrane Handbook. Statistical heterogeneity was denoted by the degree of inconsistency (I2). Fixed-effects model was preferred when I2 value was less than 25%, otherwise a random-effects model was chosen. Primary endpoints were additionally divided into multiple subgroups based on different study types and surgical types. Sensitivity analysis was conducted by removing low-quality studies and interchanging calculation models (fixed-effects and random-effects), in order to observe the outcome stability. Publication bias was analyzed by Begg’s test, Egger’s test and Trim-and-Fill method. Statistical significance was indicated by P < 0.05.
Acknowledgments
We sincerely appreciate our team members for providing statistical instructions.
Conflicts of interest
We declare that there is no conflict of interest among all listed authors.
Grant support
This study was financially supported by Research Fund of Public Welfare in Health Industry, Health and Family Plan Committee of China (No.201402015). The recipient was Guobin Wang.
References
1. Polychronidis A, Laftsidis P, Bounovas A and Simopoulos C. Twenty years of laparoscopic cholecystectomy: Philippe Mouret—March 17, 1987. JSLS. 2008; 12:109-111.
2. Sakata S, Watson MO, Grove PM and Stevenson AR. The Conflicting Evidence of Three-dimensional Displays in Laparoscopy: A Review of Systems Old and New. ANN SURG. 2016; 263:234-239.
3. Wenzl R, Pateisky N and Husslein P. [First use of a 3D video-endoscope in gynecology]. Geburtshilfe Frauenheilkd. 1993; 53:776-778.
4. Buchs NC, Volonte F, Pugin F, Toso C and Morel P. Three-dimensional laparoscopy: a step toward advanced surgical navigation. SURG ENDOSC. 2013; 27:692-693.
5. McLachlan G. From 2D to 3D: the future of surgery? LANCET. 2011; 378:1368.
6. Agrusa A, di Buono G, Chianetta D, Sorce V, Citarrella R, Galia M, Vernuccio L, Romano G and Gulotta G. Three-dimensional (3D) versus two-dimensional (2D) laparoscopic adrenalectomy: A case-control study. Int J Surg. 2016; 28 Suppl 1:S114-7.
7. Aykan S, Singhal P, Nguyen DP, Yigit A, Tuken M, Yakut E, Colakerol A, Sulejman S and Semercioz A. Perioperative, pathologic, and early continence outcomes comparing three-dimensional and two-dimensional display systems for laparoscopic radical prostatectomy—a retrospective, single-surgeon study. J ENDOUROL. 2014; 28:539-543.
8. Bilgen K, Ustun M, Karakahya M, Isik S, Sengul S, Cetinkunar S and Kucukpinar TH. Comparison of 3D imaging and 2D imaging for performance time of laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2013; 23:180-183.
9. Bove P, Iacovelli V, Celestino F, De Carlo F, Vespasiani G and Finazzi AE. 3D vs 2D laparoscopic radical prostatectomy in organ-confined prostate cancer: comparison of operative data and pentafecta rates: a single cohort study. BMC UROL. 2015; 15:12.
10. Chen H, Yu J, Huang Z and Lin X. [Application of three-dimensional high-definition laparoscope in laparoscopic radical resection of gastric cancer]. Nan Fang Yi Ke Da Xue Xue Bao. 2014; 34:588-590.
11. Chen J, Zheng H, Jiang L, Deng W, Li Q, Liu X, Fan D and He J. [Comparison the application of 3D versus 2D laparoscopic thyroidectomy via modified chest and mammary areola approach]. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015; 29:1006-1008.
12. Chen Q, Liu J, Xian Z, Xu Z, Luo Y, Chen H and Ye C. [Comparison of the effect of three-dimensional versus two-dimensional retroperitoneal laparoscopic ureter lithotomy]. Nan Fang Yi Ke Da Xue Xue Bao. 2016; 36:148-150.
13. Curro G, La Malfa G, Caizzone A, Rampulla V and Navarra G. Three-Dimensional (3D) Versus Two-Dimensional (2D) Laparoscopic Bariatric Surgery: a Single-Surgeon Prospective Randomized Comparative Study. OBES SURG. 2015; 25:2120-2124.
14. Curro G, Cogliandolo A, Bartolotta M and Navarra G. Three-Dimensional Versus Two-Dimensional Laparoscopic Right Hemicolectomy. J Laparoendosc Adv Surg Tech A. 2016; 26:213-217.
