
INTRODUCTION
Age-related macular degeneration (AMD) is a heterogeneous clinical condition in which retinal degeneration occurs predominantly in the macula and leads to impairment of central visual acuity [1, 2]. AMD, the leading cause of blindness in people aged 55 years or older in developed countries, occurs in two general forms: 1) Wet AMD involving choroidal neovascularization with subsequent bleeding and fluid exudation; 2) Dry AMD, which involves a constellation of clinical features that can include: drusen, pigment clumping, abnormalities of the retinal pigment epithelium (RPE), and geographic atrophy (GA) [1-3]. The latter can begin as a thinning of the RPE and lead subsequently to an atrophic change in the macula with loss of overlying photoreceptors [2-4]. As a result, there is a reduction of best corrected visual acuity (BCVA), retinal sensitivity, retinal bioelectric activity, and then damage to visual performance (VP). Nowadays, spectral domain-optical coherence tomography (SD-OCT) has been added to electroretinographic exams on retina for more accurate morphological and functional studies [5].
Moreover, dry AMD accounts for 80% of all intermediate and advanced forms of the retinal disease and no effective treatment for progressive vision loss is available to date. On the other hand, the retina is particularly susceptible to oxidative damage due to its high oxygen demand and constant exposure to light. It is known that smoking may slow down choroidal blood flow, promoting ischemia, hypoxia, and microinfarctions, resulting in a reduction in macular pigments and in RPE damage. Oral supplement of antioxidants and smoking cessation can help to prevent or counter AMD development and progression [1-3]. However, dry AMD progression reduces VP causing discomfort to patients who become increasingly more visually impaired [3-4].
Consequently, the idea of using systemic or local injection of stem/progenitor or reparatory cells in the area of injury to treat multiple chronic disorders has received close attention in the last decade [6]. Unfortunately, the appropriate surgical procedure to graft cells in the subretinal space appears to be very complex and expensive, as well as potentially dangerous for the eye, as it undergoes invasive surgery. Instead, embryonic stem cells are not always ethically acceptable and not entirely free from the risks related to the use of immunosuppressive therapy [7].
Nevertheless, there is another aspect linked to the properties of growth factors (GFs) which have been known for many years and specifically to their ability to curb the evolution of retinal dystrophies in experimental models, as demonstrated by several studies. GFs and neurotrophins such as basic fibroblast growth factor (bFGF), neural growth factor (NGF), ciliar neurotrophic factor (CNTF) and brain-derived neurotrophic factor (BDNF), can significantly slow down retinal degeneration and cell death in animal models [7-10].
Based on these concepts, the efficacy of autologous fat transplantation was demonstrated by Filatov [11] work and Pelaez [12] first, and by Meduri et al. [13] and Limoli et al. later [14].
Our cellular autograft, defined Limoli Retinal Restoration Technique (LRRT), uses three different cell types that are able to produce adequate GFs in terms of both quantity and quality:
Adipose stromal cells derived from orbital fat [15].
Platelets (PLT) derived from platelet-rich plasma (PRP) [16, 17].
Adipose-derived stem cells (ADSCs) included in the stromal-vascular fraction (SVF) of adipose tissue [18].
Cellular autograft efficacy in dry AMD was demonstrated by Limoli et al. in preliminary works [4, 19-21]. Indeed, to curb the worsening of retinal dry AMD, we considered employing two important elements:
neurotrophic GFs to slow down RPE cells and photoreceptor apoptosis;
angiotrophic GFs for therapeutic purposes to improve choroidal flow; in fact, the impairment of the latter is belived to be one of the pathogenetic factors of AMD.
Consequently, the rationale of our study was focused on cell therapy, through autologous cells surgically grafted in the suprachoroidal space, in order to achieve a costant production of GFs at the chorioretinal level. Besides, to evaluate the prognosis of dry AMD patients treated with LRRT, we assumed that a greater number of residual cells leads to greater interaction between GFs and chorioretinal cellular membrane receptors, more intense cellular activity and, ultimately, improvement of VP. In other words, we hypothesized that if retina is thinner and more atrophic, it is harder to obtain functional neuroenhancement through cell therapy. In order to focus on this latter aspect of our research, we chose SD-OCT for the preliminary analysis of retinal thickness average (RTA) in cell therapy with LRRT on patients affected by dry AMD.
RESULTS
In the study we included 36 eyes (21 right and 15 left eyes) of 25 patients with dry AMD (9 men and 16 women), aged between 64 and 84 years of age (75.96 years on average) (SD ±6.13) (Table 1). Prior to cell autograft with LRRT, values of RTA and all components of ERG were recorded at time 0 (T0).
Based on RTA, all the eyes were divided into two groups according to normative data for macular thickness by high-definition SD-OCT (Table 1): [5]
- Group A, where RTA was less than 250 microns (µm), with 14 eyes, 10 patients (2 men and 8 women), mean age of 77.6 years (range 64-84 years of age, SD ±6.6) (Figure 1, left panel).
- Group B, where RTA was equal to or greater than 250 µm, with 22 eyes, 15 patients (7 men and 8 women), mean age of 74.87 years (range 64-84 years of age, SD ±5.8) (Figure 1, right panel).
