
INTRODUCTION
Imatinib (Glivec®, Novartis Pharmaceuticals Corporation), along with other tyrosine kinase inhibitors (TKIs), has revolutionized treatment of chronic myelogenous leukemia (CML). Long-term follow-up of the IRIS pivotal study revealed that overall survival for patients who received imatinib as initial therapy was as high as 88% at 6 years [1]. Two second generation TKIs, dasatinib (Sprycel®, Bristol-Myers Squib) and nilotinib (Tasigna®, Novartis Pharmaceuticals Corporation) are now registered as frontline therapy for chronic phase CML (CP-CML) patients. Recent studies reported faster and deeper responses assessed by cytogenetic or molecular analysis with these drugs [2-3], however data are yet too preliminary to determine whether these agents will offer a survival advantage over imatinib. Comorbidities, age, and co-medications tend to drive the choice of the TKI in first-line therapy. Emerging reports of adverse events with nilotinib (peripheral arterial occlusive disease) [4] and dasatinib (pulmonary hypertension) [5] along with the upcoming arrival of generic imatinib will move TKI therapy towards a personalized approach. Disease-related factors such as initial Sokal score have been shown to influence molecular responses [6-9], however, few patient-related parameters such as adherence to therapy or trough imatinib levels have been evaluated [10-12].
Association studies have suggested that single nucleotide polymorphisms (SNPs) may be related to a susceptibility to develop CML [13-16], CML progression [17-18] or intracellular accumulation of imatinib in leukocytes of CML patients [19]. Only a limited number of selected SNPs have been tested in relation to imatinib response[20-28], and results obtained with the most extensively studied gene ABCG1 (MDR1) are not consistent across published analyses[29-30]. Complete cytogenetic response (CCR) at 12 months remains the best surrogate marker for survival in CML patients. However, major molecular response (MMR, defined by BCR-ABL≤0.1%) was used as a primary end point of clinical trial (such as in the ENEST 1st study) [31] and MMR at 18 months is also part of the “optimal response” definition of the ELN2009 recommendation for CML patient management [32]. We thus selected cumulative incidence of major molecular response (CI-MMR) as a criteria to identify SNPs in drug transporter genes which are associated with a favorable outcome. We performed an association study using a custom-made DNA chip in an exploratory cohort. An ABCG2 haplotype associated with high CI-MMR was identified. We then validated this haplotype in an independent “prospective-retrospective” cohort[33], and evaluated its impact according to imatinib daily dose.
RESULTS
Patient characteristics are presented in Table 1. Median age, sex ratio and Sokal score distribution were comparable between all cohorts (P > 0.05 in all cases).
Table 1: Patient characteristics
|
|
Saint-Louis Exploratory Cohort (SLEC) |
SPIRIT Validation Cohort (SVC) |
Total |
||
|
|
(400 mg) N=105 |
(400 mg) N=132 |
(600 mg) N=107 |
(SVC) N=239 |
N=344 |
Gender |
Male |
63 (60%) |
88 (67%) |
52 (49%) |
143 (60%) |
206 (60%) |
Female |
42 (40%) |
44 (33%) |
55 (51%) |
96 (40%) |
138 (40%) |
|
Sokal Score
|
Low |
34 (32%) |
52 (39%) |
38 (36%) |
90 (38%) |
124 (36%) |
Int. |
24 (23%) |
54 (41%) |
45 (42%) |
99 (41%) |
123 (36%) |
|
High |
15 (14%) |
26 (20%) |
24 (22%) |
50 (21%) |
65 (19%) |
|
NA* |
32 |
0 |
0 |
0 |
32 |
|
Median age (years) |
50.5 |
51.8 |
51.5 |
51.5 |
51.5 |
|
All p values of differences among groups were not significant
* Not available
Determinants of CI-MMR
CI-MMR were estimated according to Sokal score (n = 312). Using the Fine and Gray model we confirmed that CI-MMR was strongly related to Sokal score levels (regression coefficient: 0.64, 95% confidence interval (CI), 0.53 to 0.78, P < 0.001). Figure 1A illustrates the inverse relationship between Sokal score and CI-MMR.
CI-MMR was estimated in the SLEC (n = 105), SVC (n = 239), and in the two imatinib SVC treatment arms (n = 132 at 400 mg/d; n =107 at 600 mg/d; Figure 1B). CI-MMR was comparable between the SLEC and the SVC 400 mg/d arm (P = 0.700), but was significantly higher in the SVC 600 mg/d arm (P = 0.003). The regression coefficient increased by more than 50% (1.53, 95% CI, 1.09 to 2.14) when the dose increased from 400 mg/d to 600 mg/d (P = 0.014).
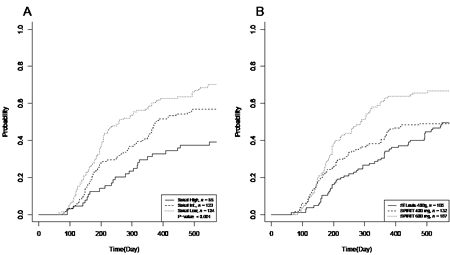
Figure 1: Cumulative incidence of MMR (CI-MMR) according to Sokal score and treatment arms. A) 18 months CI-MMR was estimated with respect to Sokal score (n = 312). A Fine and Gray model showed that time to MMR was related to Sokal status and that the coefficient of regression within the first 18 months decreased by 36% (95% confidence interval (CI), 47% to 22%) on average when Sokal increased (P < 0.001). CI-MMR was 70% for the low Sokal score, 57% for the intermediate Sokal score and 39% for high Sokal score. B) CI-MMR was estimated in the exploratory cohort (SLEC) and compared to both treatment arms of the validation cohort (SVC). CI-MMR was comparable between the SLEC and the 400 mg/d arm of SVC (n = 237, P = 0.700), but significantly different between the SLEC and the 600 mg/d arm of SVC (n = 212, P = 0.003). HR was 1.71% (95% CI, 1.20% to 2.44%) in the latter (n = 212, P = 0.003). CI-MMR was 49% for the exploratory cohort, 49% and 67% for the 400 and the 600 mg/d arm of the SVC, respectively.
