
INTRODUCTION
Gastric cardia cancer (GCC) occurs at the top of the stomach, near the junction of the esophagus, and is one of the leading causes of cancer-related death worldwide. There are two distinct types of GCC, one type being located in the more distal stomach as a consequence of atrophic gastritis, and the other type resembling esophageal adenocarcinoma, which is likely to be a consequence of short-segment gastro-esophageal reflux disease [1, 2]. Earlier studies demonstrate the incidence of the gastric cardia cancer to be 4% to 10% per year [3]. However, the mechanisms for the development of GCC have not been well-demonstrated up to now. The Chaoshan region has one of the highest incidences of esophageal cancer and GCC,with age-standardized incidence rates for GCC in the Chaoshan area being 34.81/100,000 [4], which suggests unique environmental/genetic factors involved in GCC pathogenesis.
Helicobacter pylori (H. pylori) gastric infection has been reported to be the main risk factor in gastric cardia cancer [5]. H. pylori is a gram-negative bacterium that is adapted to survive in the human stomach microenvironment. It is estimated that H. pylori infects more than half of the human population [6]. H. pylori can activate the host immune response, thus leading to chronic gastritis and ulcers. A small number of patients may develop gastric cancer, after long-term H. pylori infection, through mechanisms demonstrated in previous reports [7-11]. One mechanism involves H. pylori-mediated generation offree radicals to lead to increasesin gene mutations. Another mechanism involves H. pylori-induced pro-inflammatory genes, such as interleukin-6 and TNF-α, which are highly expressed in H. pylori-infected tissues [12]. These factors can alter gastric epithelial cell adhesion and lead to the dispersion and migration of mutated epithelial cells [13]. However, other mechanisms need to be explored.
Caudal-related homeobox transcription factor 2 (CDX2) is an intestinal transcription factor that has been reported toregulate cell differentiation, proliferation and apoptosis in normal cells [14]. Previous studies have shown that CDX2 expression is limited not only to normal intestinal cells, but also is expressed in gastric carcinoma, colorectal cancer, thyroid cancer, ovarian cancer, urinary bladder carcinoma and prostate adenocarcinoma [15-19]. Moreover, H. pylori infection induces abnormal expression of CDX2 in the gastric mucosa [20], suggesting a possible role for CDX2 in gastric cardia. However, the expression of CDX2 in gastric cardia and its correlation with H. pylori infection has not been clearly demonstrated. In this paper, we use immunohistochemistry and Giemsa staining to detect the of and determine the correlation between CDX2, Ki67 and H. pylori infection in a large cohort of GCC patients and non-malignant cardia mucosa to explore new mechanisms by which H. Pylori infection promotes GCC carcinogenesis.
RESULTS
CDX2 expression in gastric cardia specimens
To identify the expression of CDX2 in non-malignant gastric cardia and GCC specimens, we performed CDX2 immunohistochemical staining in a cohort of patient samples. CDX2 expression was mostly found in cell nuclei, and the staining intensity was scored as strong, weak and negative (Figure 1A). Of the 83 non-malignantgastric cardiatissues examined, there was no detectable CDX2 in 7 normal gastric cardia cases. In the remaining 76 gastric carditis cases, CDX2 was negative in 66 cases and positive in 10 cases (13.2%), including 4 CDX2-strong cases and 6 CDX2-weak cases. The immunohistochemical resultsshowed that inflamed epithelia had various expression levels of CDX2 in non-malignant gastric cardia mucosa (Figure 1B). Normal epithelia without inflammation had the no detectable CDX2, but negative/weak CDX2 staining was observed in epithelial cells accompanied by mild to severe inflammation (Figure 1C) (Table 1).
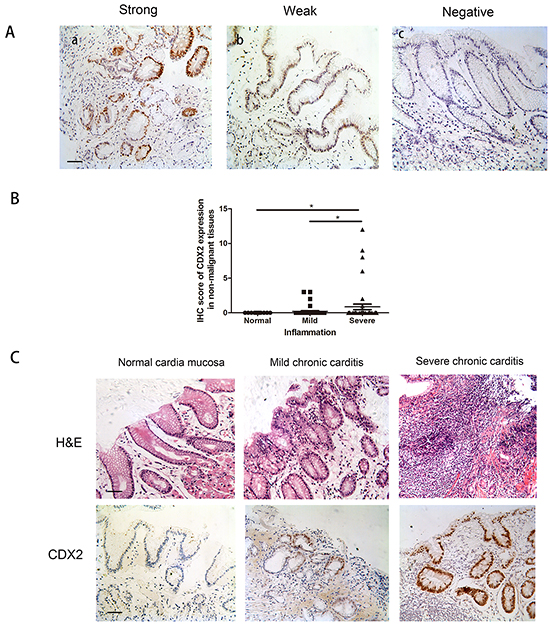
Figure 1: CDX2 expression in non-malignant gastric cardia tissues. A. Variable levels of CDX2 were detected by immunohistochemistry in a small number of non-malignant gastric cardia tissues. Analysis was based on nuclear staining. Patient samples were categorized into strong (a), weak (b) and negative (c) (IHC stain, scale bar, 50 μm). B. Boxplot shows that the IHC score for CDX2,at different inflammation levels, shows that CDX2 expression was significantly higher in the severe inflammation cases involving normal tissues. C. Gastric cardia epithelial cases were stained with hematoxylin and eosin (H&E) and immunohistochemistry. Variable expression levels of CDX2 were detected for different severities of inflammation (IHC stain, scale bar, 50 μm) (*p<0.05).