Table 1: Baseline demographic and clinical characteristics by retinal thickness average (RTA) in patient group A (RTA<250 microns) and group B (RTA ≥250 microns).
Patient data
Group A
Group B
Total
Number of patients (N)
N = 10
N = 15
N = 25
Female (%)
8 (80.0)
8 (53.3)
16 (64.0)
Male (%)
2 (20.0)
7 (46.7)
9 (36.0)
Number of eyes (right/left)
14 (8/6)
22 (13/9)
36 (21/15)
Average age (±SD)
77.6 (6.6)
74.87 (5.8)
76.0 (6.13)
No significant differences were found between the two groups either in terms of age (p = 0.284) or gender (p = 0.174) distribution.
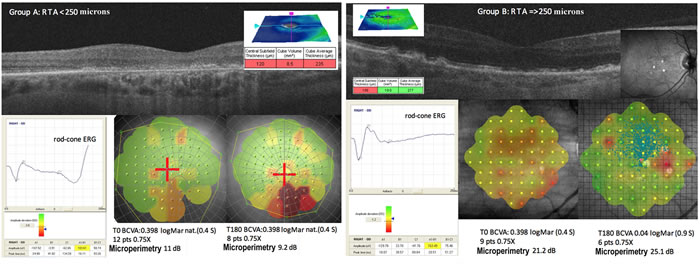
Figure 1: The level of scotopic (rod-cone or maximal) electroretinogram (ERG) is different in A and B groups depending on retinal thickness. Case report of group A (left panel). The retinal thickness average (RTA) measured by optical coherence tomography (OCT) is very low (235 microns). At 180 days post surgery we obtained a slight improvement in close-up visus. Case report of group B (right panel). The RTA is good (277 microns) and the various cell layers are well represented in the OCT. At 180 days post surgery we obtained a good improvement of best corrected visual acuity (BCVA) and close-up visus (in logMAR and Pts respectively) without magnification change. Also the sensitivity recorded with microperimetry (MY) increased in the areas with good cellularity.
Correlation with retinal thickness average (RTA) and electroretinogram (ERG)
ERG-recorded electrical activity (T0) in group A (Rod ERG = 38.1, Rod-cone ERG = 95.97, Cone ERG = 40.66) was lower than in group B (Rod ERG = 63.54, Rod-cone ERG = 131.54, Cone ERG = 47.37) (Figure 2). RTA was positive correlated with Rod-cone ERG in group A (r = 0.59, p = 0.025), but not in group B (r = -0.29, p = 0.196). RTA was positive correlated with Rod ERG in group A (r = 0.69, p = 0.006) and group B (r = 0.53, p = 0.011). (Figure 2).
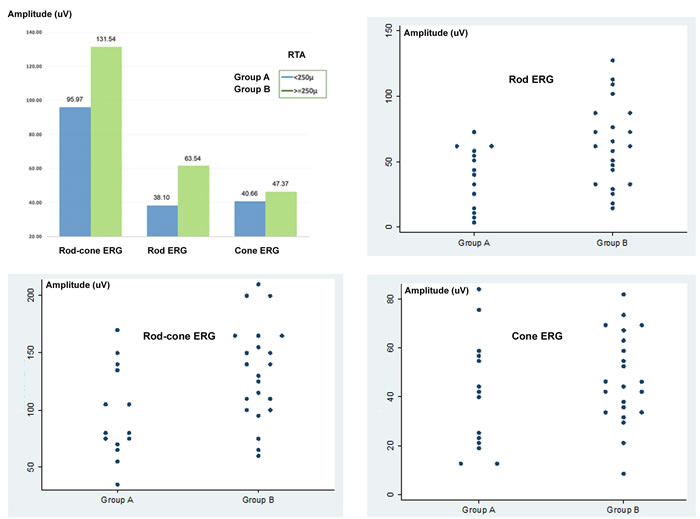
Figure 2: Electroretinogram (ERG) and retinal thickness average (RTA) in dry age-related macular degeneration (AMD) at time 0 (T0). Correlation between RTA and electrical activity (in µVolts) appears to be highly significant in relation to scotopic ERG: rod-cone or maximal ERG in group A (p = 0.025) and rod ERG in groups A (p = 0.006) and B (p = 0.011). Corresponding scatter plot graph.
Visual functional characteristics and patient compliance analysis (PCA)
The visual functional characteristics in patients with dry AMD and the average values recorded before (T0) and 6 months (T180) after cell autograft by LRRT are shown in Table 2. BCVA was measured by early treatment diabetic retinopathy study (ETDRS) charts at 4 meters in logarithm of the minimum angle of resolution (logMAR) units and visual acuity for near vision (close-up) in points (Pts) indicating the necessary zoom factor (X).
BCVA increased in group A from 0.621 logMAR to 0.588 logMAR and in group B from 0.59 logMAR to 0.41 logMAR. Mean variation was significantly lower in A (0.033 logMAR SD 0.17) than in B (0.18 logMAR SD 0.23) (Figure 1, 3A, 4) (Table 2).