SNP association study
Of the 857 selected SNPs, 413 (48.2%) from 86 drug transporters were well genotyped in all evaluated patients and passed quality control criteria. We identified 12 SNPs (located in eight transporter genes) in the SLEC group which were significantly associated with CI-MMR at 18 months on the basis of an FDR < 50% (Table 2). Only one of these SNPs (rs12505410), located in the ABCG2 gene, was significantly associated with CI-MMR in the overall SVC cohort. Separate analysis of the two SVC cohorts revealed three SNPs (rs12505410, rs13120400 and rs2725252), all from the ABCG2 gene, which were significantly associated with response in the 400 mg/d arm while none were associated in the 600 mg/d arm. CI-MMR at 18 months in the two SVC groups for the three validated ABCG2 SNPs is shown in Supplementary Figure SF1.
Table 2: Drug transporter SNPs associated with CI-MMR at 18 months
SNP |
Chr. |
Coordinate |
Transporter gene symbol |
SLEC |
SVC (P-value) |
|||
P-value |
FDR |
All |
400 mg/d |
600 mg/d |
||||
rs609468 |
6 |
160498904 |
SLC22A1 |
<0.001 |
0.001 |
0.920 |
0.210 |
0.090 |
rs10841907 |
12 |
21942563 |
ABCC9 |
0.001 |
0.238 |
0.310 |
0.670 |
0.450 |
rs12505410 |
4 |
89249865 |
ABCG2 |
0.002 |
0.238 |
0.045* |
0.035* |
0.320 |
rs4149182 |
11 |
62524689 |
SLC22A8 |
0.002 |
0.238 |
0.750 |
0.640 |
0.820 |
rs1189451 |
13 |
94520087 |
ABCC4 |
0.005 |
0.430 |
0.260 |
0.360 |
0.330 |
rs17556915 |
14 |
69318111 |
SLC10A1 |
0.008 |
0.482 |
0.068 |
0.130 |
0.230 |
rs11024300 |
11 |
17452549 |
ABCC8 |
0.009 |
0.482 |
0.870 |
0.550 |
0.160 |
rs13120400 |
4 |
89252551 |
ABCG2 |
0.012 |
0.482 |
0.140 |
0.046* |
0.740 |
rs2725252 |
4 |
89280934 |
ABCG2 |
0.012 |
0.482 |
0.086 |
0.047* |
0.740 |
rs2665691 |
11 |
22327832 |
SLC17A6 |
0.012 |
0.482 |
0.075 |
0.110 |
0.360 |
rs1678405 |
13 |
94627682 |
ABCC4 |
0.014 |
0.482 |
0.710 |
0.850 |
0.370 |
rs1048099 |
11 |
17453092 |
ABCC8 |
0.014 |
0.482 |
0.950 |
0.220 |
0.150 |
Chr., chromosome; FDR, false discover rate; SNP, single nucleotide polymorphism
* Significant association between CI-MMR and SNP (P < 0.05)
Haplotype frequency
As expected, pairwise linkage disequilibrium was found between the three SNPs at the ABCG2 locus in the SLEC. We therefore performed haplotyping at this locus. Estimated frequencies was 22% for haplotype 1 (G-C-G) having G, C and G bases at loci rs12505410, rs13120400 and rs2725252, respectively, < 1% for haplotype 2 (G-C-T), 5% for haplotype 3 (G-T-G), 15% for haplotype 4 (T-T-G), 57% for haplotype 5 (T-T-T) and 2% for haplotype 6 (G-T-T) (Supplementary Table ST2).
Haplotype frequencies at the same loci were also calculated in the independent set of unrelated individuals from the CEU population (n = 76). Frequency of haplotype 1 plus 3 was 27% in the SLEC versus 28% in the CEU population, 56% versus 55% for haplotype 5 and 16% versus 17% for other haplotypes. Equal distribution of haplotypes between populations was confirmed (P = 0.70; Figure 2A and Supplementary Table ST2).
Haplotype association study
CI-MMR at 18 months was evaluated with respect to ABCG2 haplotype distribution in the exploratory cohort. Multivariate analysis identified haplotypes 1 and 3 (G-C-G and G-T-G respectively) as linked to significantly higher CI-MMR rates. These two haplotypes share the same alleles at rs12505410 and rs2725252 and differ at rs13120400, suggesting that the association could be with the G-G haplotype at these two SNPs; carriers of the G-G haplotype at rs12505410 and rs2725252 had significantly higher CI-MMR than non-carriers (Figure 2B).
The validation cohort was analyzed using the same approach. Haplotype frequencies at ABCG2 locus were verified as being comparable to the SLEC and the CEU populations (Figure 2A). This confirmed the analysis in the SVC population was performed according to the same assumptions as for the exploratory cohort and was analyzed overall and by treatment arms (Figure 2 C, D, E and F and Table 3).