Table 1: Correlation between CDX2 protein expression and clinicopathological parameters in 76 gastric carditis cases
Clinical parameter |
Case |
CDX2 expression |
P-value |
||
|---|---|---|---|---|---|
Negative |
Positive |
||||
Age |
<54 |
35 |
32 |
3 |
|
≥54 |
41 |
34 |
7 |
p=0.326 |
|
Gender |
Male |
43 |
37 |
6 |
|
Female |
33 |
29 |
4 |
p=1.000 |
|
Inflammation |
+ |
30 |
30 |
0 |
|
++ |
20 |
16 |
4 |
||
+++ |
26 |
20 |
6 |
p=0.023* |
|
*p<0.05
In 60 GCC cases, CDX2 expression was detectable in half of the cases 32/60 (53.3%),with 17/60 (18.3%) cases considered as CDX2-strong staining,and 15/60 (25.0%) cases considered as CDX2-weak staining (Figure 2A). Expression of CDX2 in the remaining 28 cases was negative. Moreover, the strong CDX2 staining was found in GCC cases with severe inflammation, whereas the weak or negative CDX2 staining was detected in the non-inflamed GCC samples (Figure 2B and 2C) (Table 2). Expression of CDX2 was significantly higher in GCC tissues than in non-malignant gastric cardia (Figure 2D). These results led us to hypothesize that CDX2 activation is a key mediatorof gastric cardia epithelial inflammation.
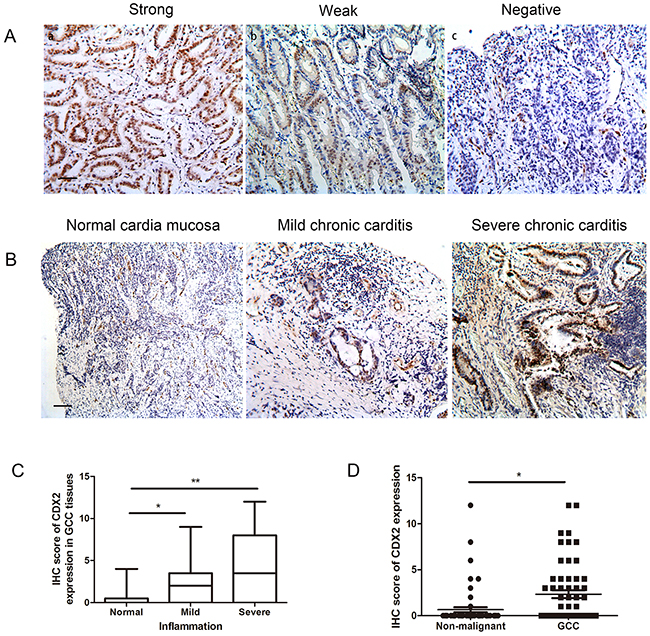
Figure 2: CDX2 expression in GCC tissues. A. Variablelevels of CDX2 were detected by IHC in half of the GCC tissues. Patient samples were categorized into strong (a), weak (b) and negative (c) (IHC stain, scale bar, 50 μm). B. Variable expression levels of CDX2 were detected at different severities of inflammation (IHC stain, scale bar, 100 μm). C. Boxplot shows that IHC scoresfor CDX2 were significantly higher in the severe GCC inflammation cases than the non-inflammation cases. D. Boxplot shows that CDX2 expression was higher in the GCC cases compared to the non-malignant cases (*p<0.05, **p<0.01).