Close-up visus evaluated with magnifying system increased in both groups from T0 to T180. In group A, it went from 12.14 to 8.86 Pts with the same magnification (X 5.1) and a mean increase of 3.29 Pts (SD 7.35). In group B, visual acuity went from 8.68 to 8.27 Pts with slightly lower magnification (from 3.1 to 2.9 X), equivalent to an increase of 0.41 Pts (SD 2.0) (Figure 1, 3B, and 4) (Table 2).
Average retinal sensitivity with microperimetry (MY) increased in both groups. The mean improvement in retinal sensitivity was 0.76 dB (SD 2.5), increasing from 7.65 dB to 8.41 dB in group A, and 1.59 dB (SD 3.34), increasing from 16.82 dB to 18.4 in group B (Figure 1, 3C, and 4) (Table 2).
Patient compliance analysis (PCA) showed that, at 6 months post surgery, 19 out of 36 eyes (52.78%) recorded better vision, 14 out of 36 (38.89%) no change in the functional situation, and 3 out of 36 (8.33%) a worsening (Table 3). Among the 19 eyes of the patients who noted an improvement at 6 months post surgery, 5 (26.3%) belonged to group A and 14 (73.7%) to group B.
No adverse effects were reported in any case and mean values of the intraocular pressure recorded before and after surgery did not change significantly.
Table 2: Mean values recorded before (T0) and 6 months (T180) after surgery with Limoli Retinal Restoration Technique (LRRT) for retinal thickness average (RTA) of group A (RTA<250 microns) and group B (RTA ≥250 microns) and statistical significance.
Parameter |
Group A |
P value* |
Group B |
P value* |
|||||||
T0 |
T180 |
T0 |
T180 |
||||||||
Mean (SD) |
Mean (SD) |
||||||||||
BCVA (logMAR) |
0.62 (0.57) |
0.58 (0.56) |
0.465 |
0.59 (0.39) |
0.41 (0.3) |
0.001 |
|||||
Close-up visus (Pts) |
12.14 (12.3) |
8.86 (5.36) |
0.083 |
8.68 (2.87) |
8.27 (3.33) |
0.33 |
|||||
Close-up visus X |
5.13 (4.44) |
5.13 (4.08) |
1.000 |
3.11 (3.39) |
2.92 (3.48) |
0.03 |
|||||
Retinal sensitivity |
7.65 (4.83) |
8.41 (4.75) |
0.237 |
16.82 (3.2) |
18.4 (3.4) |
0.01 |
|||||
Parameter |
Group A |
Group B |
P value* |
||||||||
Mean changes (SD) |
% |
Mean changes (SD) |
% |
||||||||
BCVA (logMAR) |
0.033 (0.17) |
5.16% |
0.18 (0.23) |
30.51% |
0.04 |
||||||
Close-up visus (Pts) |
3.29 (7.35) |
27.10% |
0.41 (2.02) |
4.72% |
0.09 |
||||||
Close-up visus X |
0 (1.95) |
0% |
0.19 (0.49) |
6.10% |
0.43 |
||||||
Retinal sensitivity |
0.76 (2.51) |
9.93% |
1.59 (3.34) |
9.45% |
0.50 |
||||||
* Calculated by Mixed regression model taking into account multiple eyes for the same subjects. BCVA= best corrected visual acuity for far distance measured by early treatment diabetic retinopathy study (ETDRS) charts at 4 meters in logarithm of the minimum angle of resolution (logMAR) units; close-up visus = visual acuity for near vision in points (Pts) measured by magnifying system and necessary magnification, X = necessary magnification; Retinal sensitivity = measured by microperimetry (MY) in decibel (dB); SD = standard deviation.
Table 3: Patient compliance analysis (PCA) shows that, at 6 months post surgery, 19 of 36 eyes (52.78%) recorded better vision, 14 (38.89%) no change in functional situation, and 3 (8.33%) a worsening.
PCA |
Group A |
Group B |
Total |
Number of eyes |
14 |
22 |
36 |
Improved (%) |
5 (35.71) |
14 (63.64) |
19 (52.78) |
Unchanged (%) |
7 (50) |
7 (31.82) |
14 (38.89) |
Worse (%) |
2 (14.29) |
1 (4.55) |
3 (8.33) |
Among the 19 eyes of patients who noted an improvement at 6 months post surgery, 5 (26.3%) belong to group A and 14 (73.7%) to group B.
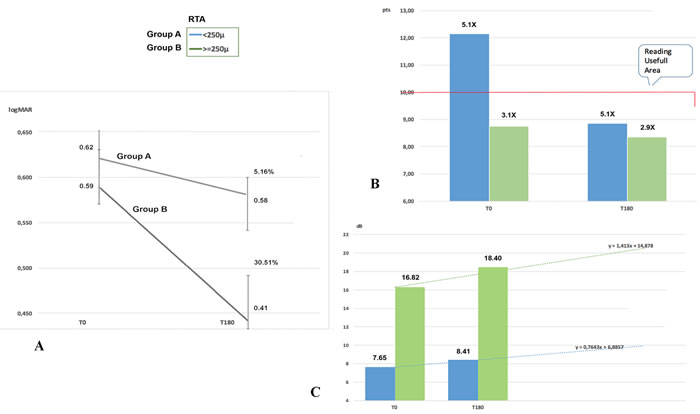
Figure 3: Values recorded from time 0 (T0) to time at 6 months (T180) after Limoli Retinal Restoration Technique (LRRT). Panel A. Best corrected visual acuity (BCVA) recorded a slight increase (5.16%) in group A and a greater increase (30.51%) in group B. Panel B. After LRRT, close-up visus (in Pts) evaluated by magnification reaches or maintains values below 10 points (Pts) in both groups. Panel C. The average retinal sensitivity (in dB) recorded by microperimetry (MY) 6 months after cellular autograft increases in both groups: +6.88% in group A and +15.23% in group B. Retinal thickness average (RTA).