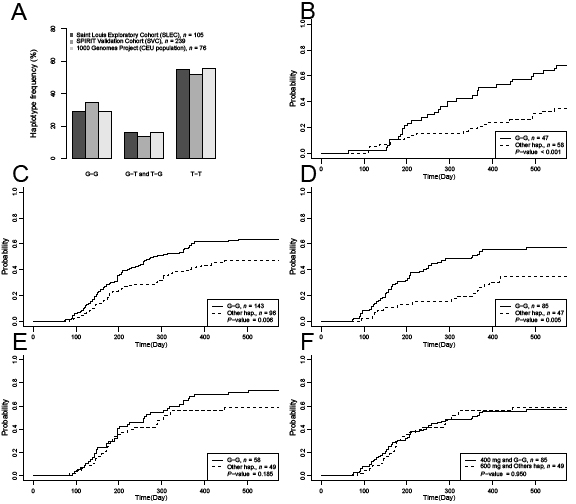
Figure 2: Frequencies and cumulative incidence of MMR relative to ABCG2 haplotypes. A) Distribution of haplotype frequencies in the SLEC, SVC and the CEU populations. Haplotypes were distributed homogeneously over the different populations. B) Cumulative incidence at 18-months of major molecular response (CI-MMR) was calculated in the SLEC according to ABCG2 haplotypes G-G. CI-MMR of patients with at least one copy of haplotype G-G was 69%. CI-MMR for other patients was 34%. C) CI-MMR at 18-months in all SVC patients with haplotype G-G was 63% and 47% for other patients (P = 0.006). D) CI-MMR in SVC patients treated with 400 mg/d was 57% and 36% for G-G haplotype carriers and other haplotype carriers respectively (P = 0.005). E) CI-MMR in SVC patients treated with 600 mg/d was 74% and 58% for G-G haplotype carriers and other patients respectively (P = 0.185). F) CI-MMR was not significantly different between in SVC patients with haplotype G-G receiving 400 mg/d and those with other haplotypes receiving 600 mg/d (57% vs 58% respectively, P = 0.950).
In the overall SVC, 18-month CI-MMR increased by 36% for patients with one copy of haplotype G-G (P = 0.005, Figure 2C). In patients included in the imatinib 400 mg/d arm, 18-month CI-MMR increased by 64% (P = 0.002, Figure 2D). Association of haplotype G-G with CI-MMR in patients included in the imatinib 600 mg/d arm was not significant (P = 0.180, Figure 2E). CI-MMR curves of patients with haplotype G-G included in the imatinib 400 mg/d arm were comparable to those of patients with other haplotypes in the imatinib 600 mg/d arm (Figure 2F, P = 0.480). Of note, Sokal score remained an independent determinant of CI-MMR in all populations in a multivariate model (Table 3).
Table 3: ABCG2 haplotype associated with CI-MMR at 18 months
SLEC |
SVC |
||||||||
All patients |
400 mg/d |
600 mg/d |
|||||||
Univariate |
n = 105 |
(P-value) |
n = 239 |
(P-value) |
n = 132 |
(P-value) |
n = 107 |
(P-value) |
|
G-G |
68.09 |
(<.001) |
63.72 |
(.006) |
56.90 |
(.005) |
73.68 |
(.185) |
|
Other haplotypes |
34.48 |
46.81 |
34.78 |
58.33 |
|||||
Bivariate Fine and Gray model statistics |
n = 73 |
|
n = 239 |
|
n = 132 |
|
n = 107 |
|
|
G-G |
Reg. Coef. |
2.27 |
(.006) |
1.75 |
(.002) |
2.41 |
(.002) |
1.32 |
(.270) |
95%CI |
1.26 to 4.10 |
1.22 to 2.51 |
1.39 to 4.19 |
0.81 to 2.15 |
|||||
Sokal score |
Reg. Coef. |
0.64 |
(.024) |
0.62 |
(<.001) |
0.68 |
(.034) |
0.51 |
(.001) |
95%CI |
0.43 to 0.94 |
0.49 to 0.78 |
0.47 to 0.97 |
0.38 to 0.69 |
|||||
As expected from results of the Fine and Gray model in the validation cohort, early molecular responses (BCR-ABLIS at 3 months ≤ 10%) as well as responses of interest (BCR-ABLIS at 12 months ≤ 1%, BCR-ABLIS at 18 months ≤ 0.1%) were associated with the ABCG2 G-G haplotype in patients treated with imatinib 400 mg/d (Table 4).
Table 4: Association between ABCG2 haplotype and molecular response in the SVC
BCR-ABLIS ≤ 10% at 3 months |
BCR-ABLIS ≤ 1% at 12 months |
BCR-ABLIS ≤ 0.1% at 18 months |
||||||||
Imatinib |
Response |
Haplotype |
Others |
P-value |
Haplotype |
Others |
P-value |
Haplotype |
Others |
P-value |
400mg |
Yes |
52 |
14 |
0.001* |
53 |
19 |
0.025* |
48 |
16 |
0.022* |
No |
33 |
33 |
32 |
28 |
37 |
31 |
||||
600mg |
Yes |
41 |
28 |
0.209 |
43 |
31 |
0.316 |
41 |
28 |
0.209 |
No |
17 |
21 |
15 |
18 |
17 |
21 |
||||
* Significant association between ABCG2 haplotype and molecular response (P < 0.05)
Using the CEU population genotypes, we tested associations between haplotype G-G and 1772 SNPs near or within the ABCG2 gene (including rs2231135, rs2231137 and rs2231142). We identified 240 SNPs with alleles in linkage disequilibrium with the haplotype G-G. Interestingly rs2231135, located in the 5’UTR and potentially linked to ABCG2 differential expression, was significantly linked to haplotype G-G (P = 0.043).