15. Hanna GB, Shimi SM and Cuschieri A. Randomised study of influence of two-dimensional versus three-dimensional imaging on performance of laparoscopic cholecystectomy. LANCET. 1998; 351:248-251.
16. Hou Y, Guo W, Yang Z and Zhao J. [Comparative study of 3D thoracoscopic esophagectomy versus 2D thoracoscopic esophagectomy for esophageal carcinoma]. Zhonghua Wei Chang Wai Ke Za Zhi. 2015; 18:889-892.
17. Ji F, Liu X, Liu Z and Fang X. [Application of three-dimensional laparoscopic system in obturator lymph node dissection of progressive rectal cancer]. Zhonghua Wei Chang Wai Ke Za Zhi. 2014; 17:1121-1124.
18. Kinoshita H, Nakagawa K, Usui Y, Iwamura M, Ito A, Miyajima A, Hoshi A, Arai Y, Baba S and Matsuda T. High-definition resolution three-dimensional imaging systems in laparoscopic radical prostatectomy: randomized comparative study with high-definition resolution two-dimensional systems. SURG ENDOSC. 2015; 29:2203-2209.
19. Curro G, La Malfa G, Lazzara S, Caizzone A, Fortugno A and Navarra G. Three-Dimensional Versus Two-Dimensional Laparoscopic Cholecystectomy: Is Surgeon Experience Relevant? J Laparoendosc Adv Surg Tech A. 2015; 25:566-570.
20. Ruan Y, Wang XH, Wang K, Zhao YY, Xia SJ and Xu DL. Clinical evaluation and technical features of three-dimensional laparoscopic partial nephrectomy with selective segmental artery clamping. WORLD J UROL. 2015.
21. Usta TA, Karacan T, Naki MM, Calik A, Turkgeldi L and Kasimogullari V. Comparison of 3-dimensional versus 2-dimensional laparoscopic vision system in total laparoscopic hysterectomy: a retrospective study. ARCH GYNECOL OBSTET. 2014; 290:705-709.
22. Velayutham V, Fuks D, Nomi T, Kawaguchi Y and Gayet B. 3D visualization reduces operating time when compared to high-definition 2D in laparoscopic liver resection: a case-matched study. SURG ENDOSC. 2016; 30:147-153.
23. Xu W, Li H, Ji Z, Zhang X, Zhang Y, Xiao H and Liu G. [Comparison of three dimensional and two dimentional laparoscopic pyeloplasty for ureteropelvic junction obstruction]. Zhonghua Wai Ke Za Zhi. 2014; 52:771-774.
24. Xu B, Liu N, Jiang H, Chen SQ, Yang Y, Zhang XW, Sun C, Zhang LJ, Liu J, Sha GZ, Zhu WD and Chen M. [3D versus 2D laparoscopic radical prostatectomy for the treatment of prostate cancer]. Zhonghua Nan Ke Xue. 2015; 21:904-907.
25. Zeng N, Fang C, Yang J, Xiang N, Zhu W, Liu J, Chen Q, Liang H and Huang W. [Application of three-dimensional laparoscopic cholecystectomy for complicated gallstone disease]. Nan Fang Yi Ke Da Xue Xue Bao. 2016; 36:145-147.
26. Zou Z, Huang Z, Li Q, Chen F, Zhao D and Wang M. [A comparative study of three-dimensional versus two-dimensional laparoscopic subtotal thyroidectomy via a breast approach]. Nan Fang Yi Ke Da Xue Xue Bao. 2014; 34:1233-1234.
27. Zhao D, Huang Z and Zou Z. [Research progress of three-dimensional laparoscope system]. Nan Fang Yi Ke Da Xue Xue Bao. 2014; 34:594-596, 1-596.
28. Shah J, Buckley D, Frisby J and Darzi A. Depth cue reliance in surgeons and medical students. SURG ENDOSC. 2003; 17:1472-1474.
29. Brigner WL, Deni JR and Hildreth LL. Simultaneous changes in length and direction as a cue for perceived depth. Percept Mot Skills. 1994; 78:1385-1386.
30. Mather G and Smith DR. Depth cue integration: stereopsis and image blur. VISION RES. 2000; 40:3501-3506.
31. Sorensen SM, Savran MM, Konge L and Bjerrum F. Three-dimensional versus two-dimensional vision in laparoscopy: a systematic review. SURG ENDOSC. 2016; 30:11-23.