
INTRODUCTION
Anal canal carcinomas (ACCs) are rare, representing 2% of all digestive cancers and 6% of the ano-rectal cancers, but their incidence is increasing [1]. Since the publication of Randomized Controled Trials (RCTs), External Beam Radiotherapy (RT) +/- concomitant chemotherapy (CT) is the standard treatment for ACCs [2–4]. The role of the prophylactic inguinal irradiation (PII) is a controversial topic of debate: for N0 tumors, PII is considered effective, but it results in larger RT field sizes. Thus, it could contribute to higher risks of acute and late toxicity. A recent study by Ortholan et al., confirming the efficacy of the PII in preventing inguinal recurrences and its indication for all T3-4 tumors, concluded also that PII should be discussed for early-stage tumors, because they present a not-negligible 5-year inguinal recurrence rate of 12% when omitting PII, a rate that is substantially high considering the early stage of these cancers [5]. On the other hand, looking at the same figures, it could be easily argued that only 1/10 patients presenting an early stage ACC would really benefit of the PII, but all the patients receiving it are exposed to the potential risk of its acute and late toxicity.
Moreover, a study by Crowley et al. supports the use, for selected cases of ACC, of smaller than standard radiation fields, avoiding PII, in order to reduce acute and late toxicity [6], an attitude of particular interest in patients presenting an intrinsic higher risk of toxicity (e.g. HIV+ patients, elderly patients…) [7, 8]. Unfortunately, none of the available classical statistical techniques or predictive models allow the identification of patients presenting a higher risk of inguinal microscopic invasion (for example, higher than 5%).
Predictive models based on the Machine Learning (ML) and Artificial Intelligence (AI) techniques are being more and more adopted in the medical and bio-molecular field, as these methods have many attractive theoretic properties, specifically, the ability of analysing very large datasets and to detect non predefined relations such as nonlinear effects and/or interactions [9, 10]. Despite the growing interest of scientific community in exploring the potential of these techniques in the decision process in clinical oncology, any of these studies have never been addressed to the identification of a predictor of the patients that could more benefit of the PPI. This study was specifically addressed to the development and verification of a ML-based predictor to solve this clinical problem.
RESULTS
Participants (items 13a-13c, see Table 1 for the items of this and for the following sub-sessions)
Table 1: The TRIPOD checklist (adapted from [12])
Section/Topic |
Item |
Checklist Item |
|---|---|---|
Title and abstract |
||
Title |
1 |
Identify the study as developing and/or validating a multivariable prediction model, the target population, and the outcome to be predicted (D;V)*. |
Abstract |
2 |
Provide a summary of objectives, study design, setting, participants, sample size, predictors, outcome, statistical analysis, results, and conclusions (D;V). |
Introduction |
||
Background and objectives |
3a |
Explain the medical context (including whether diagnostic or prognostic) and rationale for developing or validating the multivariable prediction model, including references to existing models (D;V). |
3b |
Specify the objectives, including whether the study describes the development or validation of the model or both (D;V). |
|
Methods |
||
Source of data |
4a |
Describe the study design or source of data (e.g., randomized trial, cohort, or registry data), separately for the development and validation data sets, if applicable (D;V). |
4b |
Specify the key study dates, including start of accrual; end of accrual; and, if applicable, end of follow-up (D;V). |
|
Participants |
5a |
Specify key elements of the study setting (e.g., primary care, secondary care, general population) including number and location of centres (D;V). |
5b |
Describe eligibility criteria for participants (D;V). |
|
5c |
Give details of treatments received, if relevant (D;V). |
|
Outcome |
6a |
Clearly define the outcome that is predicted by the prediction model, including how and when assessed (D;V). |
6b |
Report any actions to blind assessment of the outcome to be predicted (D;V). |
|
Predictors |
7a |
Clearly define all predictors used in developing or validating the multivariable prediction model, including how and when they were measured (D;V). |
7b |
Report any actions to blind assessment of predictors for the outcome and other predictors. |
|
Sample size |
8 |
Explain how the study size was arrived at (D;V). |
Missing data |
9 |
Describe how missing data were handled (e.g., complete-case analysis, single imputation, multiple imputation) with details of any imputation method (D;V). |