DISCUSSION
We report here a haplotype/CI-MMR association study in two independent cohorts of CP-CML patients receiving imatinib, in which patients were genotyped using a custom-made DNA chip [34] mainly containing tag SNPs. The exploratory SLEC cohort reflected real-life practice with patients treated at imatinib 400 mg/d, while the validation SVC cohort was composed of patients included in the SPIRIT clinical trial and randomized to imatinib 400 mg/d or imatinib 600 mg/d. We used the first cohort to perform an association study with a large number of drug transporter genes SNPs in CP-CML patients and the second cohort in order to validate these results.
Studies evaluating SNPs in CML patients have been performed on a small number of genes pre-selected for their potential relationship to response [20-28]. However, the clinical significance of these results is far from established, firstly because different genes were analyzed by different groups and secondly when the same gene was studied, the SNPs analyzed were not the same. Accordingly, only two genes have been tested in a validation cohort. One of them was confirmed (IFN-γ) [25] whereas results for ABCG1 were not reproducible or were contradictory [26-30].
Our approach confirmed known key data: the inverse relationship between MMR rates and Sokal score and significantly higher MMR rates at 12 and 18 months with 600 mg imatinib compared to 400 mg [35-36]. We have extended these results with the identification of an ABCG2 haplotype associated with significantly higher CI-MMR in two patient groups receiving 400 mg/d imatinib (i.e. a real-life and a clinical setting). Patients with at least one copy of haplotype G-G (G at rs12505410 and G at rs2725252) were good responders at 400 mg. This “favorable” haplotype is widespread; about half of the population in our study carries at least one copy. Interestingly, patients in the validation cohort treated at 600 mg/d who did not carry this haplotype showed similar CI-MMR levels as haplotype carriers treated at 400 mg/d. Moreover, the clinical pertinence of these results is supported by the association of the G-G ABCG2 haplotype with the early molecular response at 3 months and responses of interest at 12 and 18 months.
The ATP-binding cassette transporter ABCG2 (BCRP, MXR or ABCP) is highly expressed in the gastrointestinal tract and liver, and is involved in absorption, distribution and excretion of a wide variety of clinically relevant drugs, among them imatinib [37-38]. Germline polymorphisms in the ABCG2 gene have been described as affecting expression, cellular localization and/or substrate recognition of the encoded protein. More than 24 sequence variations have been reported. The most studied C421A (rs2231142) nucleotide change, results in a glutamine-to-lysine substitution in the translated protein (pQ141K). Among the studies of SNPs in the ABCG2 gene, two included CML patients treated with imatinib [20, 26]. The first showed that the homozygous GG genotype of rs2231137 in ABCG2 in advanced stage CML patients was significantly associated with poor major or complete cytogenetic response[26], although this result was not subsequently validated in an independent cohort 20.
We were able to test the association between ABCG2 haplotype G-G and 1772 other ABCG2-related SNPs including rs2231137 and rs2231142 (not represented in our DNA chip) by means of an open-access database. We found that rs2231135, which is a 5’UTR and is potentially implicated in ABCG2 expression, was associated with haplotype G-G of ABCG2. However, the statistical association between ABCG2 polymorphisms and CI-MMR does not necessary imply a causal relationship and eventual changes in ABCG2 expression linked to these polymorphisms will have to be addressed in further studies.
The SNP rs609468 from SLC22A1 (also known as OCTN1 or HOCT1 and involved in imatinib uptake) had the lowest p-value in our exploratory cohort (SLEC). SLC22A1 has previously been studied in relation to imatinib response. The SNP rs683369 and advanced disease stage correlated with a high rate of loss of cytogenetic response or treatment failure to imatinib [26], whereas a polymorphism in rs1050152 was significantly associated with MMR [20]. SLC22A1 activity was found predictive of MMR and correlated with overall and event-free survival, especially in patients receiving less than 600 mg/d of imatinib daily [39]. Although the hypothesis that changes in SLC22A1 sequence may result in changes of activity affecting imatinib bioavailability is particularly attractive, more recent studies have failed to demonstrate association between SLC22A1 SNPs and imatinib response [27, 40]. In the same way, SNP rs609468 identified in the SLEC, was not validated in the SVC in our study.
Finally, only 3 SNPs out of 12 were validated. This result is in accordance with the FDR level selected in our analysis. Interestingly no SNPs from our chip located in the ABCG1 gene were found to be associated with imatinib response in our analysis.
Pharmacological studies have suggested that imatinib trough levels may mediate molecular response [10, 12], and it is thus of interest to identify if this is the case for the observed effect of ABCG2 haplotype on molecular response (as is the dose effect). This question will be addressed in patients included in the OPTIM-imatinib clinical trial, an ongoing prospective clinical trial evaluating imatinib dose adjustment driven by imatinib trough levels (OPTIM-Imatinib, EudraCT number 2010-019568-35).
In conclusion, our results demonstrate the influence of a constitutive ABCG2 haplotype on the response to imatinib in CP-CML patients and raise the possibility of personalizing imatinib daily doses in this population on the basis of constitutive genotyping.
PATIENTS AND METHODS
Study design
This study was approved by the Human Ethics Committee of the St Louis Hospital, Paris. Written informed consent was obtained from all patients prior to study participation.
Analyses were performed in two independent patient cohorts; the Saint Louis exploratory cohort (SLEC) treated at the Saint Louis hospital specialized clinical trial center (CIC), and the SPIRIT validation cohort (SVC) treated at participating centers in the SPIRIT trial [36] (clinicaltrials.gov: NCT00219739). Data were collected at participating institutions, analyzed using the sponsor’s data management systems. Access to primary clinical data was available to all authors.
