
INTRODUCTION
Cutaneous melanoma is the fifteenth most common cancer in world, with more than 120,000 new cases diagnosed in 2015 [1]. It has long been recognized as a potentially aggressive form of skin cancer [2]. Despite many advances in the diagnosis, adjuvant therapy, and even targeted therapy of this disease, the prognosis for cutaneous melanoma remains poor. Several prognostic factors of OS and MSS with cutaneous melanoma have been identified in previous studies, such as tumor site, Breslow thickness, and ulceration, including sentinel lymph node biopsy (SLNB) [3, 4]. SLNB can detect micro-metastasis in the regional lymph node and is a powerful tool in the staging of cutaneous melanoma and is recommended in patients with thick Breslow depth. Until now, a few studies have proven the clinical value of SLNB; current treatment for cutaneous melanoma without metastasis is wide local excision and SLNB [5–7]. Moreover, SLNB for staging purposes is recommended by the American Joint Committee on Cancer (AJCC) Melanoma Staging Committee for all patients with primary tumors > 1 mm in Breslow thickness [8].
In this study, we aimed to evaluate the clinical usefulness of SLNB and to discuss the prognostic value of sentinel lymph node status for patients with cutaneous melanoma by using cutaneous melanoma data from the Surveillance, Epidemiology, and End Results (SEER) cancer-registry program of individuals diagnosed between 2004 and 2012.
RESULTS
Patient baseline characteristics
Between 2004 and 2012, a total of 56,285 eligible patients were identified with a new diagnosis of cutaneous melanoma with Breslow thickness greater than 1 mm during the 8-year period, including 34,466 male (61.2%) and 21,819 (38.8%) female patients. Median age was 63 years and median Breslow thickness was 1.50 mm. Lesions in 13,071 cutaneous melanoma patients were situated on the head and neck, 17,351 situated on the trunk, and 25,703 patients had lesions situated on extremities. In this study, nodular melanoma (NM) and superficial spreading melanoma (SSM) were the most common histotypes. Breslow thickness were between 1–2 mm in the majority of melanomas. The flowchart of the study population is shown in Figure 1 and the characteristics of cutaneous melanoma patients are listed in Table 1.
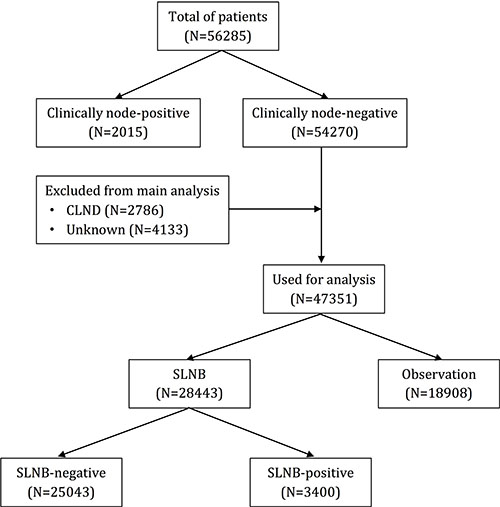
Figure 1: Flowchart of the study population.
Table 1: Characteristics of 56285 patients with cutaneous melanoma
Characteristics |
Total of patients (N = 56285) |
Clinical node-negative (N = 47351) |
SLNB (N = 28443) |
|||
|---|---|---|---|---|---|---|
Clinical node-positive (N = 2015) |
Clinical node-negative (N = 54270) |
Observation (N = 18908) |
SLNB (N = 28443) |
SLNB-positive (N = 3400) |
SLNB-negative (N = 25043) |
|
Gender |
|
|
|
|
|
|
male |
1409 |
33057 |
11650 |
17012 |
2107 |
14905 |
female |
606 |
21213 |
7258 |
11431 |
1293 |
10138 |
Age (y) |
|
|
|
|
|
|
≤ 60 |
990 |
23788 |
5907 |
14448 |
1897 |
12551 |