Statistical analysis methods |
10a |
Describe how predictors were handled in the analyses (D). |
10b |
Specify type of model, all model-building procedures (including any predictor selection), and method for internal validation (D). |
|
10c |
For validation, describe how the predictions were calculated (V). |
|
10d |
Specify all measures used to assess model performance and, if relevant, to compare multiple models (D;V). |
|
10e |
Describe any model updating (e.g., recalibration) arising from the validation, if done (V). |
|
Risk groups |
11 |
Provide details on how risk groups were created, if done (D;V). |
Development vs. validation |
12 |
For validation, identify any differences from the development data in setting, eligibility criteria, outcome, and predictors (V). |
Results |
||
Participants |
13a |
Describe the flow of participants through the study, including the number of participants with and without the outcome and, if applicable, a summary of the follow-up time. A diagram may be helpful (D;V). |
13b |
Describe the characteristics of the participants (basic demographics, clinical features, available predictors), including the number of participants with missing data for predictors and outcome (D;V). |
|
13c |
For validation, show a comparison with the development data of the distribution of important variables (demographics, predictors and outcome) (V). |
|
Model development |
14a |
Specify the number of participants and outcome events in each analysis (D). |
14b |
If done, report the unadjusted association between each candidate predictor and outcome (D). |
|
Model specification |
15a |
Present the full prediction model to allow predictions for individuals (i.e., all regression coefficients, and model intercept or baseline survival at a given time point) (D). |
15b |
Explain how to the use the prediction model (D). |
|
Model performance |
16 |
Report performance measures (with CIs) for the prediction model (D;V). |
Model-updating |
17 |
If done, report the results from any model updating (i.e., model specification, model performance) (V). |
Discussion |
||
Limitations |
18 |
Discuss any limitations of the study (such as non representative sample, few events per predictor, missing data) (D;V). |
Interpretation |
19a |
For validation, discuss the results with reference to performance in the development data, and any other validation data (V). |
19b |
Give an overall interpretation of the results, considering objectives, limitations, results from similar studies, and other relevant evidence (D;V). |
|
Implications |
20 |
Discuss the potential clinical use of the model and implications for future research (D;V). |
Other information |
||
Supplementary information |
21 |
Provide information about the availability of supplementary resources, such as study protocol, Web calculator, and data sets (D;V). |
Funding |
22 |
Give the source of funding and the role of the funders for the present study (D;V). |
*Items relevant only to the development of a prediction model are denoted by “D”, items relating solely to a validation of a prediction model are denoted by “V”, and items relating to both are denoted “D;V”.
Nineteen patients received a Curative Inguinal Irradiation (CII), and 2/19 presented an inguinal relapse. Concerning the remaining 175 patients, 151 of them did not receive a PII and 24 received it. Finally, 13/151 patients (8.6%) and 3/24 pts (12.5%) presented an inguinal relapse. The 5-years inguinal-DFS in these 2 groups of patients rates were 87.5% and 90.7%, respectively (p=0.38).
Table 2 summarizes results in terms of specificity, sensitivity and accuracy of the 3 considered AI-based methods in identifying patients that would relapse.
Table 2: Performances of the 3 proposed machine learning techniques in identifying patients that would relapse (results on training set and on testing set are showed)
AI approaches |
False + (FP) |
False - (FN) |
True + (TP) |
True - (TN) |
Specificity |
Sensitivity% |
Accuracy% |
|---|---|---|---|---|---|---|---|
J48 |
39 |
41 |
29 |
121 |
75.6 |
41.4 |
65.2 |
Random Tree |
31 |
4 |
66 |
129 |
80.6 |
94.3 |
84.8 |
Random Forest |
16 |
5 |
65 |
144 |
90.0 |
92.9 |
90.9 |
AI approaches |
False + (FP) |
False - (FN) |
True + (TP) |
True - (TN) |
Specificity |
Sensitivity% |
Accuracy% |
J48 |
8 |
3 |
3 |
51 |
86.4 |
50.0 |
83.1 |
Random Tree |
12 |
5 |
1 |
47 |
79.7 |
16.7 |
73.9 |
Random Forest |
9 |
4 |
2 |
50 |
84.8 |
33.3 |
80.0 |
LR |
6 |
2 |
1 |
54 |
90.1 |
33.3 |
87.0 |
Always Negative |
60 |
3 |
0 |
60 |
100.0 |
0.0 |
95.2 |
*The total number of patients in this table seems to be different from the total number of 194 pts only because of the Oversampling that has been applied. The real population accounted always for 194 pts.