Patients and assessments
The SLEC included 105 consecutively referred CP-CML patients enrolled at the CIC between 2006 and 2009 and treated with imatinib 400 mg/d. The SVC included 239 CP-CML patients from the prospective SPIRIT trial based on sample availability from patients recruited to the imatinib arms; 132 patients were treated with 400 mg/d and 107 with 600 mg/d. Patients receiving imatinib plus pegylated interferon-alpha2b or imatinib plus cytarabine were not analyzed.
Peripheral blood samples for DNA extraction were collected at the time of recruitment. BCR-ABL transcripts were quantified by RTQ-PCR every 3 months in accordance with international recommendations, and expressed according to the international scale (IS) as a BCR-ABL/ABL standardized ratio (BCR-ABLIS) [41]. MMR was defined as a BCR-ABLIS ratio ≤0.1%).
Genotypes from 76 unrelated and unaffected individuals obtained from the CEU population (Utah residents with northern and western European ancestry) from the CEPH (“Centre d’Etudes du Polymorphisme Humain”) database were downloaded from the 1000 Genomes Project website [42].
SNP selection and genotyping
A dedicated DNA chip[34] designed in 2006 by the French REPAC network (coordinated by Pierre Laurent-Puig and Fabien Calvo, Supplementary Table ST1) was used for patient genotyping. Among 16 561 SNPs on the chip, 857 covering 94 drug transporter genes were selected. Genotyping was performed by Integragen SA using the Illumina GoldenGate assay. A list of variations from the ABCG2 gene was downloaded from the 1000 Genomes Project website [34]. All 16 561 SNPs genotyped in the 105 SLEC patients and the 239 SVC patients were included in the quality control process. Individuals with a call rate below 90%, SNPs with minor allele frequency below 10%, and SNPs with a call rate below 90% were excluded.
Statistical analysis
Patient characteristics were compared between cohorts using Chi-squared or Wilcoxon tests. Sample size simulations show that for conventional type 1 and 2 error rates, in a population of about one hundred with approximately 60% of patients expected to reach MMR within the first 18 months and with a regression coefficient of two between groups, SNPs differentiating more than one-third of patients are required [44]. This result led us to investigate those SNPs discriminating at least one third of the patients in a recessive mode.
CI-MMR at 18 months was analyzed in the various patient cohorts (SLEC/SVC, and by imatinib dose) using the Fine and Gray regression model with multivariate and univariate analyses. Adverse events, toxicities or deaths not related to CML which led to loss of molecular follow-up were handled as competing events. An SNP association analysis for CI-MMR at 18 months was also performed using the Fine and Gray model. Markers with a false discovery rate (FDR) < 50% in the SLEC population were investigated in the validation cohort (overall, 400 mg/d and 600 mg/d) using a significance cut-off of P = 0.05. The Benjamini and Hochberg method was used for multiple testing issues [45]. Haplotype frequencies were estimated in the SLEC, SVC (overall, 400 mg/d and 600 mg/d) and CEU populations using the classic EM algorithm on unrelated individuals implemented in the Haplo.stats R library [46-48]. Homogeneity in haplotypic distribution between populations was tested. An association analysis between haplotype or Sokal score with CI-MMR at 18-months was performed using a Fine and Gray model. The association between early molecular response (BCR-ABLIS ≤ 10% at 3 months) and responses of interest (BCR-ABLIS ≤ 1% at 12 months and BCR-ABLIS ≤ 0.1% at 18 months) and ABCG2 haplotypes were tested using the chi-squared test. Data were analyzed using R Project for Statistical Computing software (R version 2.15.2) [49].
Supplementary information is available on the Oncotarget website.
ACKNOWLEDGMENTS
We thank Pr Pierre Laurent-Puig for REPAC network coordination, Dr Christophe Blondel for his contribution to SNP selection and validation, Magali Nacfer for logistical assistance, the FRENCH-CML Group (FI-LMC), Pr Jean Jacques Kiladjian, Dr Delphine Rea, Dr Odile Maarek, and all SPIRIT investigators for patient recruitment, Dr Maud Vanpeene and Dr Mélanie Letexier for technical assistance, Dr Anne Marfaing, Dr Eric Delabesse and Dr Marc Spentchian who contributed to DNA sample collection, Dr Sarah Zohar for assistance in ERB submission and Dr Sarah MacKenzie (funded by Intergroup pour la Léucemie Myeloïde Chronique) for manuscript correction. This work was supported by INSERM (Pharmacogenetic-REPAC Network), by the Grant U03S03 from the ECOS-Sud program (France-Uruguay), a Grant from the Association Jean Bernard, France and a grant from the French Ministry of Health (Programme Hospitalier de Recherche Clinique (PHRC 2011, 11N28), SPIRIT ClinicalTrials.gov Identifier: NCT00219739. PR received research grants from BMS and Novartis. JMC performs consultancy activity for Novartis.
AUTHORSHIP
Contributions:
HBG, PR, MD and FC designed the study. HBG coordinated the study. PR contributed the majority of patients and clinical expertise. HBG and PR performed patient inclusion procedures and clinical follow-up, and collected clinical and biological data. MD performed bioinformatics and statistical analysis. FC coordinated the DNA chip design. FG coordinated the French SPIRIT trial. JMC and DG performed molecular analyses. PL performed DNA extraction. FS and EG interpreted and discussed data. ER contributed patients and clinical data. CP, JG, FG contributed DNA samples, biological and clinical data from the validation cohort. JG and EG contributed with methodological expertise. HBG, MD and PR analyzed and interpreted data, participated in discussions and wrote the manuscript. All the authors read and approved the final manuscript.