Table 2: Correlation between CDX2 protein expression and clinicopathological parameters in 60 GCC samples
Clinical parameter |
Case |
CDX2 expression |
P-value |
||
|---|---|---|---|---|---|
Negative |
Positive |
||||
Age |
≤62 |
29 |
13 |
16 |
|
>62 |
31 |
15 |
16 |
p=0.802 |
|
Gender |
Male |
52 |
24 |
28 |
|
Female |
8 |
4 |
4 |
p=1.000 |
|
Differentiation |
High |
2 |
0 |
2 |
|
Mild |
28 |
11 |
17 |
||
poor |
30 |
17 |
13 |
p=0.173 |
|
Invasion |
T1-T2 |
40 |
16 |
24 |
|
T3-T4 |
20 |
12 |
8 |
p=0.176 |
|
Lymph node |
Yes |
37 |
22 |
15 |
|
metastasis |
No |
23 |
6 |
17 |
p=0.017* |
Inflammation |
+ |
15 |
12 |
3 |
|
++ |
25 |
10 |
15 |
||
+++ |
20 |
6 |
14 |
p=0.010* |
|
*p<0.05
Clinical significance of CDX2 expression in GCC
We then assessed whether CDX2 expression correlated with clinical parameters, such as age, gender and inflammation stage in the non-malignant gastric cardia cohort. As shown in Table 1, CDX2 expression correlated with the severity of inflammation in non-malignant gastric cardia patients (p=0.023, chi-square).
We then examined the correlation between CDX2 expression and clinical and pathological parameters, such as gender, size of the tumor, lymph node metastasis, histological grade, depth of tumor invasion and metastasis in the GCC patient samples (Table 2). GCC patients with strong CDX2 expression had a higher incidence of lymphatic metastasis and severity of inflammation (p=0.017 and p=0.010, respectively). There was no significant correlation between the expression of CDX2 andother clinical and pathological parameters in GCC. To further detect the correlation between CDX2 expression and lymph node metastasis, we divided the GCC patients into several subgroups, based on the site and number of metastatic lymphatic nodes. However, we did not find a significant correlation between either the number or site of lymph node metastases and CDX2 expression (Supplementary Table S1).
Correlation between CDX2 expression and H. pylori infection
H. pylori infection has been shown to induce CDX2 expression in gastric cell lines [11]. Keeping this in mind, we hypothesized that CDX2 correlates with the severity of H. pylori infection in gastric cardia tissues. Thus, we determined the extent of H. pylori infection by Giemsa staining in the same cohort of non-malignant gastric cardia and GCC specimens. H. pylori was found in the mucous and gland epithelium in gastric carditis specimens and GCC nest (Figure 3A). The severity of H. pylori infection was divided into normal, mild and severe according to the Sydney system. The expression of CDX2 paralleled the severity of H. pylori infection from normal to severe infection in non-malignant gastric cardia and GCC patient cohort (Figure 3B). The cases with severe H. pylori infectionhadhigher CDX2 expression compared to cases with normal or mild H. pylori infection, suggesting a potential correlation with H. pylori infection and CDX2 expression in the gastric cardia cells.
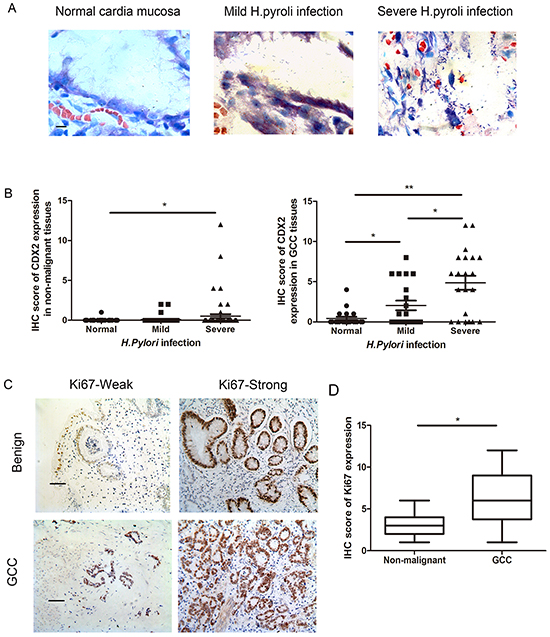
Figure 3: H. pylori infection and Ki67 expression in patient samples. A. H. pylori infection was identified by Giemsa staining and the bacterial density was graded according to the Updated Sydney System. (Giemsa stain, scale bar, 5 μm). B. Boxplot shows that IHC scoresfor CDX2 were significantly higher in the severe H. pylori infection cases than the cases with no or mild H. pylori infection in both non-malignant gastric cardia and GCC tissues. C. IHC staining of Ki67 in non-malignant gastric cardia and GCC tissues (IHC stain, scale bar, 50 μm). All cases were divided into weak and strong subgroups. D. Boxplot shows that the expression of Ki67 is higher in GCC compared to the non-malignant cardia cases (IHC stain, scale bar, 50 μm) (*p<0.05, **p<0.01).