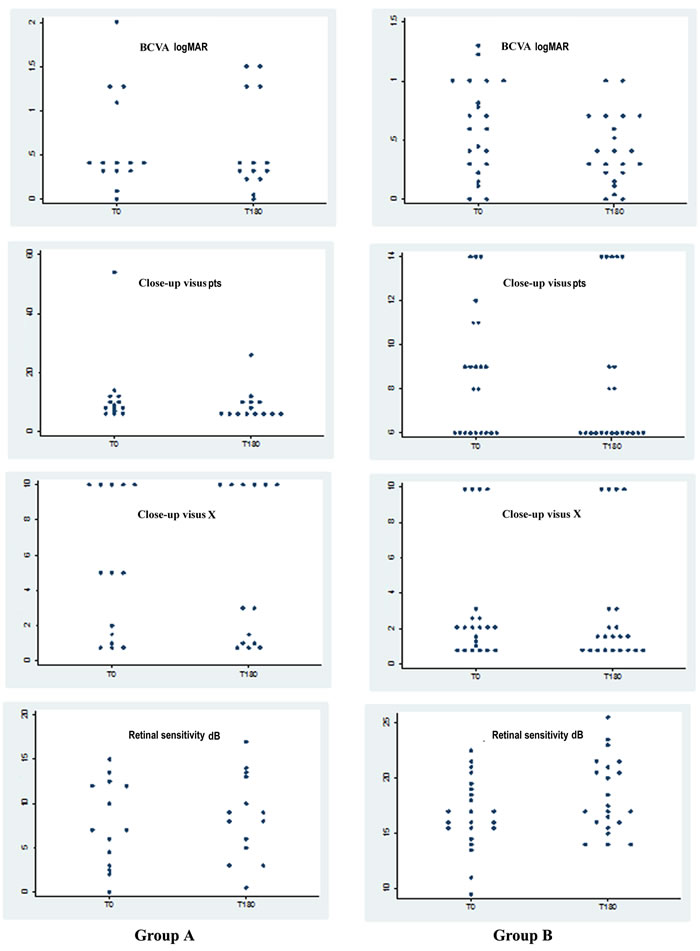
Figure 4: Corresponding scatter plot graphs of the values recorded from time 0 (T0) to time at 6 months (T180) after Limoli Retinal Restoration Technique (LRRT). Best corrected visual acuity (BCVA) (in logMAR); close-up visus (in Pts) evaluated by magnification reaches or maintains values below 10 Pts in both groups; retinal sensitivity (in dB).
DISCUSSION
We considered employing GFs for therapeutic purposes in order to improve choroidal flow, slow down RPE cells and photoreceptor apoptosis, and ultimately curb retinal worsening in dry AMD patients treated with LRRT. Moreover, we assumed that a greater number of residual cells could lead to a greater interaction between GFs and chorioretinal cellular membrane receptors, to more intense cellular activity and, ultimately, to an improvement of VP. Since GFs and neurotrophins usually have a short half-life, the promotion of retinal cell survival needs continuous and frequent administration of these factors. Their short half-life and the consequent need to perform frequent intravitreal injections with the ensuing complications have not allowed therapeutic use in humans so far [8-10].
To overcome these drawbacks, each eye of our subjects received cellular autograft according to LRRT, after the harvest of SVF with ADSCs and Platelet Rich Plasma, an innovation of Pelaez-Meduri’s intervention [4, 12, 13, 19]. They used a transplantation of autologous fat in the subscleral space, obtaining relevant but transient results [5, 19]. The goals of LRRT, that is the grafting of the suprachoroidal adipose pedicle, of ADSCs in SVF and intrapeduncolar PRP were to:
1. Promote vascular pedicle fat engraftment with the underlying choroid;
2. Enhance pedicle fat original vascularization in order to ensure its volume and survival;
3. Initiate a regenerative start-up of all the retinal elements through the secretion of paracrine GFs.
Knowing the amount of cells in the retina could be useful for both rehabilitators and surgeons in order to plan a cell therapy with an acceptable predictive power in low vision patient with dry AMD. Moreover, we observed that cone-rod ERG and rod ERG present a highly significant correlation with RTA, while cone ERG does not, since the main functional expression of fovea appears to be compromised also with still regular macular volumes in dry AMD, at least in the initial stages (Figure 2) [4, 5, 19]. Residual retinal trophism in dry AMD, value with RTA, may represent a prognostic criterion for the indication of cellular autograft with LRRT, since better outcomes are found increasingly in group B. We already saw the positive action on retinal electrical activity in our previous study, and the current study has shown that scotopic ERG, BCVA and sensitivity detected by MY appear to be more intense in thicker retinas (Table 2, Figure 2, 3, and 4) [4, 19]. On the contrary, natural evolution shows inevitable visual impairment, according to clinical events [1-3].