** The total number of patients of the test set is 65.
Depending on the technique and the goal, the overall sensitivity, specificity, and accuracy rates of the ML techniques ranged between 41.3-94.3%, 75.6-90.0% and 65.2-90.9%, respectively, while the LR presented overall sensitivity, specificity, and accuracy rates of 36.5%, 94.8% and 80.2%, respectively.
The Random Forest was the best method in predicting patients that would relapse, with specificity, sensitivity, and accuracy rates of 90.0%, 92.9% and 90.9%, respectively (See Table 2).
Once verified on the independent testing set of 65 patients, the overall specificity, sensitivity, and accuracy rates of the ML techniques ranged between 79.7-86.4%, 16.7-50% and 73.9- 83.1% respectively (Table 2), while the LR presented overall sensitivity, specificity, and accuracy rates of 36.5%, 90.4% and 80.2%, respectively. The J48 was the best method in predicting patients that would relapse on the testing set, with specificity, sensitivity, and accuracy rates of 86.4%, 50% and 83.1% respectively.
Importance of the considered features
By applying the Information gain technique (see Methods section) to the considered dataset of patients, we found that 8 of the considered features carried a significant amount of information for the correct classification of the patients’ outcome: PS, T and N stage, uTNM, Stage of the tumor, cTNM stage, tumor site, no symptoms or pain or tenesmus at diagnosis, histology and method used for the histologic definition, the presence of positive inguinal nodes, the administration of neoadjuvant CT, the treatment of an anal canal cancer relapsing after an initial surgery. In order to validate such results, we generate new predictive models using the same ML techniques, based only on the features selected by the Information gain technique. The mean accuracy was not worsened (data not shown). Interestingly, the J48 techniques improved its accuracy while considering these 8 only selected features. It means that the excluded variables have no impact on performances, or introduce only noise. This observation, confirmed by the empirical evaluation, could be of interest in understanding the actual importance of the considered features.
Discussion (items 18-22)
We report the results of the first preliminary study exploring the potential of the innovative techniques of ML in predicting the risk of inguinal relapse in a population of 194 anal cancer patients having received or not a PII. Our results show good performances in terms of specificity, sensitivity, and accuracy of these techniques.
Subclinical inguinal metastases from anal canal cancers are not rare: their incidence is estimated at 15% to 25% in the historical surgical series [11–13].
Looking at these data, international guidelines recommend 36-45 Gy of PII in all anal cancer patients treated with radio- +/- chemotherapy [1].
Despite that, looking at the same surgical series, it should be easily argued that only 1 out 4 patients treated with PII would really benefit of the PII. These rates are lower in the early stage cancers, as it has been showed in a series by Ortholan et al., reporting a 5-year inguinal recurrence rate of 12% when omitting PII [5]. Looking at these figures, it is not strange that recent reports consider feasible and of a potential interest the reduction of the treatment fields [6], particularly in some categories of patients, presenting an increased risk of acute and late toxicity [7–9]. The overall treatment time seems to have a detrimental effect on local failure and colostomy free survival in anal cancer, and results are worst in patients presenting longer total treatment times, for example because of acute toxicity [14, 15]. On the other hand, it is also noteworthy that PII is an effective treatment: in the same study by Ortholan et al., 75 patients received PII up to a total dose of 45-50 Gy (PII group) and 106 did not receive it (no PII group) [5]. After a median followup of 61 months, 14 patients in the “no PII group” and 1 patient in the “PII group” developed an inguinal recurrence, with a 5-year cumulative rate of inguinal recurrence of 2% and 16% in “PII” and “no PII group”, respectively (p = 0.006). Finally, the real problem is to find a reliable method to deliver PII to the patients that would benefit from it, avoiding the irradiation of the 100% of the patients only to treat the 25% (or the 10%, in the case of early-stage cancers) who would really take advantage from it.
Modern highly intensity modulated radiation techniques (IMRT, Volumetric-Arc and Rotational Radiation Therapy) allow an optimal coverage of the target volumes and a better sparing of the surrounding normal tissues, with a reduction of the toxicity. In this scenario, the potential interest of a method allowing the further reduction of the treatment fields (and then of the toxicity) could be easily argued [16].
The results of this study indicate that ML techniques can be effectively exploited to help the radiation oncologists. Such techniques can accurately identify patients presenting a higher risk of inguinal relapse when they are not treated at the inguinal level, thus tailoring the prescription of the PII.