References
1. Hochhaus A, O’Brien SG, Guilhot F, Druker BJ, Branford S, Foroni L, Goldman JM, Müller MC, Radich JP, Rudoltz M, Mone M, Gathmann I, Hughes TP, Larson RA. Six-year follow-up of patients receiving imatinib for the first-line treatment of chronic myeloid leukemia. Macmillan Publishers Limited; 2009:1054–1061. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19282833.
2. Kantarjian H, Shah NP, Hochhaus A, Cortes J, Shah S, Ayala M, Moiraghi B, Shen Z, Mayer J, Pasquini R, Nakamae H, Huguet F, Boqué C, Chuah C, Bleickardt E, Bradley-Garelik MB, Zhu C, Szatrowski T, Shapiro D, Baccarani M. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. The New England Journal of Medicine. 2010;362(24):2260–2270.
3. Saglio G, Kim D-W, Issaragrisil S, Le Coutre P, Etienne G, Lobo C, Pasquini R, Clark RE, Hochhaus A, Hughes TP, Gallagher N, Hoenekopp A, Dong M, Haque A, Larson RA, Kantarjian HM. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. The New England Journal of Medicine. 2010;362(24):2251–2259.
4. Aichberger KJ, Herndlhofer S, Schernthaner G-H, Schillinger M, Mitterbauer-Hohendanner G, Sillaber C, Valent P. Progressive peripheral arterial occlusive disease and other vascular events during nilotinib therapy in CML. American Journal of Hematology. 2011;86(7):1–7.
5. Montani D, Bergot E, Gunther S, Savale L, Bergeron A, Bourdin A, Bouvaist H, Canuet M, Pison C, Macro M, Poubeau P, Girerd B, Natali D, Guignabert C, Perros F, O’Callaghan DS, Jais X, Tubert-Bitter P, Zalcman G, Sitbon O, Simonneau G, Humbert M. Pulmonary Arterial Hypertension in Patients Treated by Dasatinib. Circulation. 2012;125(17):2128–37.
6. Kantarjian HM, O’Brien S, Cortes J, Giles FJ, Rios MB, Shan J, Faderl S, Garcia-Manero G, Ferrajoli A, Verstovsek S, Wierda W, Keating M, Talpaz M. Imatinib Mesylate Therapy Improves Survival in Patients with Newly Diagnosed Philadelphia Chromosome-Positive Chronic Myelogenous Leukemia in the Chronic Phase. Cancer. 2003;98:2636–2642.
7. Kantarjian HM, Hochhaus A, Saglio G, Souza C De, Flinn IW, Stenke L, Goh Y-T, Rosti G, Nakamae H, Gallagher NJ, Hoenekopp A, Blakesley RE, Larson RA, Hughes TP. Nilotinib versus imatinib for the treatment of patients with newly diagnosed chronic phase, Philadelphia chromosome-positive, chronic myeloid leukaemia: 24-month minimum follow-up of the phase 3 randomised ENESTnd trial. The lancet oncology. 2011;12(9):841–851.
8. Kantarjian HM, Shah NP, Cortes JE, Baccarani M, Agarwal MB, Undurraga MS, Wang J, Kassack Ipiña JJ, Kim D-W, Ogura M, Pavlovsky C, Junghanss C, Milone JH, Nicolini FE, Robak T, Van Droogenbroeck J, Vellenga E, Bradley-Garelik MB, Zhu C, Hochhaus A. Dasatinib or imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: 2-year follow-up from a randomized phase 3 trial (DASISION). Blood. 2012;119(5):1123–9.
9. Chomel J, Turhan AG. Chronic myeloid leukemia stem cells in the era of targeted therapies: resistance, persistence and long-term dormancy. Oncotarget. 2011;2(9):713–27.
10. Larson RA, Druker BJ, Guilhot F, O’Brien SG, Riviere GJ, Krahnke T, Gathmann I, Wang Y. Imatinib pharmacokinetics and its correlation with response and safety in chronic-phase chronic myeloid leukemia: a subanalysis of the IRIS study. Blood. 2008;111(8):4022–4028.
11. Marin D, Bazeos A, Mahon F-X, Eliasson L, Milojkovic D, Bua M, Apperley JF, Szydlo R, Desai R, Kozlowski K, Paliompeis C, Latham V, Foroni L, Molimard M, Reid A, Rezvani K, de Lavallade H, Guallar C, Goldman J, Khorashad JS. Adherence is the critical factor for achieving molecular responses in patients with chronic myeloid leukemia who achieve complete cytogenetic responses on imatinib. Journal of clinical oncology. 2010;28(14):2381–2388.
12. Picard S, Titier K, Etienne G, Teilhet E, Ducint D, Bernard M-A, Lassalle R, Marit G, Reiffers J, Begaud B, Moore N, Molimard M, Mahon F-X. Trough imatinib plasma levels are associated with both cytogenetic and molecular responses to standard-dose imatinib in chronic myeloid leukemia. Blood. 2007;109(8):3496–3499.
13. Chen H-C, Hu W-X, Liu Q-X, Li W-K, Chen F-Z, Rao Z-Z, Liu X-F, Luo Y-P, Cao Y-F. Genetic polymorphisms of metabolic enzymes CYP1A1, CYP2D6, GSTM1 and GSTT1 and leukemia susceptibility. European journal of cancer prevention. 2008;17(3):251–258.