> 60 |
1025 |
30482 |
13001 |
13995 |
1503 |
12492 |
Primary site |
|
|
|
|
|
|
head/neck |
424 |
12647 |
5996 |
4999 |
454 |
4545 |
trunk |
697 |
16654 |
5328 |
9129 |
1323 |
7806 |
extremities |
885 |
24818 |
7507 |
14268 |
1618 |
12650 |
unknown |
9 |
151 |
77 |
47 |
5 |
42 |
Histotype |
|
|
|
|
|
|
Superficial spreading |
316 |
14667 |
5027 |
8024 |
869 |
7155 |
nodular |
659 |
8175 |
2434 |
4544 |
849 |
3695 |
desmoplastic |
27 |
1411 |
525 |
718 |
24 |
694 |
lentiginous |
88 |
2630 |
1191 |
1126 |
155 |
971 |
other/unknown |
925 |
27387 |
9731 |
14031 |
1503 |
12528 |
Breslow depth (mm) |
|
|
|
|
|
|
1–2 |
502 |
35477 |
12714 |
17714 |
1206 |
16508 |
2–4 |
549 |
11434 |
3190 |
6811 |
1183 |
5628 |
≥ 4 |
964 |
7359 |
3004 |
3918 |
1011 |
2907 |
Ulceration |
|
|
|
|
|
|
yes |
1175 |
13266 |
4152 |
7035 |
1476 |
5559 |
no |
794 |
39354 |
14173 |
20579 |
1868 |
18711 |
unknown |
46 |
1650 |
583 |
829 |
56 |
773 |
SLN status
According to the flowchart of the study population, 2,015 patients (3.6%) presented with a positive clinical lymph node and underwent therapeutic lymph node dissection. 54,270 patients (96.4%) presented with clinically-negative lymph nodes and were excluded. Therapy information was unknown in patients who underwent completion lymph node dissection (CLND) despite having clinically negative SNB. Ultimately, 47,351 patients were used for analysis in this study. In these patients, SLNB was performed in 28,443 patients (60.1%), 3,400 patients presented with positive SLN and 25,043 patients presented with negative SLN (12% SLN positive rate). The remaining 18,908 patients underwent lymph node observation.
Survival analysis
A total of 12,688 patients (24.1%) died during follow-up, and in these patients, 6,039 patients (47.6%) died of melanoma and 6,649 patients (52.4%) died of other diseases. Median follow-up time was 37.0 months. Patients who presented with clinically-positive lymph nodes had significantly shorter OS (46.1% vs 78.6%, p < 0.001, Figure 2A) and MSS (55.8% vs 90.5%, p < 0.001, Figure 2B) compared with patients who no clinical lymph nodes present. Patients who underwent SLNB had significantly longer 5-year survival rate for OS (84.3% vs 70.1%, p < 0.001, Figure 2C) and MSS (91.5% vs 90.3%, p < 0.001, Figure 2D) compared with patients who did not undergo SLNB (i.e., those who underwent lymph node observation). Patients with a negative SLNB had a significantly longer 5-year survival rate for OS (86.5% vs 68.1% vs 46.1%, p < 0.001, Figure 2E) and MSS (93.7% vs 75.1% vs 55.8%, p < 0.001, Figure 2F) than patients who were SLNB-positive and had clinical lymph node-positive disease.
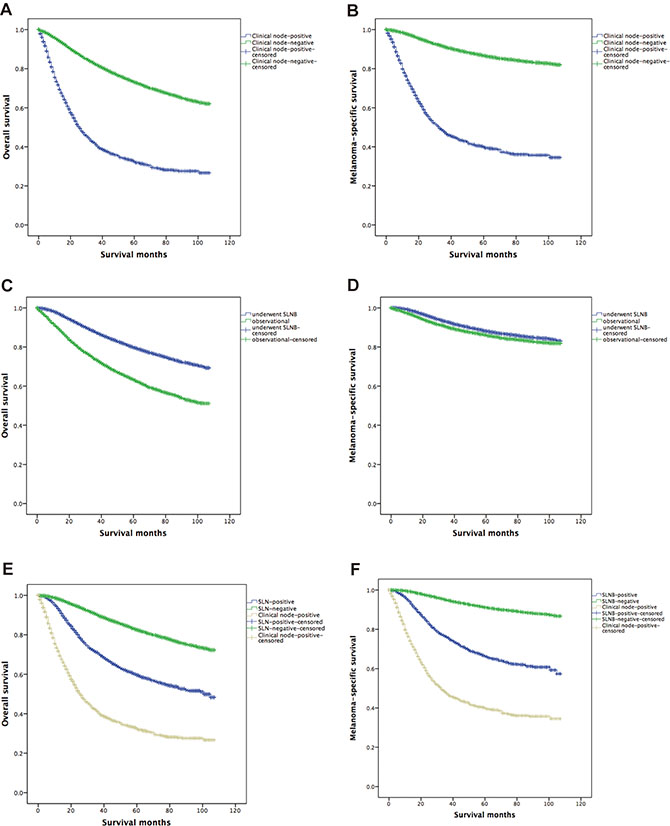
Figure 2: Kaplan-Meier curves are shown for overall survival and melanoma-specific survival. Clinically positive indicates patients with clinically positive regional disease at the time of presentation who underwent therapeutic lymph node dissection; SLN, sentinel lymph node.