Another interesting aspect is that these predicting methods do not give a result in terms of probability rates (as those recently published for anal and rectal cancer [17, 18]). The output of these algorithms is a “yes/no” one (relapsing/not relapsing). The percentages are not percentages of risk of relapse, but percentages of accuracy of the algorithm.
For example, the J48 method has a confirmed accuracy of 83.1% in predicting the patients that would relapse. It means that the system classifies a very small percentage of the patients incorrectly. Moreover, AI-based methods could fit better than the classical multivariate analysis. In general it is not clear why so often AI-based methods fit better than the typical statistic approaches (i.e. logistic regression). The mathematical models behind the two families of approaches are very different and many factors, as the strong non-linearity of the problem or unusual stochastic distribution of the involved variables, could play a major role in explaining the better performances of the ML techniques. ML encompasses most of the multivariate analysis techniques. Generally speaking, most of the multivariate statistics exploit a subset of the ML approaches: usually unsupervised linear regression. In fact, ML provides a wide range of approaches that can be fruitfully exploit, as demonstrated in our work. Moreover, supervised ML techniques (as those we used) put emphasis on the prediction, i.e. the analysis is focused on identifying patterns that maximises the possibility of providing a correct prediction. On the contrary, multivariate analysis emphasises inference: patterns in the values of features are analysed regardless of their actual usefulness for predicting the outcome.
Noteworthy, Institutional treatment protocols were different in the 2 Institutions in terms of radiotherapy volumes and type of CT but, despite these important differences, ML techniques were able to correctly classify most of the patients of the testing set.
Additionally, ML techniques are able to provide some insights about the importance of considered attributes in a correct classification of the patients in the data set. The results of this analysis indicate that a smaller number of attributes are sufficient to generate good performance decision trees and so, such attributes are somehow related with the actual outcome of an anal cancer patient.
Despite the good performances of these ML-based methods, some improvements could be probably implemented in the next future, in order to increase the potential interest of these innovative approaches in the daily clinical practice.
It could be useful to integrate the variable of the timing of the relapse (i.e. to create different algorithms to predict the risk of inguinal relapse, for example, at 3 and 5 years): it could have a potential interest in deciding if irradiate or not the inguinal nodes in more elderly patients, allowing avoiding the PII in patients with shorter life expectancy.
Moreover, these results have been obtained on a monoinstitutional series (even if 62.4% of the patients have been treated in Radiotherapy Centers other than the “Leon Berard Center”): a confirmatory study performed on a large, independent population will allow to confirm and to strengthen our data.
These AI-based methods share the problem of needing a software (or a website) to be widely diffused: our team is already working on the creation of these informatics tools, but we prefer to confirm the performances of the algorithms in larger and/or independent population, before to finalize and diffuse them in the web. Figure 1a and 1b show some snapshots of the beta version of the open-access website that is currently under-construction and will be soon available online.
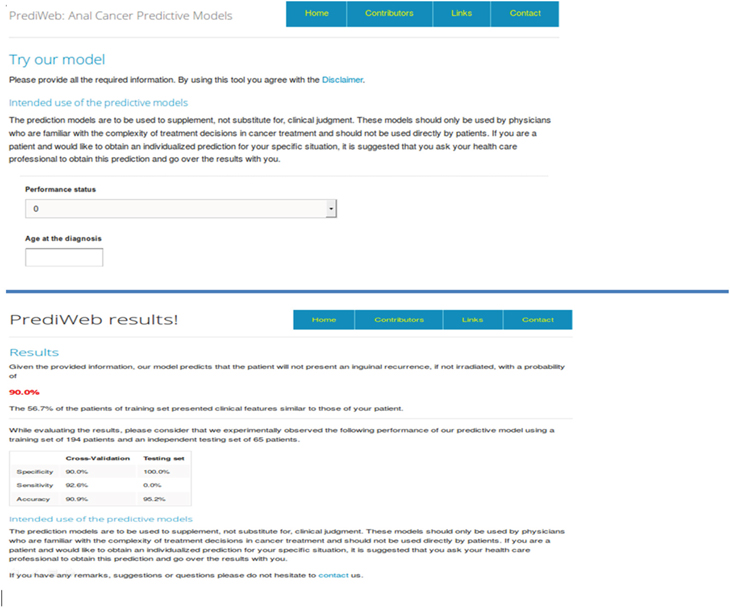
Figure 1: a-b. Screen shots taken from the PrediWeb website. The Figure 2a shows the modality of introduction of the variables (the same that have been implemented to obtain the algorithms, see Table 4), and Figure 1b shows an example of the results given by the website once all the parameters have been introduced.