LRRT allows the grafting of 3 autologous components and each of the grafted elements has its own specific assets in GFs useful from a regenerative point of view.
Fat cells of the pedicle grafted and contained in the suprachoroidal space produce: basic fibroblast growth factor (bFGF), epidermal growth factor (EGF), insulin-like growth factor-1 (IGF-1), interleukin (IL), transforming growth factor-β (TGF-β), pigment-epithelium-derived factor (PEDF), and adiponectin [22].
ADSCs produce: bFGF, vascular endothelial growth factor (VEGF), macrophage colony-stimulating factor (M-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), placental growth factor (PlGF), TGF-β, hepatocyte growth factor (HGF), IGF-1, IL, and angiogenin [15].
Platelets produce: platelet-derived growth factor (PDGF), IGF-1, TGF-β, VEGF, bFGF, EGF, platelet-derived angiogenesis factor (PDAF), and thrombospondin (TSP) [23-25].
Therefore, following the complex process of GF-receptor formation, a limited number of second messengers are generated inside the target cell. These, in turn, control a series of biochemical pathways in the cell by regulating enzyme activity and transcription factors, through a cascade of phosphorylation events [19-25]. Upon reaching the cell nucleus, the signals determine changes in the response of genes, increasing the production of proteins, enzymes, and cytokine transcription which all play a role in cell trophic control, as demonstrated by the increase in scotopic ERG-recorded electrical activity [19-25].
The main function of GFs is the external control of the cell cycle from the quiescent cell phase, G0 phase, to the entry of the cell in the G1 phase of growth. In addition, they can regulate the triggering of mitosis, cell survival, migration, and cell differentiation. Some factors, such as VEGF, bFGF, angiogenin, PDAF, PlGF, PDGF, EGF, and TGF-β promote endothelial regeneration and may contribute to choriocapillaris reperfusion [16, 17, 25, 26]. VEGF, introduced with PRP, stimulates ADSC proliferation which in turn promotes both autologous fat and adipocytes survival [21, 26, 27]. Others, such as TSP and the PEDF, inhibit pathological neovascular processes [21-26]. PEDF, similarly to bFGF, has a neurotrophic action on photoreceptors. Some factors, such as EGF, act on Müller cells inducing endogenous bFGF transcription and strengthen the protective action of these cells on the retina nerve cells; EGF also stimulates ADSCs to increase their secretory activity [30, 29].
To the best of our knowledge, bFGF, IGF-1, PEDF, PDGF, TGF-β, and VEGF are normally secreted by RPE but in the presence of maculopathy with atrophic evolution they are pathologically deficient due to the involution of RPE/choriocapillaris system. Their paracrine secretion by cell graft helps to promote photoreceptor and choriocapillaris survival [2, 32, 33]. Moreover, M-CSF, GM-CSF, and IL have both an anti-inflammatory and chemotactic action on macrophages which contribute to the removal of intraretinal cell debris and to the function normally carried out by RPE [34, 35].
From the results of our study, LRRT may result, directly and indirectly, in increased choroidal perfusion and greater trophism of the photoreceptors through GF-receptor interactions and stimulation mediated by Müller cells and RPE cells. Subsequently, these events are believed to allow more intense cellular activity as demonstrated by the improvement in electrical activity [4, 19]. It is logically supposed that the bond between cells and GF could be the necessary link in the chain of events responsible for an improvement of VP in dry AMD patients. Obviously, poor tissue cellularity would not allow the desired therapeutic effect due to scarce GF-membrane receptor interactions.
Ultimately, our results allow us to conclude that the technique offers some advantages in providing benefits to patients suffering from dry AMD. Vice versa, the surgical procedures available to date are more complex and only temporarily effective [6-13]. Obviously, our studies also have limits to overcome, such as further validation with a greater number of patients and histopathological findings that could provide scientific evidence for the results. Also a control group will be included in the next research study to exclude a placebo effect.
Therefore, we will continue our studies to provide useful updates to the scientific world on this disease which is responsible for growing disability in the modern world due to aging and will therefore have a growing burden on society.
CONCLUSIONs
Cell therapy by autologous cell graft in the suprachoroidal space according to LRRT seems to afford a functional improvement in retinal residual cells, proportional to their condition, with positive consequences on patient VP. The preliminary reading of OCT may allow rehabilitators and surgeons to plan this type of surgery/therapy in patients with dry AMD. Including in severe cases the contribution of GFs to the residual cells of the retina allows the optimization of rehabilitation and recovery of lost capacity with appropriate magnifying systems.
PATIENTS AND METHODS
The tenets of the Declaration of Helsinki were observed, and written informed consent approval by the Ethics Committee of the Low Vision Academy was obtained.
For this purpose, we included 36 eyes of 25 patients (16 women and 9 men), with an average age of 75.96 years (range from 64 to 84 years of age) affected with dry AMD.