Correlation between CDX2 expression and cell proliferation in GCC patients
To identify the correlation between CDX2 expression and cell proliferation, we quantified expression of Ki67 in the same cohort of patient samples (Table 3). Ki67 is abiomarkerfor proliferating cells. Immunohistochemical staining detected Ki67 in all non-malignant gastric cardia tissues and GCC patient samples (Figure 3C). All GCC patients’ samples were divided into Ki67-weak (n= 29) and Ki67-strong (n= 31) subgroups and non-malignant samples were categorized into Ki67-weak(n= 43) and Ki67-strong(n= 40) subgroups.
Table 3. Correlation between CDX2 and Ki67 in non-malignant and GCC patient samples
Ki67 expression |
CDX2 expression by IHC in non-malignance samples |
P-value |
||
|---|---|---|---|---|
Negative |
Weak |
Strong |
||
Weak |
37 |
4 |
2 |
|
Strong |
36 |
2 |
2 |
p=0.754 |
Ki67 expression |
CDX2 expression by IHC in GCC |
P-value |
||
|---|---|---|---|---|
Negative |
Weak |
Strong |
||
Weak |
18 |
7 |
4 |
|
Strong |
10 |
8 |
13 |
p=0.031* |
Expression of Ki67 was higher in GCC than innon-malignant gastric cardia epithelial tissues (Figure 3D). Moreover, in GCCsamples, increased Ki67 staining in gastric cardia tissues correlated with increased CDX2 expression. The strongest immunostaining of Ki67 was observed in tumors with the highest expression level of CDX2.
DISCUSSION
In this study, we used a cohort of gastric cardia tissues to detect the correlation between CDX2 and H. pylori infection, as well as inflammation and cell proliferation. We found that CDX2 is detectable in most GCC tissues and only a small set of non-malignant gastric cardia tissues. CDX2 expression is significantly higher in GCC tissues compared to non-malignant gastric cardia mucosa samples, indicating that CDX2 is up-regulated in the GCC tumorigenesis. In addition, CDX2 expression significantly correlates with the severity of inflammation in benign cardia samples and lymphatic metastasis in GCC samples,as well as the level of cell proliferation, suggesting that H.pylori infection may induce CDX2 expression in GCC cells, providing pathological evidence that H.pylori infection promotes GCC carcinogenesis.
Gastric cardia is a narrow circular zone between the esophagus and stomach, which also involves a transition from esophageal squamous epithelia to gastric mucosa. The unique location results in GCC involving both the stomach and the esophagus. Previous reports show that GCC has different characteristics from adenocarcinomas arising in the remainder of the stomach, including various risk factors and clinicopathologic characteristics, as well as alterations in gene expression [22-25]. However, most gastric cancer studies do not distinguish GCC from gastric non-cardia cancer.
CDX2 is a transcription factor that induces the transcription of target genes associated with intestinal epithelial differentiation. In normal tissue cells, CDX2 performs various important biological functions, such as cell differentiation, cell growth and cell death, especially in intestinal epithelial cells [18]. Recent studies have revealed that CDX2 is aberrantly expressed in gastric cancer, colorectal cancer, thyroid cancer, ovarian cancer, endometrial adenocarcinoma, bladder and prostate adenocarcinoma [26, 27].
H.pylori, a gram-negative spiral bacteria, is the most common pathogen and affects two of three populationsin the world [28]. H.pylori infectionmay lead to changes in the stomach environment and causeseveral diseases, such as atrophic gastritis, intestinal metaplasia, and gastric cancer. Complex mechanisms involve the induction of the major virulence factors cytotoxin-associated gene A (CagA) and vacuolating cytotoxin A (VacA) [29], which can damage the gastric mucosa and cause inflammation and cell death. The inflammatory response induced by H. pylori infection leads G cells to secrete the hormone gastrin, which stimulates more acid to destroy the stomach mucosa [30]. Most studies have demonstrated H. pylori is an important risk factor of non-cardia gastric adenocarcinoma. However, in our previous paper, we performed a combined analysis of a large cohort of GCC patient samples,from the Chaoshan area,to additionally demonstrate an association between H. pylori infection and risk of cardia gastric cancer, [3]. In Chaoshan, 81.5% of GCC tumors are infected with H. pylori, which is significantly higher than the 59% incidence of tumor infection in GCC patients in other parts of China [31], suggesting H. pylori infection correlates with the risk of cardia gastric cancer. However, this conclusion is not without controversy due to some studies describing an inverse relationship between H. pylori infection and gastric cardia cancer, especially in Western countries [32, 33].