Univariate and multivariate analyses
Multivariate analysis showed that age (HR 1.896, 95% CI: 1.227–1.908, P < 0.001), primary site (HR 3.487, 95% CI: 2.125–4.009, P < 0.001), histotype (HR 1.843, 95% CI: 1.565-1.994, P < 0.001), Breslow depth (HR 1.453, 95% CI: 1.182-2.346, P < 0.001), ulceration (HR 2.367, 95% CI: 2.002–2.874, P < 0.001), status of clinical node (HR 1.236, 95% CI: 0.992–8.223, P < 0.001), and status of SLN (HR 1.083, 95% CI: 0.865–1.853, P < 0.001) were independent risk factors for OS. These factors were also independent prognostic factors associated with MSS. Tables 2 and 3 shows the risk factors related to OS and MSS.
Table 2: Univariate and multivariate analyses of factors associated with overall survival in patients with cutaneous melanoma
Factor |
Univariate |
Multivariate |
||
|---|---|---|---|---|
HR (95% CI) |
P |
HR (95% CI) |
P |
|
Gender |
1.675 (0.830–1.648) |
0.134 |
|
NI |
Age |
1.541 (1.332–1.609) |
< 0.001 |
1.896 (1.227–1.908) |
< 0.001 |
Primary site |
3.221 (1.088–4.632) |
< 0.001 |
3.487 (2.125–4.009) |
< 0.001 |
Histotype |
1.062 (0.364–1.323) |
< 0.001 |
1.843 (1.565–1.994) |
< 0.001 |
Breslow depth |
1.341 (1.118–2.165) |
< 0.001 |
1.453 (1.182–2.346) |
< 0.001 |
Ulceration |
2.112 (1.988–2.427) |
< 0.001 |
2.367 (2.002–2.874) |
< 0.001 |
Status of clinical node |
0.965 (0.898–4.756) |
< 0.001 |
1.236 (0.992–8.223) |
< 0.001 |
Status of SLN |
1.043 (0.853–2.442) |
< 0.001 |
1.562 (1.439–2.880) |
< 0.001 |
NI: not included in the multivariate survival analysis.
Table 3: Univariate and multivariate analyses of factors associated with melanoma-specific survival in patients with cutaneous melanoma
Factor |
Univariate |
Multivariate |
||
|---|---|---|---|---|
HR (95% CI) |
P |
HR (95% CI) |
P |
|
Gender |
1.973 (1.335–2.876) |
0.378 |
|
NI |
Age |
1.673 (1.556–1.923) |
< 0.001 |
0.987 (0.665–1.632) |
< 0.001 |
Primary site |
3.887 (1.231–5.443) |
< 0.001 |
1.689 (1.124–3.887) |
< 0.001 |
Histotype |
0.875 (0.586–1.545) |
< 0.001 |
1.778 (1.345–2.334) |
< 0.001 |
Breslow depth |
1.122 (0.893–1.883) |
< 0.001 |
1.086 (0.993–1.446) |
< 0.001 |
Ulceration |
1.776 (1.013–2.006) |
< 0.001 |
2.157 (1.884–3.432) |
< 0.001 |
Status of clinical node |
0.778 (0.582–3.112) |
< 0.001 |
1.187 (0.698–5.963) |
< 0.001 |
Status of SLN |
0.931 (0.845–1.975) |
< 0.001 |
1.083 (0.865–1.853) |
< 0.001 |
NI: not included in the multivariate survival analysis.
DISCUSSION
SLN helps to predict the outcome of melanoma, and also allows clinicians to decide which patient may skip a completion lymphadenectomy and thus reduce morbidity. The status of the sentinel lymph node has been identified an important prognostic factor for cutaneous melanoma patients [9]. However, until now, there have not been large-sample clinical trials that have demonstrated this conclusion in overall survival or Melanoma-specific survival with the use of SLNB. Despite this, SLNB has become standard practice and has been recommended for clinically localized cutaneous melanoma with Breslow thickness between 1–4 mm and without metastasis [6, 10].