MATERIALS AND METHODS
The TRIPOD statement
The TRIPOD (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis) Statement is a 22-item checklist, created to improve the reporting of studies dealing with the development and validation of diagnostic or prognostic predictive models [19]. Table 1 summarizes the items of the TRIPOD, and we followed this statement both to create and validate our model, and to present it in this article. No funds were obtained for this research (item 22).
Participants (items 4a – 5c, 8,9 and 12)
Patients presenting an histologically proven ACC were the target population. The training set was constituted by patients consecutively addressed to the Radiation Oncology Department of the “Léon Bérard” Anticancer Center (Lyon, France) to receive brachytherapy after a first course of radiotherapy +/- chemotherapy (received in the same Center or in other Radiotherapy departments of the Rhone-Alpes Region) from may 1992 to december 2009.
The initial whole population accounted for a total of a population of 209 patients. Fifteen patients were excluded from the final analysis as at least one of the considered clinical and/or therapeutic variables was lacking (see “Experimental design” section for the variables). Finally, 194 patients were used as training sets. The Male/Female ratio was 32/162 and the median age was 64 years (range: 36-88). Median follow-up was 72.8 months.
We used an independent testing set of 65 patients affected by an histologically proven ACC consecutively treated with curative radiotherapy +/- chemotherapy at the Academic Radiation Oncology Department of the Catholic University (Rome, Italy) from Mars 1990 to August 2013. The mean follow-up was 43 months. None of the patients treated in this Department in the considered period has been excluded.
Table 3 summarizes features and differences of patients considered in the training and in the testing set, as well as their tumors characteristics (staged according to the 2002 International Union against Cancer Classification (UICC 2002) [20]) and treatment features.
Table 3: Description of the clinical and therapeutic features of the populations
|
Testing set |
Testing set |
||
|---|---|---|---|---|
|
n. |
% |
n. |
% |
Patients (n) |
194 |
100 |
65 |
100 |
Sex (n) |
32 |
17 |
13 |
20 |
Age (y) |
63.6 |
- |
60.2 |
- |
Performance Status |
40 |
21 |
51 |
78 |
SYMPTOMS |
6 |
3 |
0 |
57 |
Endorectal Echography |
130 |
67 |
21 |
33 |
MRI |
44 |
23 |
35 |
54 |
Description of the disease |
||||
Location (n) |
98 |
51 |
27 |
42 |
Tumor |
21 |
11 |
6 |
10 |
Histologic Subtype (n) |
4 |
2 |
0 |
|
Nodal Status |
140 |
72 |
31 |
48 |
Staging TNM |
19 |
10 |
6 |
10 |
Histological Procedures |
182 |
94 |
53 |
81 |
Squamous Cell Carcinoma Antigen* |
2 |
5.6 |
||
* Available for only 15 patients in the training set. |
||||
EBRT details |
||||
Total Dose (Gy) |
45Gy [36–56] |
55 [30.6-58.5] |
||
Pelvic Volume (patients) |
152 |
78 |
12 |
18 |
Inguinal irradiation (patients) |
151 |
78 |
4 |
6 |
Type of beams (patients) |
187 |
96 |
65 |
100 |
Field Balistic (patients) |
147 |
75 |
50 |
77 |
Median number of fractions [range] |
25 [12–30] |
27 [17–34] |
||
RT Duration in days [range] |
36 [15–63] |
56 [22–88] |
||
BRT details |
||||
Interval between RT and BRT (days) |
32 |
|
- |
- |
BRT technique |
143 |
74 |
- |
- |
Median dose [range] |
18 [10-31.7] |
- |
- |
|
Median duration of BRT in hours [range] |
22 [11–77] |
- |
- |
|
Number of sources [range] |
6 [4–12] |
- |
- |
|
Median length of sources (cm, range) |
5 [4–9] |
- |
- |
|
Median total dose RT + BRT (Gy, range) |
64 [54-76.7] |
- |
- |
|
Concomitant Chemotherapy details |
|
|
|
|
Schedule (patients) |
52 |
27 |
5 |
8 |
CT Protocol |
102 |
72 |
5 |
8 |
Neoadjuvant CT |
18 |
9 |
2 |
3 |
Outcomes (items 6a-6b)
Aim of this study was to develop a model instructed to recognize patients who would relapse if not irradiated on the inguinal groin. Because of the intrinsic nature of an automated method, we do not use any action to blind assessment of the outcome to be predicted.