14. Kim DHD, Xu W, Ma C, Liu X, Siminovitch K, Messner HA, Lipton JH. Genetic variants in the candidate genes of the apoptosis pathway and susceptibility to chronic myeloid leukemia. Blood. 2009;113(11):2517–2525.
15. Taspinar M, Aydos SE, Comez O, Elhan AH, Karabulut HG, Sunguroglu A. CYP1A1, GST gene polymorphisms and risk of chronic myeloid leukemia. Swiss medical weekly. 2008;138(1-2):12–17.
16. Zhang Y, Wang B, Ye S, Liu S, Liu M, Shen C, Teng Y, Qi J. Killer cell immunoglobulin-like receptor gene polymorphisms in patients with leukemia: possible association with susceptibility to the disease. Leukemia research. 2010;34(1):55–58.
17. Boultwood J, Perry J, Zaman R, Fernandez-Santamaria C, Littlewood T, Kusec R, Pellagatti A, Wang L, Clark RE, Wainscoat JS. High-density single nucleotide polymorphism array analysis and ASXL1 gene mutation screening in chronic myeloid leukemia during disease progression. Leukemia. 2010;24(6):1139–1145.
18. Zhang S-J, Shi J-Y, Li J-Y. GATA-2 L359 V mutation is exclusively associated with CML progression but not other hematological malignancies and GATA-2 P250A is a novel single nucleotide polymorphism. Leukemia research. 2009;33(8):1141–1143.
19. Nambu T, Hamada A, Nakashima R, Yuki M, Kawaguchi T, Mitsuya H, Saito H. Association of SLCO1B3 polymorphism with intracellular accumulation of imatinib in leukocytes in patients with chronic myeloid leukemia. Biological & pharmaceutical bulletin. 2011;34(1):114–119.
20. Angelini S, Soverini S, Ravegnini G, Barnett M, Turrini E, Thornquist M, Pane F, Hughes TP, White DL, Radich J, Kim D-W, Saglio G, Cilloni D, Iacobucci I, Perini G, Woodman R, Cantelli-Forti G, Baccarani M, Hrelia P, Martinelli G. Association between imatinib transporters and metabolizing enzymes genotype and response in newly diagnosed chronic myeloid leukemia patients receiving imatinib therapy. Haematologica. 2013;98(2):193–200.
21. Crossman LC, O’Hare T, Lange T, Willis SG, Stoffregen EP, Corbin AS, O’Brien SG, Heinrich MC, Druker BJ, Middleton PG, Deininger MWN. A single nucleotide polymorphism in the coding region of ABL and its effects on sensitivity to imatinib. Leukemia. 2005;19(11):1859–1862.
22. Dulucq S, Bouchet S, Turcq B, Lippert E, Etienne G, Reiffers J, Molimard M, Krajinovic M, Mahon F-X. Multidrug resistance gene (MDR1) polymorphisms are associated with major molecular responses to standard-dose imatinib in chronic myeloid leukemia. Blood. 2008;112(5):2024–2027.
23. Guillem VM, Cervantes F, Martínez J, Alvarez-Larrán A, Collado M, Camós M, Sureda A, Maffioli M, Marugán I, Hernández-Boluda J-C. XPC genetic polymorphisms correlate with the response to imatinib treatment in patients with chronic phase chronic myeloid leukemia. American journal of hematology. 2010;85(7):482–486.
24. Kim DH, Xu W, Kamel-Reid S, Liu X, Jung CW, Kim S, Lipton JH. Clinical relevance of vascular endothelial growth factor (VEGFA) and VEGF receptor (VEGFR2) gene polymorphism on the treatment outcome following imatinib therapy. Annals of oncology. 2010;21(6):1179–1188.
25. Kim DHD, Kong JH, Byeun JY, Jung CW, Xu W, Liu X, Kamel-Reid S, Kim Y-K, Kim H-J, Lipton JH. The IFNG (IFN-gamma) genotype predicts cytogenetic and molecular response to imatinib therapy in chronic myeloid leukemia. Clinical cancer research. 2010;16(21):5339–5350.
26. Kim DHD, Sriharsha L, Xu W, Kamel-Reid S, Liu X, Siminovitch K, Messner HA, Lipton JH. Clinical relevance of a pharmacogenetic approach using multiple candidate genes to predict response and resistance to imatinib therapy in chronic myeloid leukemia. Clinical cancer research. 2009;15(14):4750–4758.
27. Maffioli M, Camós M, Gaya A, Hernández-Boluda J-C, Alvarez-Larrán A, Domingo A, Granell M, Guillem V, Vallansot R, Costa D, Bellosillo B, Colomer D, Cervantes F. Correlation between genetic polymorphisms of the hOCT1 and MDR1 genes and the response to imatinib in patients newly diagnosed with chronic-phase chronic myeloid leukemia. Leukemia Research. 2011;35(8):1014–1019.
28. Ni L-N, Li J-Y, Miao K-R, Qiao C, Zhang S-J, Qiu H-R, Qian S-X. Multidrug resistance gene (MDR1) polymorphisms correlate with imatinib response in chronic myeloid leukemia. Medical oncology. 2011;28(1):265–269.
29. Deenik W, van der Holt B, Janssen JJWM, Chu IWT, Valk PJM, Ossenkoppele GJ, van der Heiden IP, Sonneveld P, van Schaik RHN, Cornelissen JJ. Polymorphisms in the multidrug resistance gene MDR1 (ABCB1) predict for molecular resistance in patients with newly diagnosed chronic myeloid leukemia receiving high-dose imatinib. Blood. 2010;116(26):6144–6146. .