They were identified and enrolled according to several characteristics. The inclusion criteria were:
- Caucasian patients classified as well-nourished;
- age ranging from 64 to 84 years;
- dry AMD diagnosis with SD-OCT, fundus autofluorescence imaging, and angiography in the presence of drusen and irregularities of RPE in at least 1 eye;
- well-preserved extrafoveal areas;
- measurable visual acuity not influenced by lens opacity;
- normal intraocular pressure;
- acceptance of the clinical protocol by signing the informed consent.
The criteria for exclusion from the study due to possible cross interference with the test were as follows:
- patients with signs of exudative AMD;
- myopia or hypermetropy with spherical equivalent of ≥ 6 diopters;
- cataract, chorioretinal and neovascular membrane-associated disorders, macular pucker, uveitis, etc.;
- other ocular disorders, such as glaucoma, optic neuritis, ocular trauma, high refractive errors, etc.;
- insufficient compliance in individuals affected by medical problems, such as hypovitaminoses, multiple sclerosis, epilepsy, Parkinson’s disease, diabetes mellitus, hypertension, vasculitis, renal and hepatic diseases, gastrointestinal malabsorption, hypothyroidism, malignant neoplasias, and other systemic acute or chronic diseases.
The eyes were retrospectively divided into two groups according to RTA: group A in which RTA was less than 250 µm, and group B in which RTA was equal to or greater than 250 µm (Figure 1). For each patient we evaluated the visual acuity for far and near distance at T0. BCVA was measured with ETDRS charts at 4 meters in logMAR and visual acuity for near vision, close-up, in Pts indicating the necessary zoom factor (X). The diagnosis of dry AMD was confirmed by Nidek F10 confocal scanning laser ophthalmoscope (Nidek Inc, Fremont, CA), Cirrus 5000 SD-OCT (Carl Zeiss Meditec AG, Jena, Germany), and Maia 100809 MY (CenterVue S.p.A., Padua, Italy). Therefore, we recorded electrical cell activity through scotopic and photopic ERG (ocular electrophysiology electromedical system, Retimax; C.S.O. S.r.l., Scandicci, Italy) according to the standards set in 2009 by the International Society for Clinical Electrophysiology of Vision (ISCEV) [19].
Fat tissue was collected and purified from the abdominal subcutaneous layer of patients according to the Lawrence and Coleman [20] technique. Briefly, 10 mL of fat tissue was harvested manually from each patient with a 3 mm blunt cannula (Mentor, Santa Barbara, CA) connected to a Luer-LokTM syringe (BD Biosciences, Franklin Lakes, NJ). Pure SVF of fat tissue was separated from blood, fat, oil, and liquid after 3’ of centrifugation at 3200 rpm at 1200 G. For PRP preparation, 8 mL of human peripheral blood was collected in a Regen-BCT tube (RegenKit; RegenLab, Le Mont-sur-Lausanne, CH). The collected blood was centrifuged for 5’ at 1500 G. In the LRRT variant, the following changes were made to increase autologous fat graft survival, to trigger ADSC proliferation in order to promote increased choroidal perfusion, and to obtain a more complete modulation of the action of factors secreted only by fat [15, 17, 19-21].
- The distance between the grafted autologous cells and choroid was reduced by deep sclerectomy to favor the paracrine secretion of the autologous cells into the choroidal flow.
- For the same reason, the area of contact between the stalk and choroid was expanded.
- The suprachoroidal pocket was built to accommodate the graft and saturated with a mixture of ADSCs and SVF obtained according to the Lawrence and Coleman technique [20].
- The adipose pedicle was infiltrated with PRP gel obtained by centrifugation of the blood material, separation of the component, and its platelet degranulation [16].
The details are as follows:
- A deep scleral door of about 5 mm was opened by radial hinge in the infero-temporal quadrant at 8 mm from the limbus. The sclerectomy must be deep enough to allow viewing of the slate color of the choroid.
- Orbital fat was extracted from a gap above the inferior oblique muscle. The extracted pedicle fat must be sufficient to ensure the survival of the vascular scaffold after its location.
- The flap of autologous fat was laid gently on the bed and sutured with choroidal vicryl 6/0 at the proximal edge of the door.
- The scleral flap was then secured to avoid compression on the fat pedicle or on its nutrient vessels.
- The remaining space between the autologous fat graft, choroid, and scleral flaps was saturated with 0.5 cc of SVF, previously prepared with ADSCs by venflon inserted into the scleral pocket.
- Then, the stroma of the peduncle was infiltrated with 1 cc of PRP using a 25-gauge cannula.
Therefore, an autograft consisting of fat cells, ADSCs from SVF, and PRP was obtained.
The functional analysis was then repeated after 180 days. Particularly, we considered BCVA and close-up visus after visual rehabilitation and the necessary magnification factor, retinal sensitivity, PCA, RTA, and ERG activity in both groups.
Statistical Analysis
Student’s t-test was used to compare mean age between the two study groups. Gender distribution was compared by chi square test. In order to take into account multiple eyes for the same patients, a Mixed linear regression model was used to evaluate the difference in this parameter at T0 between the two groups and the variation at T0 and T180, and to compare the mean change between the two groups. A p value of < 0.05 was considered statistically significant. All statistical analyses were performed with STATA 14.0 (Collage Station, Texas, USA).