The correlation between H. pylori and CDX2 expression has been demonstrated in several published papers, but conclusionshave been contradictory [34-49]. In in-vivo studies, researchers have demonstrated that CDX2 expression is significantly higher in H. pylori-positive cases than H. pylori-negative intestinal metaplasia patients, whereas others found that CDX2 signaling is much higher in H. pylori-negative patients than positive patients [34, 35]. More convincing evidence has been obtained in a 6-year follow-up study, where researchers found that CDX2 expression in the antrum is lower after eradication of H. pylori infection [36-40]. However, the expression of CDX2 in gastric epithelial cells did not disappear after eradication of H. pylori in other patient cohorts [41-46]. The difference may relateto the length of follow-up, as well as unique patient characteristics. Another potential reason is intestinal metaplasia degradation is a long-term process and that inflammation could continue even after H. pylori eradication. In invitro experiments, H. pylori infection induces CDX2 expression in the AGS gastric carcinoma cell line, but not in other cell lines [47]. All the above results indicate that H. pylori infection induces CDX2 expression in gastric cells [48, 49].
MATERIALS AND METHODS
ESCC tumor samples
We collected 60 consecutive gastric cardiacarcinoma samples and 83 non-malignant gastric cardia mucosa at the First Affiliated Hospital of Shantou between 2005 and 2012. All patients underwent potentially curative surgery without preoperative chemotherapy or radiotherapy. For each patient, tumor-surrounding non-malignant tissue (within 2 cm of the tumor) and distant non-malignant tissue (more than 5 cm away from tumor) were also analyzed. In the GCC cohort, 52 were men and 8 were women; the age range was 43-78 years, with a median of 62 years. In the non-malignant gastric cardia cohort,49 were men and 34 were women; the age was 22-77 years, with a median of 54 years. This study was approved by the ethical review committees of the Medical College of Shantou University. All participants involved in our study gave informed consent.
Immunohistochemistry (IHC)
IHC staining was performed using the Envision Labeled Peroxidase System (Dako, Carpinteria, CA). Consecutive 4 μm-thick slices from each sample were deparaffinized in dimethyl benzene, rehydrated through a graded ethanol series and incubated with fresh 3% H2O2 for 10 min to quench endogenous peroxidase activity. After a rinse in phosphate-buffered saline (PBS), antigen retrieval was performed by microwave heating. Following incubation in 10 mmol/l citrate buffer (pH 6.0) for 20min, sections were incubated with primary antibodies for CDX2(Cell Signaling, 1:100), and Ki67 (Cell Signaling, 1:1000) at 4°C overnight. After washing, the corresponding secondary antibody (DAKO) was added for incubation at 37°C for 30 min before reaction with diaminobenzidine and counterstaining with haematoxylin. Images were captured using a Leica IM50 microscope (Imagic Bildverarbeitung AG, Wetzlar, Germany) at ×400. IHC staining was examined by two pathologists who were blinded to the clinical outcome, and a high degree of concordance between two pathologists was indicated by an inter-rater agreementkappa value of 0.903.
Scoring for CDX2and Ki67 immunostaining was performed similarly. Thus, the percentage of positive cells in each case was categorized as: 0 (<5% positive cells), 1+ (6% to 25%), 2+ (26% to 50%), 3+ (51% to 75%) or 4+ (> 75%). Staining intensity was categorized as 0 to 3+. Final scores were based on the multiplication of the percentage and intensity scores, and ranged from 0 to 12. Tumors were considered weak when they were assigned a score of 0 to 4, whereas tumors were considered strong if they had a final score of ≥6.
Chronic inflammation grading
Inflammation ingastric cardia specimens was assessed as normal, mild and severe according to the updated Sydney System [21]. Normal gastric mucosa contains only individual (0-5)scattered inflammatory cells (mononuclear cells) in the lamina propria. However, any increase indicates chronic gastritis. Mild inflammation involving gastric mucosal mononuclear leukocytes in the lamina propria was viewed as a maximum of 5 to 30 lymphocytes, plasma cells and macrophages per highpower (×40 objective) microscopic field or, by another approach, 5 to 30 lymphocytes or plasma cells between foveolae (the area in which chronic inflammatory cells are most often found. More than 30 inflammatory cells per fieldwas considered as severe inflammation.
Giemsa staining
For the study, 4 μm-thick sections were deparaffinized in xylene and rehydrated in a descending series of ethanol solutions, and then incubated with 0.5% hydrochloric acid alcohol for 10 min. After washing in distilled water, slides were immersed in Giemsa stain preheated to 58 °C for 4 min, and immediately washed in distilled water. An additional wash in distilled water was performed after treating with 1% glacial acetic acid for 3 s, and then the slides were placed into a 52°C incubator for 30 min. Sections were dehydrated, cleared in xylene, and mounted. The H. pylori level was also determined according to the updated Sydney System, which categorizes infection into normal, mild and severe infection subgroups [21].