To our knowledge, a large prospective randomized trial named MSLT-I has evaluated cutaneous melanoma patients with clinically-negative lymph nodes who underwent SLNB while others were observed [3, 4]. The results showed that the prognostic significance of SLNB with five-year melanoma survival was 72% for SLN-positive patients compared to 90% survival for SLN-negative patients. Therefore, SLN status is a useful predictor of OS and MSS for patients with Breslow thickness between > 1 mm and without metastasis [10, 11].
According to previous studies, SLNB will detect nodal metastases in approximately 15–22% of cases in clinical lymph node-negative patients [12, 13]. These patients usually undergo completion lymphadenectomy and may be eligible for adjuvant therapy. The remaining 80–85% of patients with SLN-negative disease in general have a good prognosis: 5-year DFS is 88–90% and OS is 93% [14, 15]. SLNB has replaced radical regional lymph node dissection as a staging procedure with less morbidity. The SLN procedure is 95–98% accurate in staging the regional node basin and identifies the 15–20% of patients with nodal metastasis who require a complete lymph node dissection [16].
Until now, the status of sentinel lymph node helps to predict the outcome of melanoma. However, up to data, there is no large samples of clinical trials have demonstrated this conclusion in overall survival or Melanoma-specific survival with the use of SLNB. Therefore, the primary aim of this present study was to evaluate SLNB in patients with thick, clinically lymph node-negative melanoma to provide the relative value of SLNB by using large sample size of data from SEER database. The results showed that patients who performed SLNB had significantly longer OS and MSS compared with patients with did not undergo SLNB (lymph node observation). Patients with a negative SLNB had significantly longer OS and MSS than the patients who were SLNB-positive or clinically lymph node-positive.
This current study used the SEER database to investigate the value of SLNB and confirmed the prognostic role of SLNB for patients who were clinically lymph node-negative without metastasis. However, it still had several potential limitations. First, the SEER database lacks information on postoperative adjuvant therapy or target therapy in patients with cutaneous melanoma. Second, the survival outcomes of SLNB-positive patients with Breslow thickness > 4 mm is still unclear. Patients with thick melanoma have a higher risk of developing distant metastatic and guidelines suggested that SLNB “may be recommended”. Therefore, early control of regional disease may not impact survival [8].
In conclusion, this study shows that SLN status is a valuable prognostic factor in patients with Breslow thickness greater than 1 mm, clinically lymph node-negative cutaneous melanoma. Despite these potential limitations, SLNB is still recommended in patients with thick Breslow depth and without metastasis.
MATERIALS AND METHODS
Study population and data extracted
We used the SEER*Stat software to search for patients who were diagnosed with melanoma between 2004 and 2012 with a known SLNB status. The SEER Cancer Statistics Review (http://seer.cancer.gov/data/citation.html), a report on the most recent cancer incidence, mortality, survival, prevalence, and lifetime risk statistics, is published annually by the Data Analysis and Interpretation Branch of the National Cancer Institute, USA. The current SEER database consists of 17 population-based cancer registries that represent approximately 28% of the population of the United States. It contains no identifiers and is widely used for studies of the correlation between SLNB and OS or MSS information of patients with cutaneous melanoma.
In our study, we divided cutaneous melanoma patients into two groups according to clinical status of lymph nodes: (1) Clinically-positive nodes (2015); and (2) Clinically-negative nodes (54270). In clinically-negative node patients, they were further divided into two subgroups: (1) patients who underwent SLNB (28,443) and (2) observation group (18,908). Depending on the results of the SLNB, they were subsequently stratified into three groups: (1) SLNB-positive (3,400); (2) SLNB-negative (25,043); and (3) SLNB not performed (observation group, 18,908).
Statistical analysis
The characteristics of cutaneous melanoma patients were extracted from the SEER database, including age, gender, tumor site, and Breslow thickness. Kaplan-Meier analyses were used to compare between groups by log-rank test. Survival outcomes of risk factors were analyzed by Multivariable Cox regression models for cutaneous melanoma patients. Statistical analyses were performed using the statistical software package SPSS for Windows, version 18.0 (SPSS Inc, Chicago, IL). All CIs were stated at the 95% confidence level. P values < 0.05 were considered statistically significant.
ACKNOWLEDGMENTS AND FUNDING
The authors acknowledge the efforts of the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER database. The interpretation and reporting of these data are the sole responsibility of the authors.
CONFLICTS OF INTEREST
None of the authors have any conflicts of interest to declare.
Authors’ contributions
JC, HYZ and YQS conceived and designed the study. JC and YX performed the analyses. JC and YX prepared all figures and tables. JC wrote the main manuscript. All authors reviewed the manuscript.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A: Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87–108.
