The aim was to test the feasibility of using cell-free DNA to support evaluation of treatment response, pseudo-progression and whether progression could be found before clinical and/or radiologic progression.
Cf DNA fluctuated during treatment with the highest levels before diagnostic surgery and at progression.
An increase was seen in 3 out of 4 patients at the time of progression while no increase was seen in 3 out of 4 patients without progression.
Dr. Dorte Schou Nørøxe from the Department of Radiation Biology as well as the Department of Oncology at Rigshospitalet in Copenhagen, Denmark said "Glioblastoma (GB) is a highly malignant brain tumor with limited treatment options. With standard treatment, median overall survival (OS) is 16–22 months"
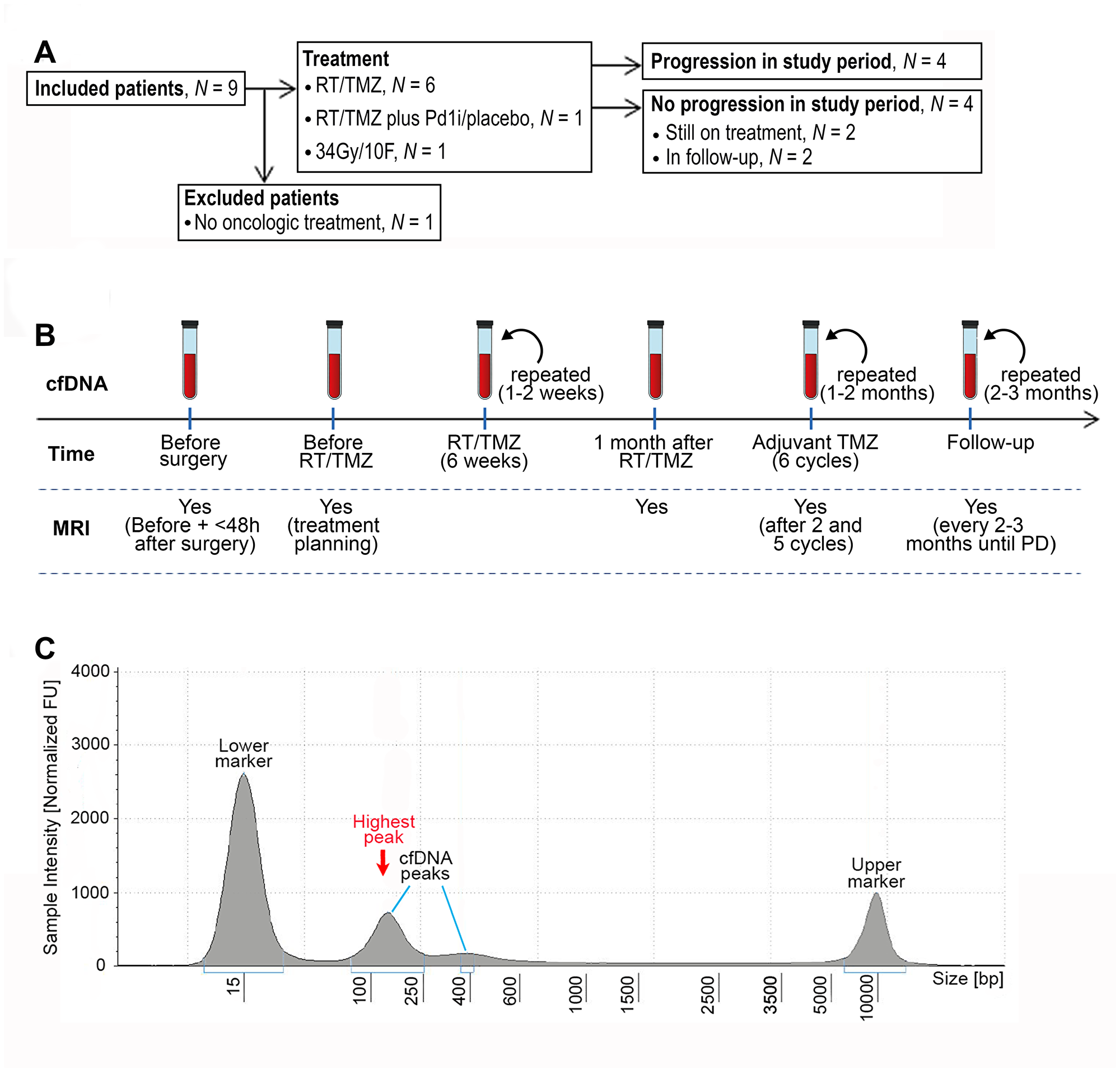
Figure 1: CONSORT diagram, workflow and example of fragment size analysis. (A) CONSORT diagram of included patients. Abbreviations: RT/TMZ: radiotherapy/Temozolomide (concurrent RT/TMZ plus adjuvant TMZ); RT/TMZ plus PD1i/placebo: (concurrent RT/TMZ plus Programmed Death1 inhibitor/placebo followed by adjuvant TMZ plus PD1i/placebo). (B) Illustration of work flow. First sample was taken the day before or on the day of diagnostic surgery. If the diagnosis of glioblastoma was confirmed, the next sample was taken one month after surgery at first visit to the oncologic department, every 1–2 weeks during RT/TMZ, throughout the adjuvant TMZ with 1–2 months interval and in the follow-up period with approximately 2–3 months interval until progressive disease (PD). Magnetic resonance imaging (MRI) was performed before surgery, ≤48 hours after surgery, for treatment planning of RT/TMZ, one month after RT/TMZ, after two and five cycles of adjuvant TMZ and then every 2-3 months until progression. (C) An example of a result from the fragment analysis assessed using the Tape Station instrument. CfDNA fragments were visualized using a higher and lower ladder as reference, respectively. The peak of the curve with the highest % of fragments, was defined as the highest peak.
Another more accessible tumor source is circulating cell-free DNA and specifically circulating tumor DNA.
The fraction of ct DNA in cancer patients accounts for 3 93% of the total cf DNA, thus cf DNA can be used as a surrogate marker of tumor activity/burden.
Elevated cf DNA levels have been detected in patients with severe brain injury which is proof-of-principle that cf DNA is shed from the brain to the blood stream during cell degradation and ct DNA has been detected in patients with brain cancer.
In this study, the authors aimed to test the feasibility of detecting cf DNA in patients with GB and to investigate if cf DNA fluctuations could support evaluation of treatment response, pseudo-progression and whether progression could be found before clinical and/or radiologic progression.
The Nørøxe Research Team concluded, "Several studies have shown that increased levels of a specific mutation in the blood can be found significantly earlier than a radiologic or clinical progression and IDH R132H mutation, TERT promotor mutation, and MGMT promotor methylation has been detected in brain cancer."
Full text - https://doi.org/10.18632/oncotarget.27030
Correspondence to - Dorte Schou Nørøxe - [email protected]
Keywords - glioblastoma, liquid biopsy, cell-free DNA, fragment length, base-pair