Abbreviations
ADSCs = adipose-derived stem cells, AFT = autologous fat transplantation, AMD = age-related macular degeneration, BCVA = best corrected visual acuity for far distance, bFGF = basic fibroblast growth factor, BDNF = brain-derived neurotrophic factor, BM = Bruch membrane, CC = choriocapillaris, close up visus = visual acuity for near vision, CNTF = ciliar neurotrophic factor, dB = decibel, EGF = epidermal growth factor, ERG = electroretinogram, ETDRS = early treatment diabetic retinopathy study, G0 = quiescent cell phase, G1 phase = cell entry in the growth phase, GF = growth factor, GM-CSF = granulocyte-macrophage colony-stimulating factor, HGF = hepatocyte growth factor, IGF-1 = insulin-like growth factor-1, IL = interleukin, logMAR = logarithm of the minimum angle of resolution, LRRT = Limoli Retinal Restoration Technique, M-CSF = macrophage colony-stimulating factor, MY = microperimetry, µm = microns, mV = micronVolts, NGF = neural growth factor, NS = not statistically significant, PCA = patient compliance analysis, PDAF = platelet-derived angiogenesis factor, PDGF = platelet-derived grow factor, PEDF = pigment-epithelium-derived factor, Ph = photoreceptors, PlGF = placental growth factor, PLT = Platelets, PRP = platelet rich plasma, Pts = points, RPE = retinal pigment epithelial, RTA = retinal thickness average, SD-OCT = spectral domain-optical coherence tomography, SD = standard deviation, SVF = stromal-vascular fraction, T0 = time before of implantation of cell autograft cells, T180 = time 6 months post implantation of cell autograft, TGF-β = transforming growth factor-β, TSP = thrombospondin, VEGF = vascular endothelial growth factor, VP = Visual Performance.
Conflicts of Interest
No conflicting relationship exists for any author. None of the authors have any proprietary interest in any material or method described in this article. This submission has not been published anywhere previously and it is not simultaneously being considered for any other publication.
REFERENCES
1. Reibaldi M, Longo A, Pulvirenti A, Avitabile T, Russo A, Cillino S, Mariotti C and Casuccio A. Geo-Epidemiology of Age-Related Macular Degeneration: New Clues Into the Pathogenesis. Am J Ophthalmol. 2016; 161:78-93.
2. Bhutto I and Lutty G. Understanding age-related macular degeneration (AMD): relationships between the photoreceptor/retinal pigment epithelium/Bruch’s membrane/choriocapillaris complex. Mol Aspects Med. 2012; 33:295-317.
3. Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001; 119:1417-1436. Erratum in Arch Ophthalmol. 2008; 126:1251.
4. Limoli PG, Vingolo EM, Nebbioso M, Scalinci SZ, Mele L and Limoli C. BCVA Changes after suprachoroidal graft of autologus cells in dry AMD. ARVO Meeting. Denver USA, 3-7 May 2015.
5. Grover S, Murthy RK, Brar VS, Chalam KV. Normative data for macular thickness by high-definition spectral-domain optical coherence tomography (spectralis). Am J Ophthalmol. 2009; 148:266-71.
6. Schwartz SD, Hubschman JP, Heilwell G, Franco-Cardenas V, Pan CK, Ostrick RM, Mickunas E, Gay R, Klimanskaya I and Lanza R. Embryonic stem cell trials for macular degeneration: a preliminary report. Lancet. 2012; 379:713-20.
7. Jin X, Lin T and Xu Y. Stem Cell Therapy and Immunological Rejection in animal models. Curr Mol Pharmacol. 2015 Sep 28. [Epub ahead of print]
8. Daftarian N, Kiani S and Zahabi A. Regenerative Therapy for Retinal Disorders. J Ophthalmic Vis Res. 2010; 5:250-64.
9. Zhang K, Hopkins JJ, Heier JS, Birch DG, Halperin LS, Albini TA, Brown DM, Jaffe GJ, Tao W and Williams GA. Ciliary neurotrophic factor delivered by encapsulated cell intraocular implants for treatment of geographic atrophy in age-related macular degeneration. Proc Natl Acad Sci USA. 2011; 108:6241-5.
10. Sampat KM and Garg SJ. Complications of intravitreal injections. Curr Opin Ophthalmol. 2010; 21:178-83.
11. Filatov VP. Tissue therapy. Med Gen Fr. 1951; 11:3-5.
12. Pelaez O. Retinitis pigmentosa. Cuban experience. Editorial Cientifico Técnica. La Habana, 1997.
13. Meduri R, Scorolli L, Morara M, Scalinci SZ, Greco P and Meduri RA. Effect of basic fibroblast growth factor on the retinal degeneration of B6 (A)- Rperd12/J (retinitis pigmentosa) mouse: a morphologic and ultrastructure study. Annual Meeting, Fort Lauderdale, ARVO 2007 May 3-7.