Statistical analysis
Statistical analysis was performed with SPSS15.0 software. The correlation between CDX2 and other clinical parameters was evaluated using the chi-square or Student’s t-test. A value of p<0.05 was considered as statistically significant.
CONCLUSION
In this paper, we detect CDX2 expression in GCC, gastric carditis and normal gastric cardia tissue, and demonstrate a correlation with H. pylori infection, as well as cell proliferation. We find that CDX2, a specific gastrointestinally expressed protein, plays an important role in GCC carcinogenesis. CDX2 significantly correlates with H. pylori infection in gastric cardia cells. Our findings provides a new approach to the pathogenesis of cardiac tumors in the further.
CONFLICTS OF INTEREST
There is no conflict of interest.
GRANT SUPPORT
This work was supported by National Nature Science Foundation of China (3124007) and Province self-financing science fund of Guangdong (2015-110).
REFERENCES
1. Wang LD, Zheng S, Zheng ZY, Casson AG. Primary adenocarcinomas of lower esophagus, esophagogastric junction and gastric cardia: inspecial reference to China. World J Gastroenterol. 2003; 9:1156-1164.
2. De Groot KM. Cancer of the oesophagus -- quo vadis? S Afr Med J. 2006; 96:197-8.
3. Zheng T, Mayne ST, Holford TR, Boyle P, Liu W, Chen Y, Mador M, Flannery J. The time trend and ageperiod-cohort effects on incidence of adenocarcinoma of thestomach in Connecticut from 1955–1989. Cancer. 1993; 72:330–340.
4. Su M, Liu M, Tian DP, Li XY, Zhang GH, Yang HL, Fan X, Huang HH, Gao YX. Temporal trends of esophageal cancer during 1995-2004 in Nanao Island, an extremely high-risk area in China. Eur J Epidemiol. 2007; 22:43-8.
5. Goldblum JR, Richter JE, Vaezi M, Falk GW, Rice TW, Peek RM. Helicobacter pylori infection, not gastroesophageal reflux, is the major cause of inflammation and intestinal metaplasia of gastric cardiac mucosa. Am J Gastroenterol. 2002; 97:302-11.
6. Sotoudeh M, Derakhshan MH, Abedi-Ardakani B, Nouraie M, Yazdanbod A, Tavangar SM, Mikaeli J, Merat S, Malekzadeh R. Critical role of Helicobacter pylori in the pattern of gastritis and carditis in residents of an area with high prevalence of gastric cardia cancer. Dig Dis Sci. 2008; 53:27-33.
7. Kamangar F, Qiao YL, Blaser MJ, Sun XD, Katki H, Fan JH, Perez-Perez GI, Abnet CC, Zhao P, Mark SD, Taylor PR, Dawsey SM. Helicobacter pylori and oesophageal and gastric cancers in a prospective study in China. Br J Cancer. 2007; 96:172-176.
8. Limburg P, Qiao Y, Mark S, Wang G, Perez-Perez G, Blaser M, Wu Y, Zou X, Dong Z, Taylor P, Dawsey S. Helicobacter pylori seropositivity and subsite-specific gastric cancer risks in Linxian, China. J Natl Cancer Inst. 2001; 93:226-233.
9. Kikuchi S, Wada O, Nakajima T, Nishi T, Kobayashi O, Konishi T, Inaba Y. Serum anti-Helicobacter pylori antibody and gastric carcinoma among young adults. Research Group on Prevention of Gastric Carcinoma among Young Adults. Cancer. 1995; 75:2789-2793.
10. Lin JT, Wang LY, Wang JT, Wang TH, Yang CS, Chen CJ. A nested case-control study on the association between Helicobacter pylori infection and gastric cancer risk in a cohort of 9775 men in Taiwan. Anticancer Res. 1995; 15:603-606.
11. Kamangar F, Dawsey SM, Blaser MJ, Perez-Perez GI, Pietinen P, Newschaffer CJ, Abnet CC, Albanes D, Virtamo J, Taylor PR. Opposing risks of gastric cardia and noncardia gastric adenocarcinomas associated with Helicobacter pylori seropositivity. J Natl Cancer Inst. 2006; 98:1445-52.
12. Koike T, Ohara S, Inomata Y, Abe Y, Iijima K, Shimosegawa T. The prevalence of Helicobacter pylori infection and the status of gastric acid secretion in patients with gastroesophageal junction adenocarcinoma in Japan. Inflammopharmacology. 2007; 15:61-4.