2. Siegel RL, Miller KD, Jemal A: Cancer statistics, 2016. CA Cancer J Clin. 2016; 66:7–30.
3. Morton DL, Thompson JF, Cochran AJ, Mozzillo N, Nieweg OE, Roses DF, Hoekstra HJ, Karakousis CP, Puleo CA, Coventry BJ, Kashani-Sabet M, Smithers BM, Paul E, et al. Group M: Final trial report of sentinel-node biopsy versus nodal observation in melanoma. The New England journal of medicine. 2014; 370:599–609.
4. Morton DL, Thompson JF, Cochran AJ, Mozzillo N, Elashoff R, Essner R, Nieweg OE, Roses DF, Hoekstra HJ, Karakousis CP, Reintgen DS, Coventry BJ, Glass EC, et al. Group M: Sentinel-node biopsy or nodal observation in melanoma. The New England journal of medicine. 2006; 355:1307–1317.
5. Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, Storm FK, Foshag LJ, Cochran AJ: Technical details of intraoperative lymphatic mapping for early stage melanoma. Archives of surgery. 1992; 127:392–399.
6. Murali R, Haydu LE, Quinn MJ, Saw RP, Shannon K, Spillane AJ, Stretch JR, Thompson JF, Scolyer RA: Sentinel lymph node biopsy in patients with thin primary cutaneous melanoma. Annals of surgery. 2012; 255:128–133.
7. Mozzillo N, Pennacchioli E, Gandini S, Caraco C, Crispo A, Botti G, Lastoria S, Barberis M, Verrecchia F, Testori A: Sentinel node biopsy in thin and thick melanoma. Annals of surgical oncology. 2013; 20:2780–2786.
8. Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Atkins MB, Byrd DR, Buzaid AC, Cochran AJ, Coit DG, Ding S, Eggermont AM, Flaherty KT, Gimotty PA, et al. Final version of 2009 ajcc melanoma staging and classification. Journal of clinical oncology. 2009; 27:6199–6206.
9. Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, Cascinelli N, Urist M, McMasters KM, Ross MI, Kirkwood JM, Atkins MB, Thompson JA, Coit DG, et al. Prognostic factors analysis of 17,600 melanoma patients: Validation of the american joint committee on cancer melanoma staging system. Journal of clinical oncology. 2001; 19:3622–3634.
10. Yamamoto M, Fisher KJ, Wong JY, Koscso JM, Konstantinovic MA, Govsyeyev N, Messina JL, Sarnaik AA, Cruse CW, Gonzalez RJ, Sondak VK, Zager JS: Sentinel lymph node biopsy is indicated for patients with thick clinically lymph node-negative melanoma. Cancer. 2015; 121:1628–1636.
11. Wong SL, Balch CM, Hurley P, Agarwala SS, Akhurst TJ, Cochran A, Cormier JN, Gorman M, Kim TY, McMasters KM, Noyes RD, Schuchter LM, Valsecchi ME, et al. American Society of Clinical O,Society of Surgical O: Sentinel lymph node biopsy for melanoma: American society of clinical oncology and society of surgical oncology joint clinical practice guideline. Journal of clinical oncology. 2012; 30:2912–2918.
12. Berk DR, Johnson DL, Uzieblo A, Kiernan M, Swetter SM: Sentinel lymph node biopsy for cutaneous melanoma: The stanford experience, 1997-2004. Archives of dermatology. 2005; 141:1016–1022.
13. McMasters KM, Wong SL, Edwards MJ, Ross MI, Chao C, Noyes RD, Viar V, Cerrito PB, Reintgen DS: Factors that predict the presence of sentinel lymph node metastasis in patients with melanoma. Surgery. 2001; 130:151–156.
14. Yee VS, Thompson JF, McKinnon JG, Scolyer RA, Li LX, McCarthy WH, O'Brien CJ, Quinn MJ, Saw RP, Shannon KF, Stretch JR, Uren RF: Outcome in 846 cutaneous melanoma patients from a single center after a negative sentinel node biopsy. Annals of surgical oncology. 2005; 12:429–439.
15. Zogakis TG, Essner R, Wang HJ, Foshag LJ, Morton DL: Natural history of melanoma in 773 patients with tumor-negative sentinel lymph nodes. Annals of surgical oncology. 2007; 14:1604–1611.
16. Morton DL: Overview and update of the phase iii multicenter selective lymphadenectomy trials (mslt-i and mslt-ii) in melanoma. Clinical & experimental metastasis. 2012; 29:699–706.