14. Limoli P, Carpi R, Tassi F, Vingolo E, D’Amato L, Giacomotti E, Solari R and Di Corato R. Adipocities subscleral implant. Growth factors may be considered a new therapy of atrophic retinal pathology? Fort Lauderdale. IOVS. 2011; 52:437.
15. Schaffler A and Buchler C. Concise review: adipose tissue-derived stromal cells-basic and clinical implications for novel cell-based therapies. Stem Cells. 2007; 25:818-82.
16. Anitua E, Pelacho B, Prado R, Aguirre JJ, Sánchez M, Padilla S, Aranguren XL, Abizanda G, Collantes M, Hernandez M, Perez-Ruiz A, Peñuelas I, Orive G, et al. Infiltration of plasma rich in growth factors enhances in vivo angiogenesis and improves reperfusion and tissue remodeling after severe hind limb ischemia. J Control Release. 2015; 202:31-9.
17. Modarressi A. Platlet rich plasma (PRP) improves fat grafting outcomes. World J Plast Surg. 2013; 2:6-13.
18. Lindroos B, Suuronen R and Miettinen S. The Potential of Adipose Stem Cells in Regenerative Medicine. Stem Cell Rev and Rep. 2010. Doi 10.1007/s12015-010-9193-7.
19. Limoli PG, Vingolo EM, Morales MU, Nebbioso M and Limoli C. Preliminary Study on Electrophysiological Changes After Cellular Autograft in Age-Related Macular Degeneration. Medicine. 2014; 93:1-8.
20. Lawrence N and Coleman WP. Liposuction. J Am Acad Dermatol. 2002; 47:105-8.
21. Luo S, Hao L, Li X Yu D, Diao Z, Ren L and Xu H. Adipose tissue-derived stem cells treated with estradiol enhance survival of autologous fat transplants. Tohoku J Exp Med. 2013; 231:101-10.
22. Wang P, Mariman E, Renes J and Keijer J.The secretory function of adipocytes in the physiology of white adipose tissue. J Cell Physiol. 2008; 216:3-13.
23. Anitua E, Andia I, Ardanza B, Nurden P, and Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thrombosis and Haemostasis. 2004; 91:4-15.
24. Qureshi AH, Chaoji V, Maiguel D, Faridi MH, Barth CJ, Salem SM, Singhal M, Stoub D, Krastins B, Ogihara M, Zaki MJ and Gupta V. Proteomic and phospho-proteomic profile of human platelets in basal, resting state: insights into integrin signaling. PLoS One. 2009; 4:e7627.
25. Bagchi M, Kim LA, Boucher J, Walshe TE, Kahn CR, and D’Amore PA. Vascular endothelial growth factor is important for brown adipose tissue development and maintenance. FASEB J. 2013; 27:3257-71.
26. Mammoto T, Jiang A, Jiang E and Mammoto A. Platelet rich plasma extract promotes angiogenesis through the angiopoietin1-Tie2 pathway. Microvasc Res. 2013; 89:15-24.
27. Chen G, Shi X, Sun C, Li M, Zhou Q, Zhang C, Huang J, Qiu Y, Wen X, Zhang Y, Zhang Y, Yang S, Lu L, et al. VEGF-mediated proliferation of human adipose tissue-derived stem cells. PLoS One. 2013; 8:e73673.
28. Sakaguchi DS, Janick LM and Reh TA. Basic fibroblast growth factor (FGF-2) induced transdifferentiation of retinal pigment epithelium: generation of retinal neurons and glia. Dev Dyn. 1997; 209:387-98.
29. Kim SY, Mocanu C, McLeod DS, Bhutto IA, Merges C, Eid M, Tong P and Lutty GA. Expression of pigment epithelium-derived factor (PEDF) and vascular endothelial growth factor (VEGF) in sickle cell retina and choroid. Exp Eye Res. 2003; 77:433-45.
30. Ueki Y and Reh TA. EGF stimulates Müller glial proliferation via a BMP-dependent mechanism. Glia. 2013; 61:778-89.
31. Li Q, Li PH, Hou DJ, Zhang AJ, Tao CB, Li XY and Jin PS. EGF enhances ADSCs secretion via ERK and JNK pathways. Cell Biochem Biophys. 2014; 69:189-96.
32. Rabin DM, Rabin RL, Blenkinsop TA, Temple S and Stern JH. Chronic oxidative stress upregulates Drusen-related protein expression in adult human RPE stem cell-derived RPE cells: a novel culture model for dry AMD. Aging (Albany, NY). 2013; 5:51-66. doi: 10.18632/aging.10516.
33. Kozlowski MR. RPE cell senescence: a key contributor to age- related macular degeneration. Elsevier Med Hypotheses. 2012; 78:505-10.
34. Yin Y, Henzl MT, Lorber B, Nakazawa T, Thomas TT, Jiang F, Langer R and Benowitz LI. Oncomodulin is a macrophage- derived signal for axon regeneration in retinal ganglion cells. Nat Neurosci. 2006; 9:843-52.
35. LaVail MM, Unoki K, Yasumura D, Matthes MT, Yancopoulos GD, Steinberg RH. Multiple growth factors, cytokines, and neurotrophins rescue photoreceptors from the damaging effects of constant light. Proc Natl Acad Sci USA. 1992; 89:11249-53.