13. Palli D, Masala G, Del Giudice G, Plebani M, Basso D, Berti D, Numans ME, Ceroti M, Peeters PH, Bueno de Mesquita HB, Buchner FL, Clavel-Chapelon F, Boutron-Ruault MC, et al. CagA+ Helicobacter pylori infection and gastric cancer risk in the EPIC-EURGAST study. Int J Cancer. 2007; 120:859-867.
14. Bai YQ, Miyake S, Iwai T, Yuasa Y. CDX2, a homebox transcripton factor, upregulates transcription of thep21/WAF1/CIP1 gene. Oncogene. 2003; 22:7942-9.
15. Gao N, Kaestner KH. Cdx2 regulates endo-lysosomal function and epithelial cell polarity. Genes Dev. 2010; 24:1295-305.
16. Mallo GV, Soubeyran P, Lissitzky JC, André F, Farnarier C, Marvaldi J, Dagorn JC, Iovanna JL. Expression of the Cdx1 and Cdx2 homeotic genes leads to reduced malignancy in colon cancer-derived cells. J Biol Chem. 1998; 273:14030-6.
17. Hinoi T, Tani M, Lucas PC, Caca K, Dunn RL, Macri E, Loda M, Appelman HD, Cho KR, Fearon ER.Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon. Am J Pathol. 2001; 159:2239-48.
18. Qualtrough D, Hinoi T, Fearon E, Paraskeva C. Expression of CDX2 in normal and neoplastic human colon tissue and during differentiation of an in vitro model system. Gut. 2002; 51:184-90.
19. Kaimaktchiev V, Terracciano L, Tornillo L, Spichtin H, Stoios D, Bundi M, Korcheva V, Mirlacher M, Loda M, Sauter G, Corless CL. The homeobox intestinaldifferentiati on factor CDX2is selectively expressed in gastrointestinal adenocarcinomas. Mod Pathol. 2004; 17:1392-1399.
20. Vauhkonen M, Vauhkonen H, Sipponen P. Helicobacter pylori infection induces a reversible expression of the CDX2 transcription factor protein in human gastric epithelium. Scand J Gastroenterol. 2008; 43:915-21.
21. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and gradingof gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol. 1996; 20:1161-1181.
22. Powell J, McConkey CC. Increasing incidence of adenocarcinoma of the gastric cardia and adjacent sites. Br J Cancer. 1990; 62:440-3.
23. Cameron AJ, Souto EO, Smyrk TC. Small adenocarcinomas of the esophagogastric junction: association with intestinal metaplasia and dysplasia. Am J Gastroenterol. 2002; 97:1375-80.
24. Carneiro F, Chaves P. Pathologic riskfactors of adenocarcinoma of the gastric cardia and gastroesophageal junction. Surg Oncol Clin N Am. 2006; 15:697-714.
25. Odze RD. Pathology of the gastroesophageal junction. Semin Diagn Pathol. 2005; 22:256-65.
26. Olsen J, Espersen ML, Jess P, Kirkeby LT, Troelsen JT. The clinical perspectives of CDX2 expression in colorectal cancer:aqualitative systematic review. Surg Oncol. 2014; 23:167-76.
27. Hong SM, Cho H, Moskaluk CA, Frierson HF Jr, Yu E, Ro JY. CDX2 and MUC2 protein expression in extrahepatic bile ductcarcinoma. Am J Clin Pathol. 2005; 124:361-70.
28. Ishaq S, Nunn L. Helicobacter pylori and gastric cancer: a state of the artreview. Gastroenterol Hepatol Bed Bench. 2015; 8:S6-S14.
29. Ferreira RM, Machado JC, Figueiredo C. Clinical relevance of Helicobacter pylori vacA and cagAgenotypes in gastric carcinoma. Best Pract Res Clin Gastroenterol. 2014; 28:1003-15.
30. de Bernard M, Josenhans C. Pathogenesis of Helicobacter pylori infection. Helicobacter. 2014; 19:11-8.
31. Wang Y, Liu S, Zhang Y, Bi C, Xiao Y, Lin R, Huang B, Tian D, Ying S, Su M. Helicobacter pylori infection and gastric cardia cancer in Chaoshan region. Microbes Infect. 2014; 16:840-4.
32. Sipponen P, Marshall BJ. Gastritis and gastric cancer. Western countries. Gastroenterol Clin North Am. 2000; 29:579-92, v-vi.
33. Deng B, Li Y, Zhang Y, Bai L, Yang P. Helicobacter pylori infection and lung cancer: a review of an emerging hypothesis. Carcinogenesis. 2013; 34:1189-95.