Predictors (items 7a-7b)
The performances of a classic Logistic Regression (LR) has been tested and compared to the results of the ML algorithms for the considered outcome.
For each patient, a large set of clinical or therapeutic features considered as potential predictors of microscopic inguinal involvement were included in the generation of the predictive models (see Table 4). Because of the intrinsic nature of an automated method, we do not use any action to blind assessment of the outcome to be predicted.
Table 4: Features considered for the development of the predictive model
Variable |
Accepted values |
|---|---|
Performance Status |
From 0 to 4 |
Age at the diagnosis |
≥ 18 years |
Initial level of SCC antigen |
All values ≥ 0.1 |
RT+/-CT after a not-curative surgical resection |
Yes/No |
Histologic type |
In situ carcinoma, large cells keratinizing SCC, not keratinizing SCC, basaloid, ADK, ADK developed on a ano-rectal fistula, small cell carcinoma, undifferentiated, cloacogenic, others |
Symptoms at the moment of the diagnosis |
No symptoms, rectal bleeding, anal/rectal pain, anal swelling/hemorrhoids, positive inguinal nodes, rectal syndrome, defecation troubles, other. |
Method used for the histological definition |
Only biopsy, R0 surgical excision, R1 surgical excision, R2 surgical excision. |
T side |
Anal canal, anorectal junction, anal margin, anal canal with rectal extension |
T stage |
From 1 to 4 |
N stage |
From 0 to 3 |
Staging methods |
Only clinics, echoendoscopy, MRI |
uTNM stage |
Depending on the T and N stage established with echography |
cTNM stage |
Depending on the T and N stage established with clinical examination and staging examens |
Neoadjuvant CT |
Yes/No |
Concomitant CT |
Yes/No |
Type of concomitant CT |
5FU-CDDP |
type of inguinal irradiation |
curative/prophylactic |
Legend: SCC = squamous cell carcinoma; ADK = adenocarcinoma; CDDP = cisplatin; 5-FU = 5-fluorouracile; MMC = mitomycine.
Statistical methods (items 10a-e and 11)
The correct selection of the best classification technique is crucial: it should be an automated system being reliable, allowing accurate predictions and, at the same time, easy to be explained and represented. We decided to adopt ML techniques based on the decision trees (the J48 [21], the Random Tree [22] and the Random Forest [23]). The methodology that we adopted has been previously described and detailed in a previous study by our group [24].
Two risk groups were created, according to the outcome of the treatment in terms of relapse. The largest one accounted for 160 patients, and it referred to patients who, regardless to the received treatment, did not relapse. The risk group that the model should predict was the alternative one, including only the relapsing patients. This class accounted for 34 patients. As it could be easily argued, these population are quite unbalanced. Thus, we adopted the random oversampling to take into account the imbalanced patients distribution among these 2 groups [25]. Random oversampling is frequently adopted in AI studies, and it increases the number of elements of the less represented class (relapsing patients, in our population) by randomly considering more than once some of these patients. After the application of this technique, classes had a distribution of about 70%-30% of, respectively, non-relapsing and relapsing patients [26]. Finally, the considered population is composed by 230 patients; 160 of them did not relapse, while 70 of them are members of the relapsing class. It is worth to note that oversampling could lead to overfitting, which results in over-structured models that are too focused on training population.
As it is also stated in the TRIPOD statement, it should be avoided to evaluate the performances of a model on the same data from which the model was developed. Indeed, it could overestimate its performances, owing to overfitting (too few outcome events relative to the number of candidate predictors). For this reason, some forms of internal validation, as bootstrapping or cross-validation, should always be part of the development of a new prediction model. This is also clearly stated in the TRIPOD indications. In our study, each of the selected classifying techniques was trained on the previously described data sets separately, and the resulting predictive models were then evaluated using a k-fold cross-validation strategy [27]. Models have been evaluated by considering their accuracy, specificity and sensitivity. Accuracy indicates the proportion of patients of the given class correctly classified. Sensitivity is the ability of the model to correctly classify a patient in a given class. Specificity relates to the ability of the generated algorithm to identify and classify patients as not to be members of a given class, and that are actually not members of the considered class. In order to compare the performances of ML techniques with a more common statistical approach, we trained a LR model using the same k-fold cross-validation schema. The used algorithm was the one implemented in R software (version 3.0.0) [28] ant it was based on the generalized linear model inspired from Hastie et al [29].