30. Dulucq S, Preudhomme C, Guilhot F, Mahon F-X. Response: is there really a relationship between Multidrug Resistance Gene (MDR1) polymorphisms and major molecular response to imatinib in chronic myeloid leukemia? Blood. 2010;116(26):6145–6146.
31. Giles FJ, Rosti G, Beris P, Clark RE, Le Coutre P, Mahon F-X, Steegmann J-L, Valent P, Saglio G. Nilotinib is superior to imatinib as first-line therapy of chronic myeloid leukemia: the ENESTnd study. Expert review of hematology. 2010;3(6):665–673.
32. Baccarani M, Cortes J, Pane F, Niederwieser D, Saglio G, Apperley J, Cervantes F, Deininger M, Gratwohl A, Guilhot F, Hochhaus A, Horowitz M, Hughes T, Kantarjian H, Larson R, Radich J, Simonsson B, Silver RT, Goldman J, Hehlmann R. Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. Journal of clinical oncology official journal of the American Society of Clinical Oncology. 2009;27(35):6041–6051.
33. Simon RM, Paik S, Hayes DF. Use of archived specimens in evaluation of prognostic and predictive biomarkers. Journal of the National Cancer Institute. 2009;101(21):1446–52.
34. Ahmed I, Tamouza R, Delord M, Krishnamoorthy R, Tzourio C, Mulot C, Nacfer M, Lambert J-C, Beaune P, Laurent-Puig P, Loriot M-A, Charron D, Elbaz A. Association between Parkinson’s disease and the HLA-DRB1 locus. Movement disorders. 2012;27(9):1104–10. .
35. Hehlmann R, Lauseker M, Jung-Munkwitz S, Leitner A, Müller MC, Pletsch N, Proetel U, Haferlach C, Schlegelberger B, Balleisen L, Hänel M, Pfirrmann M, Krause SW, Nerl C, Pralle H, Gratwohl A, Hossfeld DK, Hasford J, Hochhaus A, Saussele S. Tolerability-adapted imatinib 800 mg/d versus 400 mg/d versus 400 mg/d plus interferon-α in newly diagnosed chronic myeloid leukemia. Journal of clinical oncology. 2011;29(12):1634–1642.
36. Preudhomme C, Guilhot J, Nicolini FE, Guerci-Bresler A, Rigal-Huguet F, Maloisel F, Coiteux V, Gardembas M, Berthou C, Vekhoff A, Rea D, Jourdan E, Allard C, Delmer A, Rousselot P, Legros L, Berger M, Corm S, Etienne G, Roche-Lestienne C, Eclache V, Mahon F-X, Guilhot F. Imatinib plus peginterferon alfa-2a in chronic myeloid leukemia. The New England journal of medicine. 2010;363(26):2511–2521.
37. Ieiri I. Functional significance of genetic polymorphisms in P-glycoprotein (MDR1, ABCB1) and breast cancer resistance protein (BCRP, ABCG2). Drug metabolism and pharmacokinetics. Int J Biochem Mol Biol. 2012;27(1):85–105.
38. Mo W, Zhang J-T. Human ABCG2: structure, function, and its role in multidrug resistance. International journal of biochemistry and molecular biology. 2012;3(1):1–27.
39. White DL, Dang P, Engler J, Frede A, Zrim S, Osborn M, Saunders VA, Manley PW, Hughes TP. Functional activity of the OCT-1 protein is predictive of long-term outcome in patients with chronic-phase chronic myeloid leukemia treated with imatinib. J Clin Oncol. 2010; 28:2761–2767.
40. White, D.L. Saunders, V.A. Dang, P. Engler, J. Hughes TP. OCT-1 activity measurement provides a superior imatinib response predictor than screening for single-nucleotide polymorphisms of OCT-1. Leukemia. 2010;24(11):1962–1965.
41. Hughes T, Deininger M, Hochhaus A, Branford S, Radich J, Kaeda J, Baccarani M, Cortes J, Cross NCP, Druker BJ, Gabert J, Grimwade D, Hehlmann R, Kamel-Reid S, Lipton JH, Longtine J, Martinelli G, Saglio G, Soverini S, Stock W, Goldman JM. Monitoring CML patients responding to treatment with tyrosine kinase inhibitors: review and recommendations for harmonizing current methodology for detecting BCR-ABL transcripts and kinase domain mutations and for expressing results. Blood. 2006;108(1):28–37.
42. Site 1000 Genomes Project ftp. Ftp://ftp.1000genomes.ebi.ac.uk/. Available at: ftp://ftp.1000genomes.ebi.ac.uk/.
43. http://www.1000genomes.org/.
44. Latouche A, Porcher R, Chevret S. Sample size formula for proportional hazards modelling of competing risks. Statistics in Medicine. 2004;23(21):3263–3274.
45. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society Series B Methodological. 1995;57(1):289–300.
46. Schaid DJ, Rowland CM, Tines DE, Jacobson RM, Poland GA. Score Tests for Association between Traits and Haplotypes when Linkage Phase Is Ambiguous. American journal of human genetics. 2002;70(2):425–434.
47. Sinnwell JP SD. Haplo.stats: Statistical Analysis of Haplotypes with Traits and Covariates when Linkage Phase is Ambiguous. R package version 1.4.4.
48. Site SG and GEMC. http://mayoresearch.mayo.edu/mayo/research/schaid_lab/. Available at: http://mayoresearch.mayo.edu/mayo/research/schaid_lab/software.cfm).
49. González, Juan R; Armengol, Lluís; Guinó, Elisabet; Solé, Xavier; Moreno V. http://cran.r-project.org/web/packages/SNPassoc/index.html.