34. GY Song, ZA Gao, HC Lie. Correlation between H pylori infection and CDX2. Jinzhouyixueyuanxuebao. 2005; 26:1-4.(Chinese).
35. FM Xiao, Y Sun, H Tian. CDX2 expression in gastric samples and correlation with H pylori infection. Gastric and liver disease. 2009; 18:550-552.
36. Vauhkonen M, Vauhkonen H, Sipponen P. Helicobacter pylori infection induces a reversible expression of the CDX2 transcription factor protein in human gastric epithelium. Scand J Gastroenterol. 2008; 43:915-21.
37. Uemura N, Mukai T, Okamoto S, Yamaguchi S, Mashiba H, Taniyama K, Sasaki N, Haruma K, Sumii K, Kajiyama G. Effect ofHelicobacter pylori eradication on subsequentdevelopment of cancer after endoscopic resectionof early gastric cancer. Cancer Epidemiol BiomarkersPrev. 1997; 6:639–42.
38. Kuipers EJ, Nelis GF, Klinkenberg-Knol EC, Snel P, Goldfain D, Kolkman JJ, Festen HP, Dent J, Zeitoun P, Havu N, Lamm M, Walan A. Eradicationof Helicobacter pylori reverses intestinalmetaplasia in patients with severe atrophic gastritis. Gastroenterology. 1997; 112:A142.
39. Sung JJ, Lin SR, Ching JY, Zhou LY, To KF, Wang RT, Leung WK, Ng EK, Lau JY, Lee YT, Yeung CK, Chao W,Chung SC. Atrophy andintestinal metaplasia one year after cure ofH. pylori infection: a prospective, randomizedstudy. Gastroenterology, 2000; 119:7-14.
40. Correa P, Fontham ET, Bravo JC, Bravo LE, Ruiz B, Zarama G, Realpe JL, Malcom GT, Li D, Johnson WD, Mera R. Chemoprevention of gastric dysplasia: randomizedtrial of antioxidant supplements and antiHelicobacter pylori therapy. J Natl Cancer Inst. 2000; 92:1881-8.
41. Satoh K, Mutoh H, Eda A, Yanaka I, Osawa H, Honda S, Kawata H, Kihira K, Sugano K. Aberrant expression of CDX2 in the gastric mucosa with and without intestinal metaplasia: effect of eradication of Helicobacter pylori. Helicobacter. 2002; 7:192-8.
42. Tucci A, Poli L, Tosetti C, Biasco G, Grigioni W, Varoli O, Mazzoni C, Paparo GF, Stanghellini V, Caletti G. Reversal of fundic atrophy after eradication of Helicobacter pylori. Am J Gastroenterol. 1998; 93:1425-31.
43. Satoh K, Kimura K, Takimoto T, Kihira K. A follow-upstudy of atrophic gastritis and intestinal metaplasiaafter eradication of Helicobacter pylori. Helicobacter. 1998; 3:236–40.
44. Annibale B, Aprile MR, Caruana P, Bordi C, Fave D. Cure of Helicobacter pylori infection inatrophic body gastritis patients does not improvemucosal atrophy but reduces hypergastrinemiaand its related effects on body ECL-cell hyperplasia.Aliment Pharmacol Ther. 2000; 14:625-34.
45. Weston AP, Topalovski M, Cherian R, Dixon A. Prospective 5-year follow-up of gastric intestinalmetaplasia following cure of H. pylori using anextensive gastric mucosal bioptic mapping protocol. Gastroenterology. 1998; 114:A703.
46. Kim N, Lim SH, Lee KH, Choi SE, Jung HC, Song IS, Kim CY. Long-term effectsof Helicobacter pylori eradication on intestinalmetaplasia in patients with duodenal and benigngastric ulcers. Dig Dis Sci, 2000; 45:1754-62.
47. Genta RM, Lew GM,Graham DY. Changes in the gastricmueosafolowing eradication of Helieobaeter pylori. ModPathol, 1993; 6:281-289.
48. Matsuda K, Yamauchi K, Matsumoto T, Sano K, Yamaoka Y, Ota H. Quantitative analysis of the effect of Helicobacter pylori on the expressions of SOX2, CDX2, MUC2, MUC5AC, MUC6, TFF1, TFF2, and TFF3 mRNAs in human gastric carcinoma cells. Scand J Gastroenterol. 2008; 43:25-33.
49. Barros R, Marcos N, Reis CA, De Luca A, David L, Almeida R. CDX2 expression is induced by Helicobacter pylori in AGS cells. Scand J Gastroenterol. 2009; 44:124-5.