Finally, performances of the obtained models have been verified on a testing set of 65 anal canal cancer patients treated in another Radiotherapy Department (Catholic University, Rome, Italy).
Last but not least, we decided to define an intuitive ordering of the importance of the considered features, in order to assess those having a major role in the prediction. We applied the Information gain technique [30, 31]. This technique, widely adopted in ML applications, is based on an evaluation of the information that each feature carries with regard to the class to predict. Globally, it measures the information that is lost when a single feature, or a subset of the available features, is used to approximate the class to predict.
CONCLUSION
ML-based methods seem promising tools in predicting patients who are the best candidates to the PII, with very good performances in terms of sensibility, sensitivity and accuracy. ML could potentially help the Radiation Oncologist in the selection not only of those patients who would benefit of the PII, but also of those that would only be exposed to the potential toxicity of this treatment, increasing the therapeutic ratio of the treatments. These interesting results should to be confirmed in larger and/or independent populations of ACC patients.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDINGS AND FINANCIAL DISCLOSURES
The work had no specific funding. Authors have no financial disclosures to declare.
REFERENCES
1. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#anal.
2. Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR anal cancer trial working party. UK Co-ordinating committee on cancer research. Lancet 1996; 348:1049–54.
3. Bartelink H, Roelofsen F, Eschwege F, Rougier P, Bosset JF, Gonzalez DG, Peiffert D, van Glabbeke M, Pierart M. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European organization for research and treatment of cancer radiotherapy and gastrointestinal cooperative groups. J Clin Oncol. 1997; 15: 2040–2049.
4. Flam M, John M, Pajak TF, Petrelli N, Myerson R, Doggett S, Quivey J, Rotman M, Kerman H, Coia L, Murray K. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J Clin Oncol. 1996; 14: 2527–2539.
5. Ortholan C, Resbeut M, Hannoun-Levi JM, Teissier E, Gerard JP, Ronchin P, Zaccariotto A, Minsat M, Benezery K, François E, Salem N, Ellis S, Azria D, et al. Anal canal cancer: management of inguinal nodes and benefit of prophylactic inguinal irradiation (CORS-03 Study). Int J Radiat Oncol Biol Phys. 2012; 82: 1988-95.
6. Crowley C, Winship AZ, Hawkins MA, Morris SL, Leslie MD. Size does matter: can we reduce the radiotherapy field size for selected cases of anal canal cancer undergoing chemoradiation? Clin Oncol (R Coll Radiol). 2009; 21: 376-9.
7. Lestrade L, De Bari B, Montbarbon X, Pommier P, Carrie C. Radiochemotherapy and brachytherapy could be the standard treatment of anal canal cancer in elderly patients? A retrospective single centre analysis. Med Oncol. 2013;30:402. doi: 10.1007/s12032-012-0402-x. Epub 2013 Jan 16.
8. Fraunholz I, Rabeneck D, Gerstein J, Jäck K, Haberl A, Weiss C, Rödel C. Concurrent chemoradiotherapy with 5-fluorouracil and mitomycin C for anal carcinoma: are there differences between HIV-positive and HIV-negative patients in the era of highly active antiretroviral therapy? Radiother Oncol. 2011; 98: 99-104.
9. Regnier-Coudert O, McCall J, Lothian R, Lam T, McClinton S, N'dow J. Machine learning for improved pathological staging of prostate cancer: a performance comparison on a range of classifiers. Artif Intell Med. 2012; 55: 25-35.
10. Delen D, Walker G, Kadam A. Predicting breast cancer survivability: a comparison of three data mining methods. Artif Intell Med. 2005; 34: 113-27.
11. Moons KG, Altman DG, Reitsma JB, Ioannidis JP, Macaskill P, Steyerberg EW, Vickers AJ, Ransohoff DF, Collins GS. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): explanation and elaboration. Ann Intern Med. 2015; 162: W1-73.
12. Sobin LH, Gospodarowicz MK, Wittekind Ch. Eds. TNM Classification of Malignant Tumors, 7th ed. Wiley-Blackwell, Oxford 2009. (ISBN 978-1-4443-3241-4).
13. Quinlan JR. C4.5: programs for machine learning. Burlington: Morgan Kaufmann. 1993.
14. Fan W, Wang H, Yu P, Ma S. Is random model better? on its accuracy and efficiency. In: Shavlik J, Wu X, Tuzhilin A, editors. Proceedings of the 3rd IEEE International Conference on Data Mining. Washington: IEEE, 2003: 51-58.
15. Breiman L. Random forests. Machine Learning 2001; 45: 5-32.
16. De Bari B, Vallati M, Gatta R, Simeone C, Girelli G, Ricardi U, Meattini I, Gabriele P, Bellavita R, Krengli M, Cafaro I, Cagna E, Bunkheila F, et al. Could Machine Learning Improve the Prediction of Pelvic Nodal Status of Prostate Cancer Patients? Preliminary Results of a Pilot Study. Cancer Invest. 2015; 33: 232-40
17. He H, Garcia EA. Learning from imbalanced data. IEEE Transactions on Knowledge and Data Engineering. 2009; 21: 1263-1284.
18. Van Hulse J, Khoshgoftaar TM, Napolitano A. Experimental perspectives on learning from imbalanced data. In: Ghaharamani Z, editor. Proceedings of the 24th International Conference on Machine learning. New York: ACM, 2007: 935-942.
19. Witten IH, Frank E, Hall MA. Data Mining: Practical Machine Learning Tools and Techniques. 3rd Ed. Burlington: Morgan Kaufmann. 2011.
20. R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available at http://www.R-project.org/. 2013.
21. Hastie TJ, Pregibon D. Generalized linear models. Chapter 6 of Statistical Models in S. Eds Chambers JM, Hastie TJ, Wadsworth & Brooks/Cole,1992.
22. Novakovic J. Using Information Gain Attribute Evaluation to Classify Sonar Targets, 17th Telecommunications forum, 2009.
23. Kullback S. Letter to the Editor: The Kullback–Leibler distance. The American Statistician. 1987; 41: 340–341.
24. Boman BM, Moertel CG, O'Connell MJ, Scott M, Weiland LH, Beart RW, Gunderson LL, Spencer RJ. Carcinoma of the anal canal. A clinical and pathologic study of 188 cases. Cancer. 1984; 54: 114-25.
25. Golden GT, Horsley JS 3rd. Surgical management of epidermoid carcinoma of the anus. Am J Surg. 1976; 131: 275-80.
26. Stearns MW Jr, Urmacher C, Sternberg SS, Woodruff J, Attiyeh F. Cancer of the anal canal. Curr Probl Cancer. 1980; 4: 1-44.
27. Roohipour R, Patil S, Goodman KA, Minsky BD, Wong WD, Guillem JG, Paty PB, Weiser MR, Neuman HB, Shia J, Schrag D, Temple LK. Squamous-cell carcinoma of the anal canal: predictors of treatment outcome. Dis Colon Rectum. 2008; 51: 147-53.
28. Ben-Josef E, Moughan J, Ajani JA, Flam M, Gunderson L, Pollock J, Myerson R, Anne R, Rosenthal SA, Willett C. Impact of overall treatment time on survival and local control in patients with anal cancer: a pooled data analysis of Radiation Therapy Oncology Group trials 87-04 and 98-11. J Clin Oncol. 2010; 28: 5061-6.
29. Bazan JG, Hara W, Hsu A, Kunz PA, Ford J, Fisher GA, Welton ML, Shelton A, Kapp DS, Koong AC, Goodman KA, Chang DT. Intensity-modulated radiation therapy versus conventional radiation therapy for squamous cell carcinoma of the anal canal. Cancer. 2011; 117: 3342-51.
30. Glynne-Jones R, Sebag-Montefiore D, Adams R, Gollins S, Harrison M, Meadows HM, Jitlal M; United Kingdom Coordinating Committee on Cancer Research Anal Cancer Trial Working Party. Prognostic factors for recurrence and survival in anal cancer: generating hypotheses from the mature outcomes of the first United Kingdom Coordinating Committee on Cancer Research Anal Cancer Trial (ACT I). Cancer. 2013; 119: 748-55.
31. Valentini V, van Stiphout RG, Lammering G, Gambacorta MA, Barba MC, Bebenek M, Bonnetain F, Bosset JF, Bujko K, Cionini L, Gerard JP, Rödel C, Sainato A, et al. Nomograms for predicting local recurrence, distant metastases, and overall survival for patients with locally advanced rectal cancer on the basis of European randomized clinical trials. J Clin Oncol. 2011; 29: 3163-72.